A. B. JANDAGHI ET AL. 419
negative predictive value in tibial arteries than for other
sectors [13]. In our study, good agreement was achieved
in all below the knee arterial segments (k ≥ 0.75; P <
0.0001); however, lower agreement was noted for
proximal segments of anterior tibialis and peroneal arter-
ies (k = 0.77 and 0.75, respectively). Also, distal portion
of SFA in Hunter canal was difficult to be evaluated. So,
we used convex probe to overcome the poor view of this
arterial segment. Nevertheless, the lowest agreement (k =
0.72) in our study was related to this segment. Although
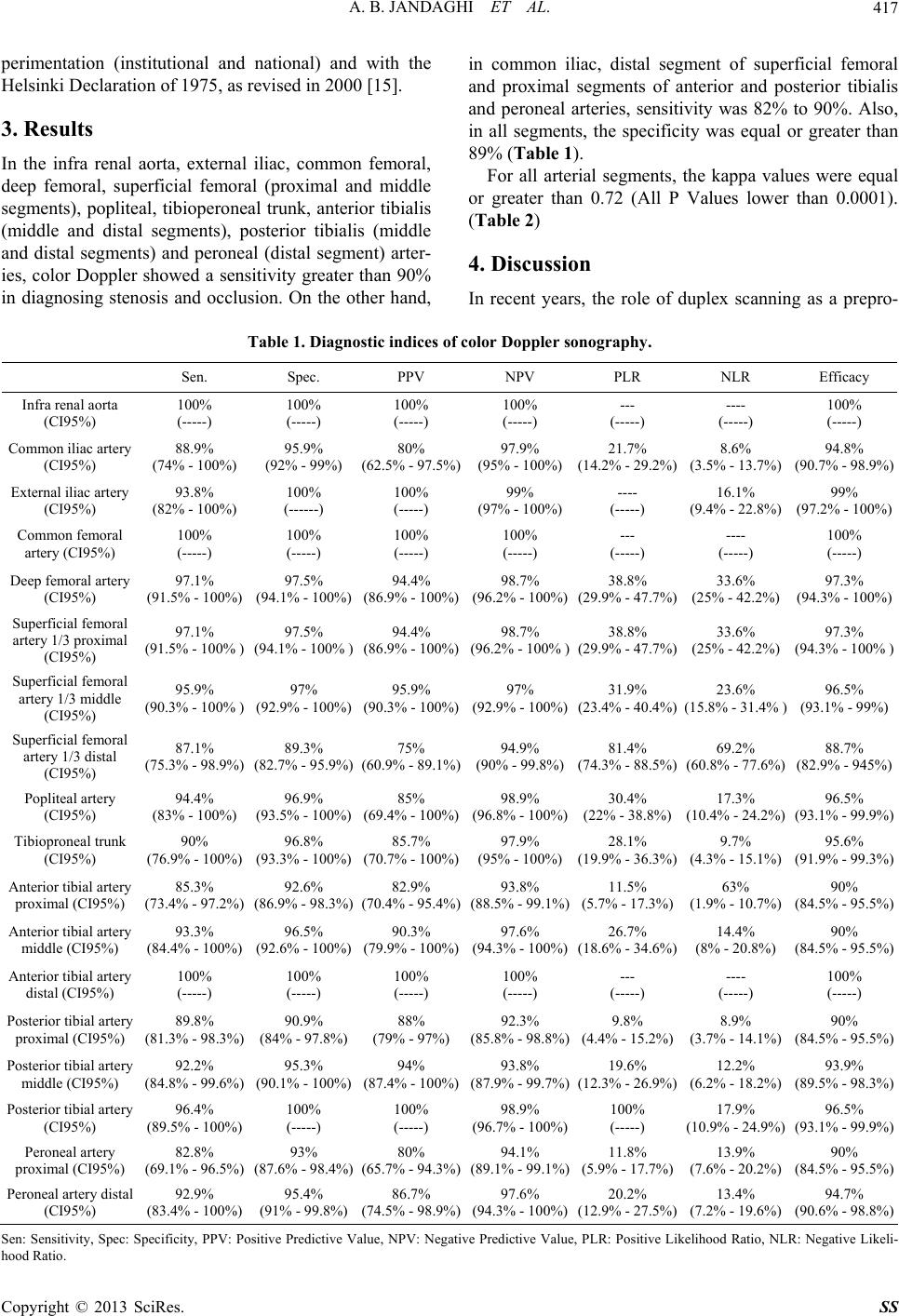
duplex scanning has lower sensitivity and specificity in
distal segment of superficial femoral and proximal seg-
ments of anterior and posterior tibialis and peroneal ar-
teries (Table 1), it is effective for drawing arterial map-
ping and further clinical decision making.
The arterial mapping in our study helped our vascular
surgeon to be ready for possible interventional proce-
dures such as need for stenting or angioplasty at the same
time of diagnostic DSA angiography. This resulted in
less patient’s costs and necessity for second interven-
tional angiography. Moreover, the patients were satisfied
by one step intervention.
5. Conclusion
In conclusion, this study suggests that considering excel-
lent capability of color Doppler sonography in the
evaluation of lower extremity arterial disease, color
Doppler arterial mapping is sufficient for decision mak-
ing in treatment of these patients and can reduce the rate
of diagnostic angiography.
REFERENCES
[1] K. A. Jager, D. J. Phillips, R. L. Martin, et al., “Noninva-
sive Mapping of Lower Limb Arterial Lesions,” Ultra-
sound in Medicine and Biology, Vol. 11, No. 3, 1985, pp.
515-521.
http://dx.doi.org/10.1016/0301-5629(85)90164-4
[2] T. R. Kohler, D. R. Nance, M. M. Cramer, et al., “Duplex
Scanning for Diagnosis of Aortoiliac and Femoropopliteal
Disease: A Prospective Study,” Circulation, Vol. 76, No.
5, 1987, pp. 1074-1080.
http://dx.doi.org/10.1161/01.CIR.76.5.1074
[3] B. L. Thiele and D. E. Strandness Jr., “Accuracy of An-
giographic Quantification of Peripheral Atherosclerosis,”
Progress in Cardiovascular Diseases, 1983, Vol. 26, No.
3, pp. 223-236.
http://dx.doi.org/10.1016/0033-0620(83)90007-5
[4] H. B. Slot, L. Strijbosch and J. M. Greep, “Interobserver
Variability in Single-Plane Aortography,” Surgery, Vol.
90, No. 3, 1981, pp. 497-503.
[5] M. Pemberton, S. Nydahl, T. Hartshorne, et al., “Can
Lower Limb Vascular Reconstruction Be Based on Color
Duplex Imaging Alone?” European Journal of Vascular
& Endovascular Surgery, Vol. 12, No. 4, 1996, pp. 452-
454. http://dx.doi.org/10.1016/S1078-5884(96)80013-X
[6] B. H. Elsman, D. A. Legemate, F. H. van der Heijden, et
al., “Impact of Ultrasonographic Duplex Scanning on
Therapeutic Decision Making in Lower-Limb Arterial
Disease,” British Journal of Surgery, Vol. 82, No. 5, 1995,
pp. 630-633.
[7] C. G. Koshy, B. R. Chacko and S. N. Keshava, “Diagnos-
tic Accuracy of Color Doppler Imaging in the Evaluation
of Peripheral Arterial Disease as Compared to Digital
Subtraction Angiography,” Vascular Disease Manage-
ment, Vol. 6, No. 1, 2009, pp. 2-9.
[8] E. Favaretto, C. Pili, A. Amato, et al., “Analysis of
Agreement between Duplex Ultrasound Scanning and
Arteriography in Patients with Lower Limb Artery Dis-
ease,” Journal of Cardiovascular Medicine, Vol. 8, No. 5,
2007, pp. 337-341.
http://dx.doi.org/10.2459/01.JCM.0000268124.51543.b2
[9] A. Krnic, N. Vucic and Z. Sucic, “Duplex Scanning Com-
pared with Intra-Arterial Angiography in Diagnosing Pe-
ripheral Arterial Disease: Three Analytical Approaches,”
Vasa, Vol. 35, No. 2, 2006, pp. 86-91.
http://dx.doi.org/10.1024/0301-1526.35.2.86
[10] S. Aly, K. Sommerville, M. Adiseshiah, et al., “Com-
parison of Duplex Imaging and Arteriography in the
Evaluation of Lower Limb Arteries,” British Journal of
Surgery, Vol. 85, No. 8, 1998, pp. 1099-1102.
http://dx.doi.org/10.1046/j.1365-2168.1998.00786.x
[11] T. Leiner, A. G. Kessels, P. J. Nelemans, et al., “Periph-
eral Arterial Disease: Comparison of Color Duplex US
and Contrast-Enhanced MR Angiography for Diagnosis,”
Radiology, Vol. 235, 2005, pp. 699-708.
http://dx.doi.org/10.1148/radiol.2352040089
[12] J. F. Polak, M. I. Karmel, J. A. Mannick, et al., “Deter-
mination of the Extent of Lower-Extremity Peripheral
Arterial Disease with Color-Assisted Duplex Sonography:
Comparison with Angiography,” American Journal of
Roentgenology, Vol. 155, No. 5, 1990, pp. 1085-1089.
http://dx.doi.org/10.2214/ajr.155.5.2120939
[13] J. Fontcuberta, A. Flores, A. Orgaz, M. Doblas, J. Gil, I.
Leal, R. Rodriguez, J. Maria and M. Dolores, “Reliability
of Preoperative Duplex Scanning in Designing a Thera-
peutic Strategy for Chronic Lower Limb Ischemia,” An-
nals of Vascular Surgery, Vol. 23, No. 5, 2009, pp. 577-
582. http://dx.doi.org/10.1016/j.avsg.2008.07.011
[14] G. K. Chiramel, R. C. Binita, N. K. Shyamkumar, S.
Edwin and A. Sunil, “Decision Making in the Treatment
of Peripheral Arterial Disease—A Single-Institution
Comparative Study Using Information from Color Dop-
pler and Digital Subtraction Angiogram Studies,” Indian
Journal of Radiology and Imaging, Vol. 21, No. 4, 2011,
pp. 294-297. http://dx.doi.org/10.4103/0971-3026.90694
[15] World Medical Association, “Declaration of Helsinki-
Ethical Principles for Medical Research Involving Human
Subjects,” 2012.
http://www.wma.net/en/30publications/10policies/b3/inde
x.html
[16] A.-M. Löfberg, S. Karacagil, A. Hellberg, A. Boström, C.
Ljungman and G. Östholm, “The Role of Duplex Scan-
ning in the Selection of Patients with Critical Lower-Limb
Ischemia for Infrainguinal Percutaneous Transluminal
Copyright © 2013 SciRes. SS