 International Journal of Clinical Medicine, 2013, 4, 395-399 http://dx.doi.org/10.4236/ijcm.2013.49071 Published Online September 2013 (http://www.scirp.org/journal/ijcm) 395 Psychosocial Factors for Women Reques ting Cesarean Section Yajuan Zhao1, Shuangyun Chen2* 1Department of Obstetric and Gynecology, Taihe Hospital, Hubei Medical College, Shiyan, China; 2Department of Obstetric and Gynecology, Taihe Hospital, Yunyang Medical College, Shiyan, China. Email: zhaoyajuan609@sohu.com, *873729453@qq.com Received June 26th, 2013; revised July 31st, 2013; accepted August 10th, 2013 Copyright © 2013 Yajuan Zhao, Shuangyun Chen. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Background: Rates of caesarean section are progressively increasing in many parts of the world. As a result of psy- chosocial factors, there has been an increasing tendency for pregnant women without justifiable medical indications for caesarean section to ask for this procedure in China. The psychosocial factors for requesting cesarean section were ana- lyzed in our study. Methods: A self-made questionnaire and the State-Trait Anxiety Inventory (STAI) and Self-rating Depression Scale (SDS) were administered to evaluate lying-in women’s psychosocial state. Results: The proportion of lying-on women’s age and education degree was different significantly between the two groups (p < 0.01). In the study groups, the proportion of lying-on women who were in lower economic degree and in her first para was markerly higher than control (88.62% vs. 63.24%; 13.32% vs. 3.42%, p < 0.01). In the study groups, the proportion of women who felt fearful, anxious, depressed and lacking confidence was higher than control. The ratio of women with university educa- tion in the CS group was higher than vaginal delivery group. The proportion of lying-on women without correct deliv- ery knowledge was higher than control, but the difference was not significant (p > 0.05). By logistic regression, we found that for primipara, higher education degree, anxiety and lacking confidence were the dangerous factors for cesar- ean, while lower economic degree was a defendant factor. Conclusion: There were five main psychosocial factors such as education degree and economic state, parity, anxiety and confidence of lying-on women affecting the choice of the delivery way. The nulliparous women who feel anxious without confidence in nice economic state, with better educa- tion have higher risk to choose cesarean. Keywords: Cesarean Section; Psychosocial Factor; Delivery Mode; Anxiety; Depression 1. Background Caesarean section (CS) is needed to prevent or treat life- threatening maternal or foetal complications in an esti- mated 5 - 15 percent of pregnancies [1,2]. During the past few decades, CS rates are progressively increasing in many countries, particularly among developing coun- tries such as China [3-5]. The World Health Organization (WHO) Global Survey on Maternal and Perinatal Health reported that in 2007-2008 the overall facility-based CS rate was estimated to be 27.3 percent in Asia with the highest estimate for China at 46.2 percent [6]. During the last 30 years, the cesarean rate in China has risen from 6% in to 30% in 2005 [7-11]. In many Chinese hospitals, the caesarean section rate was more than 40%, while in some cases, it was up to 80%, which was much higher than the acceptable caesarean rate (5% - 15%) in WHO’s guidelines [12]. In recent years, there has been an increasing tendency for pregnant women without obstetric indications for caesarean section to ask for this procedure because they perceive it to be safer and more convenient than vaginal delivery [4,6]. This situation has become a significant factor leading to the increased rate of caesarean section in China [13,14]. Caesarean section on maternal request (CSMR) has been added to this list of indications and considered an important contributing factor in the CS rising rate [15-17]. The latter occurs when a woman asks to schedule a purely planned caesarean section on a date mutually convenient for her and her doctor, before the onset of labour, without any medical rationale, and in the absence of any clinical indication. Women’s preference can be affected by tokophobia *Corresponding autho . Copyright © 2013 SciRes. IJCM 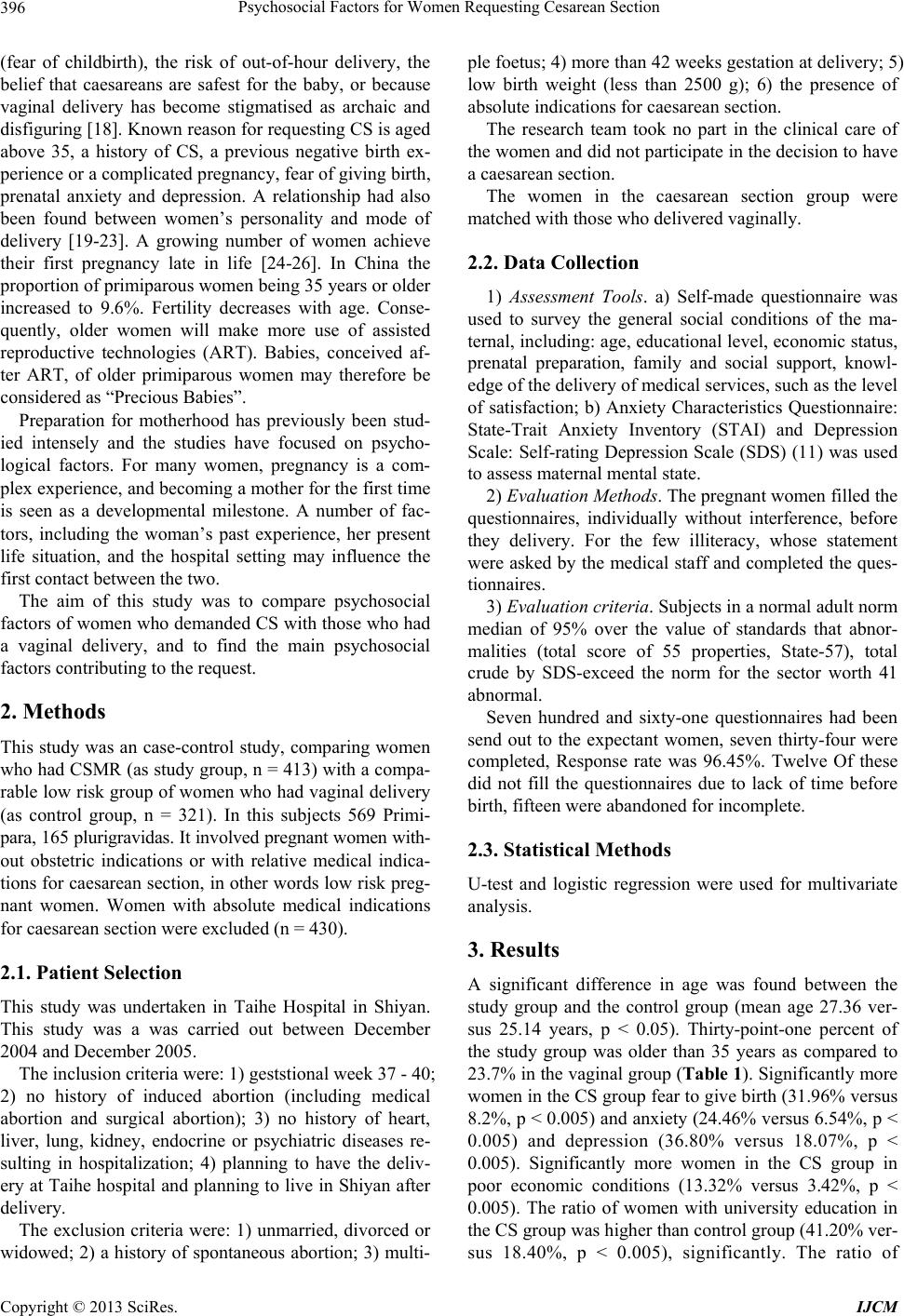 Psychosocial Factors for Women Requesting Cesarean Section 396 (fear of childbirth), the risk of out-of-hour delivery, the belief that caesareans are safest for the baby, or because vaginal delivery has become stigmatised as archaic and disfiguring [18]. Known reason for requesting CS is aged above 35, a history of CS, a previous negative birth ex- perience or a complicated pregnancy, fear of giving birth, prenatal anxiety and depression. A relationship had also been found between women’s personality and mode of delivery [19-23]. A growing number of women achieve their first pregnancy late in life [24-26]. In China the proportion of primiparous women being 35 years or older increased to 9.6%. Fertility decreases with age. Conse- quently, older women will make more use of assisted reproductive technologies (ART). Babies, conceived af- ter ART, of older primiparous women may therefore be considered as “Precious Babies”. Preparation for motherhood has previously been stud- ied intensely and the studies have focused on psycho- logical factors. For many women, pregnancy is a com- plex experience, and becoming a mother for the first time is seen as a developmental milestone. A number of fac- tors, including the woman’s past experience, her present life situation, and the hospital setting may influence the first contact between the two. The aim of this study was to compare psychosocial factors of women who demanded CS with those who had a vaginal delivery, and to find the main psychosocial factors contributing to the request. 2. Methods This study was an case-control study, comparing women who had CSMR (as study group, n = 413) with a compa- rable low risk group of women who had vaginal delivery (as control group, n = 321). In this subjects 569 Primi- para, 165 plurigravidas. It involved pregnant women with- out obstetric indications or with relative medical indica- tions for caesarean section, in other words low risk preg- nant women. Women with absolute medical indications for caesarean section were excluded (n = 430). 2.1. Patient Selection This study was undertaken in Taihe Hospital in Shiyan. This study was a was carried out between December 2004 and December 2005. The inclusion criteria were: 1) geststional week 37 - 40; 2) no history of induced abortion (including medical abortion and surgical abortion); 3) no history of heart, liver, lung, kidney, endocrine or psychiatric diseases re- sulting in hospitalization; 4) planning to have the deliv- ery at Taihe hospital and planning to live in Shiyan after delivery. The exclusion criteria were: 1) unmarried, divorced or widowed; 2) a history of spontaneous abortion; 3) multi- ple foetus; 4) more than 42 weeks gestation at delivery; 5) low birth weight (less than 2500 g); 6) the presence of absolute indications for caesarean section. The research team took no part in the clinical care of the women and did not participate in the decision to have a caesarean section. The women in the caesarean section group were matched with those who delivered vaginally. 2.2. Data Collection 1) Assessment Tools. a) Self-made questionnaire was used to survey the general social conditions of the ma- ternal, including: age, educational level, economic status, prenatal preparation, family and social support, knowl- edge of the delivery of medical services, such as the level of satisfaction; b) Anxiety Characteristics Questionnaire: State-Trait Anxiety Inventory (STAI) and Depression Scale: Self-rating Depression Scale (SDS) (11) was used to assess maternal mental state. 2) Evaluation Methods. The pregnant women filled the questionnaires, individually without interference, before they delivery. For the few illiteracy, whose statement were asked by the medical staff and completed the ques- tionnaires. 3) Evaluation criteria. Subjects in a normal adult norm median of 95% over the value of standards that abnor- malities (total score of 55 properties, State-57), total crude by SDS-exceed the norm for the sector worth 41 abnormal. Seven hundred and sixty-one questionnaires had been send out to the expectant women, seven thirty-four were completed, Response rate was 96.45%. Twelve Of these did not fill the questionnaires due to lack of time before birth, fifteen were abandoned for incomplete. 2.3. Statistical Methods U-test and logistic regression were used for multivariate analysis. 3. Results A significant difference in age was found between the study group and the control group (mean age 27.36 ver- sus 25.14 years, p < 0.05). Thirty-point-one percent of the study group was older than 35 years as compared to 23.7% in the vaginal group (Table 1). Significantly more women in the CS group fear to give birth (31.96% versus 8.2%, p < 0.005) and anxiety (24.46% versus 6.54%, p < 0.005) and depression (36.80% versus 18.07%, p < 0.005). Significantly more women in the CS group in poor economic conditions (13.32% versus 3.42%, p < 0.005). The ratio of women with university education in the CS group was higher than control group (41.20% ver- sus 18.40%, p < 0.005), significantly. The ratio of Copyright © 2013 SciRes. IJCM  Psychosocial Factors for Women Requesting Cesarean Section Copyright © 2013 SciRes. IJCM 397 Table 1. Maternal psychosocial factors compared between the two groups. study group (413) control group (321) χ2 P-value Related Factors n % n % University education 170 41.20 59 18.40 33.86 <0.005 Age > 35 23 5.60 40 5.60 8.48 <0.005 Primiparae 366 88.62 203 63.24 51.76 <0.005 Fear of giving birth 132 31.96 68 21.18 8.20 <0.005 Poor economic conditions 55 13.32 11 3.42 16.74 <0.005 Erroneous understanding of childbirth 224 54.24 156 48.60 1.78 >0.10 Lack of confidence 136 32.93 24 7.48 53.21 <0.005 Depression 152 36.8 58 18.07 24.06 <0.005 Anxiety 101 24.46 21 6.54 32.42 <0.005 primiparae in the study group was significantly more than the control (88.62% versus 63.24, p < 0.005). The women with erroneous understanding of childbirth in the study group was more than the vaginal group (54.24% versus than 48.60% p > 0.1), but not significant. Psychosocial factors for unnecessary cesarean The single factor analysis had shown some psychosocial fac- tors including: maternal age, education level, family economic status, lack of confidence in childbirth, depres- sion and anxiety, was associated with delivery mode. Logistic regression analysis on psychosocial factors for cesarean section Took the mode of delivery as the dependent variable, with maternal age, education level, parity, economic status, fear, anxiety, depression, lack of self-confidence as independent variables. Logistic-re- gression analysis was performed; the variables entered the equation shown in Table 2. 4. Discussion Some studies had shown that the rate of selective cesar- ean section without medical indications were growing, psycho-social factors have become the main reason for it [6,7]. In our study some psycho-social factors such as women’s economic status, education level, parity, the lack of confidence in childbirth, anxiety had associated with cesarean section. A maternal demographic factors The single factor analysis showed that CS had a correlation with the ma- ternal’, education level, economic status, and parity. The women with higher education level more likely request CS. The ratio of women who had university education was higher in the study group than that of the control, while who had primary school education was less than that of the control, significantly. Logistic regression analysis suggested that high qualifications were a risk factors for unnecessary CS. Other study discovered that the younger women with a stable income and higher education level, prefer to give birth with CS; The older with relatively low income and low education prefer to give birth with vaginal delivery [14]. This is consistent with our study results. The reason for this phenomenon was that women with higher education feared to give birth, because the older primiparae age, on the contrary, the women with lower education are often regarded rais- ing children as perfectly justified. The proportion of low economic status women in the CS group was significantly lower than the control group (52.8% vs 83.33%), Logistic regression analysis of com- bined results suggest that low economic status was a protective factors from CS. Worrying about the high cost of CS, the parturient at lower economic status preferred to natural childbirth, in addition, the success rate of trial of labor in this group was higher, because of their physi- cal activity and better tolerance. Primiparous age above 35 years was a known reason for requesting CS [7]. Be- cause women aged between 25 - 35 in this study ac- counted for the majority part, it couldn’t shown statistical significance correlation between women’s age between cesarean section. Maternal psychological factors As one of the four main factors affect the delivery, the impact of maternal psychological factors on childbirth can not be ignored, it affects not only the labor progress but also the choice of delivery mode [14-16]. Severe anxiety of childbirth has been demonstrated in 5% - 10% of pregnancy woman [17]. Maternity is a major physical and psychological stress, the majority of women have varying degrees of mental pressure, severe anxiety and depression occurred, which led to bad feelings increased obstetric complica- tions and cesarean section rates are rising [16,17]. The results had shown that fear of childbirth, lack of confi- dence in childbirth, feelings of depression and anxiety had associated with CS. Logistic regression analysis showed that maternal anxiety and lack of confidence in childbirth must be the main risk factors for CS. Other studies found that maternal erroneous understanding for delivery mode was correlated with increasing rate of CS  Psychosocial Factors for Women Requesting Cesarean Section 398 Table 2. The variables entered the equation and the estimated value of parameters. Variables Regression coefficient Standard error Wald P OR education level 0.386 0.186 4.308 0.038 1.471 Parity 1.892 0.637 8.830 0.003 6.631 Poor economic conditions −1.210 0.471 6.599 0.010 0.298 Fear of giving birth 1.955 0.495 15.586 0.000 0.142 Lack of confidence 2.306 0.641 12.930 0.000 10.038 anxiety 3.551 1.113 10.179 0.001 34.832 Constant −1.367 0.714 3.667 0.055 0.255 [14]. Our study did not support that view. Nevertheless, the investigation did found that some of maternal request CS without any medical indication because the wrong knowledge for delivery, such as, the child delivered by CS are more smart, fear the quality of sexual life decline for relaxation of vaginal after delivery. A small group of people asked optional CS, because they believed that born chrono decided fate. Moreover, for the tense doc- tor-patient relationship, some doctors accommodate there patients in order to avoid risks, it might be another risk for unnecessary CS rate increased. This factor has not been incorporated into the analysis, due to low response rate. 5. Limitation In this study, data concerning women’s health are based on self-report and not clinically confirmed. We did not get enough information about personality, family rela- tionship and the physician-patient relationship. 6. Conclusion Women requesting a CS without a specific medical indi- cation were anxious, lack of confidence, fear of giving birth, primiparity, in higher education level and better economic condition. This finding suggested psychologi- cal counseling and support for women requesting CS, as it may reduce the unnecessary CS. REFERENCES [1] WHO, “Monitoring Emergency Obstetric Care: A Hand- book,” WHO, Geneva, 2009. [2] WHO, “Indicators to Monitor Maternal Health Goals,” WHO, Geneva, 1994. [3] A. P. Betrán, M. Merialdi, J. A. Lauer, W. Bing-Shun, J. Thomas, P. Van Look and M. Wagner, “Rates of Caesar- ean Section: Analysis of Global, Regional and National Estimates,” Paediatric and Perinatal Epidemiology, Vol. 21, No. 2, 2007, pp. 98-113. doi:10.1111/j.1365-3016.2007.00786.x [4] T. Duan, “Present Situation and Some Thoughts of Cae- sarean Section,” Chinese Journal of Practical Gynecol- ogy and Obstetrics, Vol. 24, No. 10, 2008, pp. 721-723. [5] M. R. Festin, M. Laopaiboon, P. Pattanittum, M. R. Ewens, D. J. Henderson-Smart, C. A. Crowther and SEA- OR- CHID Study Group, “Caesarean Section in Four South East Asian Countries: Reasons for, Rates, Associated Care Practices and Health Outcomes,” BMC Pregnancy Childbirth, Vol. 9, 2009, p. 17. doi:10.1186/1471-2393-9-17 [6] P. Lumbiganon, M. Laopaiboon, A. M. Gülmezoglu, J. P. Souza, S. Taneepanichskul, P. Ruyan, D. E. Attygalle, N. Shrestha, R. Mori, D. H. Nguyen, T. B. Hoang, T. Rath- avy, K. Chuyun, K. Cheang, M. Festin, V. Udomprasert- gul, M. J. Germar, G. Yanqiu, M. Roy, G. Carroli, K. Ba-Thike, E. Filatova and J. Villar, “World Health Or- ganization Global Survey on Maternal and Perinatal Health Research Group: Method of Delivery and Preg- nancy Outcomes in Asia: The WHO Global Survey on Maternal and Perinatal Health 2007-2008,” Lancet, Vol. 375, No. 9713, 2010, pp. 490-499. doi:10.1016/S0140-6736(09)61870-5 [7] S. L. Tang, X. Y. Li and Z. C. Wu, “Rising Caesarean Delivery Rate in Primiparous Women in Urban China: Evidence from Three Nationwide Household Health Sur- veys,” American Journal of Obstetrics & Gynecology, Vol. 195, No. 6, 2006, pp. 1527-1532. doi:10.1016/j.ajog.2006.03.044 [8] A. Li and Y. Lan, “Pregnant Women’s Mental Health Status of 2,523 Cases Investigated,” China Practical Gy- necologic and Obstetric, Vol. 19, No. 1, 2003, p. 32. [9] L.-Y. Kuo, B. Q. White and W. Long, “Maternal Psycho- logical Status and the Relationship between Mode of De- livery,” China Practical Gynecol ogic and Obstetric Maga- zine, Vol. 17, No. 5, 2001, p. 2814. [10] I. Wiklund, G. Edman and E. Andolf, “Cesarean on Ma- ternal Request: Reson for the Request, Self-Estimated Health, Expectations, Experience of Birth and Signs of Depression among First-Time Mothers,” Acta Obstetricia et Gynecologica Scandinavica, Vol. 86, No. 4, 2007, pp. 451-456. doi:10.1080/00016340701217913 [11] I. Hilldingsson, I. Radestad, C. Rupertsson, et al., “Few Women wish Tobe Delivered by Caesarean Section,” BJOG: An International Journal of Obstetrics & Gynae- colog, Vol. 109, No. 6, 2002, pp. 618-623. doi:10.1111/j.1471-0528.2002.01393.x [12] World Health Organization, “Appropriate Technology for Birth,” Lancet, Vol. 2, No. 8452, 1985, pp. 436-437. Copyright © 2013 SciRes. IJCM  Psychosocial Factors for Women Requesting Cesarean Section 399 [13] B. S. Wang, L. F. Zhou, L. Zhu, X. L. Gao and E. S. Gao, “Maternal Preference of Delivery Mode and the Causes,” Maternal and Child Health Care of China, Vol. 20, No. 22, 2005, pp. 2920-2924. [14] M. W. Pang, T. N. Leung, T. K. Lau and T. K. Hang Chung, “Impact of First Childbirth on Changes in Wo- men’s Preference for Mode of Delivery: Follow-Up of a Longitudinal Observational Study,” Birth, Vol. 35, No. 2, 2008, pp. 121128. doi:10.1111/j.1523-536X.2008.00225.x [15] B. A. Bettes, V. H. Coleman, S. Zinberg, et al., “Cesarean Delivery on Maternal Request: Obstetrician-Gynecolo- gists’ Knowledge, Perception, and Practice Patterns,” Ob- stetrics and Gynecology, Vol. 109, No. 1, 2007, pp. 57-66. doi:10.1097/01.AOG.0000249608.11864.b6 [16] S. J. Robson, W. S. Tan, A. Adeyemi and K. B. G. Dear, “Estimating the Rate of Cesarean Section by Maternal Request: Anonymous Survey of Obstetricians in Austra- lia,” Birth, Vol. 36, No. 3, 2009, pp. 208-212. doi:10.1111/j.1523-536X.2009.00331.x [17] T. Nilstun, M. Habiba, G. Lingman, R. Saracci, M. Da Frè and M. Cuttini, “Cesarean Delivery on Maternal Re- quest: Can the Ethical Problem Be Solved by the Princi- plist Approach?” BMC Medical Ethics, Vol. 9, 2008, p. 11. doi:10.1186/1472-6939-9-11 [18] S. R. Miesnik and B. J. Reale, “A Review of Issues Sur- rounding Medically Elective Cesarean Delivery,” JOGNN, Vol. 36, No. 6, 2007, pp. 605-615. doi:10.1111/j.1552-6909.2007.00196.x [19] H. Amark and E. L. Ryding, “Women Wishig Tobe De- livered by Cesarean section. Anxiety, Risk-Thing and Shame Common According to A Qualitative Study,” La- kartidningen, Vol. 104, No. 12, 2007, pp. 950-953. [20] L. Anderson, I. Sundstom-Poroma, M. Bixo, et al., “Piont Prevalence of Psychiatric Disorders during the Second Trimester of Pregnancy: A Population Based Study,” American Journal of Obstetrics & Gynecology, Vol. 189, No. 1, 2003, pp. 148-154. doi:10.1067/mob.2003.336 [21] I. Wiklund, G. Edman and E. Andolf, “Personality and Mode of Delivery,” Acta Obstetricia et Gynecologica Scandinavica, Vol. 85, No. 10, 2006, pp. 1225-1230. doi:10.1080/00016340600839833 [22] I. Siklund, G. Edman, C. Larsson, et al., “Personality and Mode of Delivery,” Acta Obstetricia et Gynecologica Scandinavica, Vol. 85, No. 10, 2006, pp. 1225-1230. [23] T. Kitamaru, A. Ahima, M. Augawara, et al., “Psycho- social Correlates of Antennal Depression,” Psychotherapy and Psychosomatics, Vol. 65, 1998, pp. 117-123. doi:10.1159/000289062 [24] A. O. Ilesanmi, O. Fawole, D. O. Olaleye and A. Arowo- jolu, “Pregnancy Outcome in the Elderly Primigravidae,” Journal of Obstetrics and Gynaecology, Vol. 18, No. 1, 1998, pp. 40-43. doi:10.1080/01443619868253 [25] M. Carolan, “The Project: Having a Baby over 35 Years,” Women and Birth, Vol. 20, No. 3, 2007, pp. 121-126. doi:10.1016/j.wombi.2007.05.004 [26] R. Lampinen, K. Vehvilainen-Julkunen and P. Kank- kunen, “A Review of Pregnancy in Women over 35 Years of Age,” Open Nursing Journal, Vol. 3, 2009, pp. 33-38. doi:10.2174/1874434600903010033 Copyright © 2013 SciRes. IJCM
|