Vol.1, No.1, 1-3 (2013) Open Journal of Emergency Medicine
Presentation of multiple midface fractures combined
with intracranial injury treated conservatively
Talal Rane1, Firas Nasser2, Samir Taha2*
1Department of Oral & Maxillofacial Surgery, Al-Ahli Hospital, Doha, Qatar
2Department of Oral and Maxillofacial Surgery, Hamad Medical Corporation, Doha, Qatar; *Corresponding Author: staha3@hmc.org.qa
Received 17 July 2013; revised 19 August 2013; accepted 1 September 2013
Copyright © 2013 Talal Rane et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Midface injuries are normally the result of high
forces impacted on the fac e , that can bypass the
power of the connection buttresses, which are
thick and strong, base of skull is also a rigid and
tough structure which requires significant forces
to break. In our case, multiple midface and cra-
nial base fractures are presented, which reflect
injury caused by high forces and norma lly, these
result in instability in the facial skeleton, or
cause CSF rhinorrhea, or sharp spicules to en-
danger the orbit or the anterior cranial fossa, or
the presence of any other indication of surgery.
It is unusual to find such an extent of facial
trauma and such a multiplication of fractures on
the midface and cranial base levels, yet they
were st able enough an d without a re al indication
to require surgical interference.
Keywords: Midface Fracture; Upp er Face Fracture;
Conservative Management
1. INTRODUCTION
Combined intracranial injury with midface and upper
face multiple fractures signify severe force involved [1-
4], published work on forces calculated to produce a
fracture of each craniofacial bone structure is well docu-
mented [1,2], normally, this results in severe injuries to
the face [1-3]. Hodgson, V.R. et al. presented detailed
work on the tolerance of facial bones to impact [3], and
indicated that impacts produce fracture near 200 pounds,
but that is closely related to the length of the pulse of
impact measured in milliseconds.
A lot of work is presented in the literature about treat-
ment [5-8], sequencing of which bone to fix first [6,7],
timing of treatment [6,7].
We present a case of facial trauma that resulted in
multiple midface and upper face fractures combined with
a base-of-skull fracture, but all were undisplaced and not
mobile therefore, did not require any intervention, and
were managed conservatively, together with the intracra-
nial hemorrhage being minor, that did not require surgi-
cal treatment as well.
2. CASE REPORT
A (46) years old year old male was brought to the A &
E Department of Hamad General Hospital on 12 May
2009, he was lowering a swimming pool basin down into
a pre-dug site in a house garden, when the edge of the
basin hit him on the face.
Patient was conscious, oriented with GCS 15/15, his
BP was 146/82 and Oxygen saturation of 98%, airway
was stable and neck is clear of injury.
Craniofacial examination revealed bilateral periorbital
ecchymosis, active oronasal bleeding, and oro-facial lac-
erations.
Pupils were round, equal and brisk reactive, directly
and consensually, visual acu ity intact with mild p roptosis
of right eye, no obvious restriction of ocular movements.
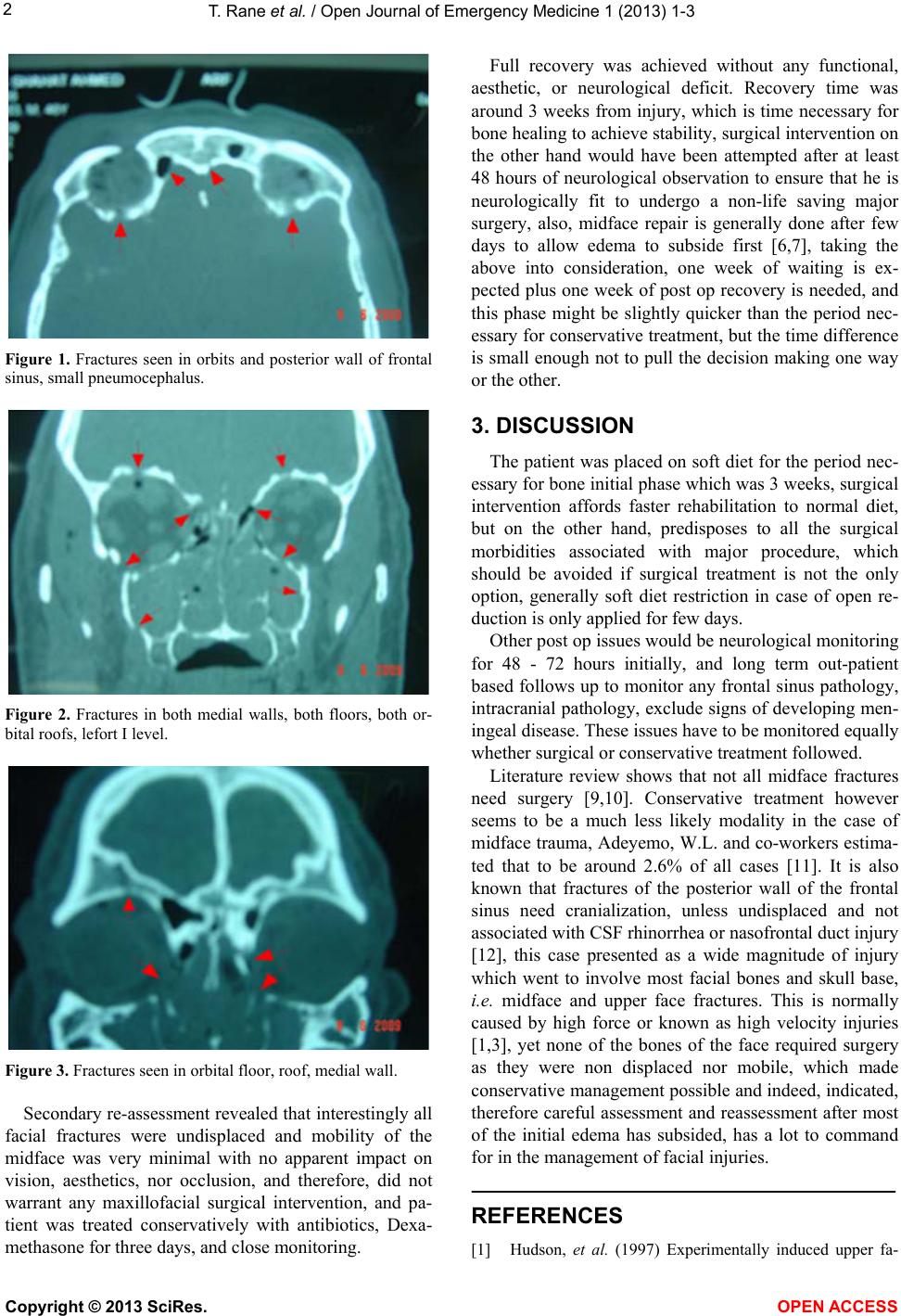
CT scan showed left small foci of frontal subarachno id
hemorrhage and bleeding into the anterior part of the
interhaemospheric fissure and very small pneumocepha-
lus of the frontal region (Figure 1) plus fracture of the
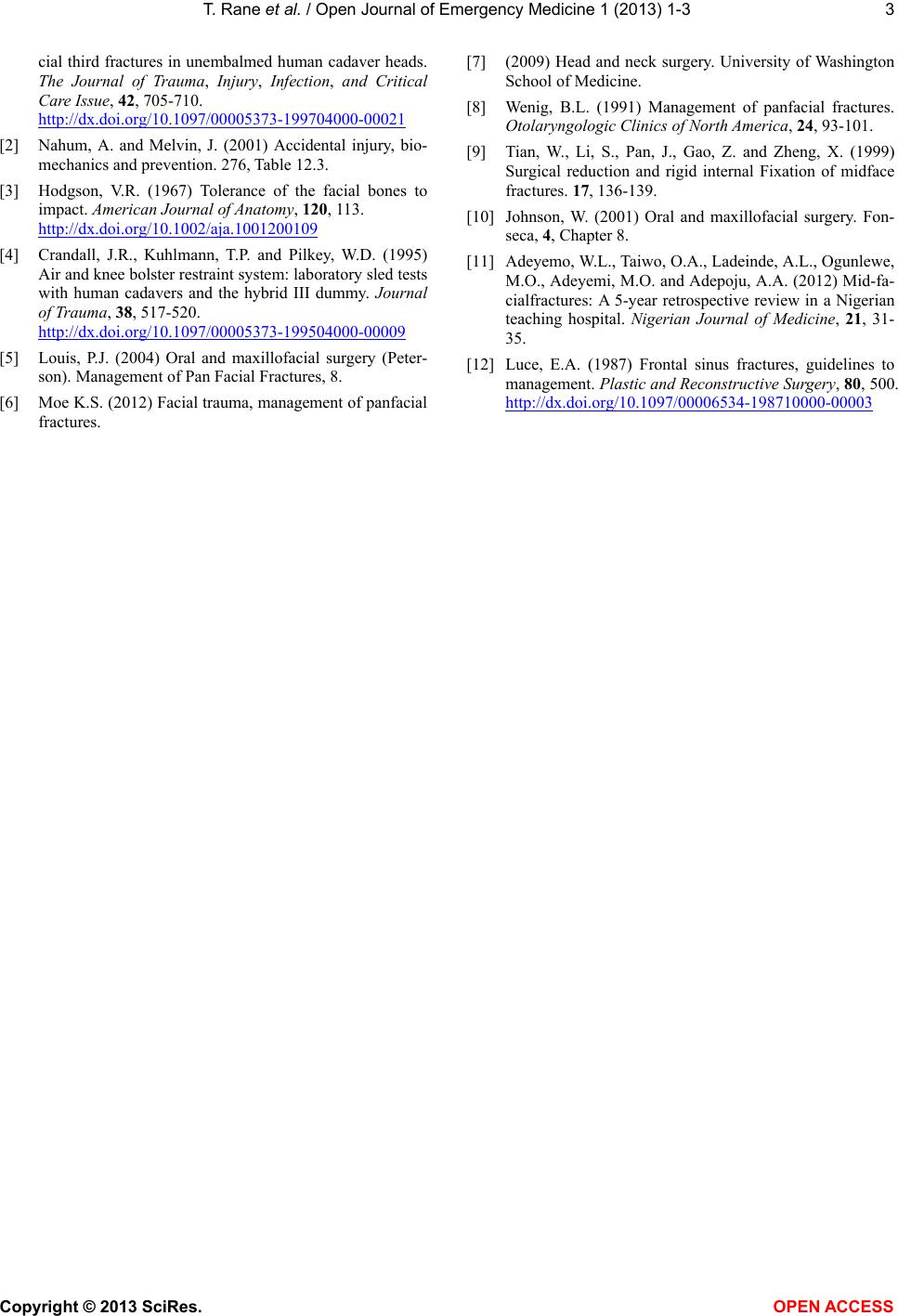
anterior cranial fossa, both orbital roofs (Figures 1 and 2)
and right side of the frontal bone (Figure 3) with fracture
of the left zygoma and a lefort I (Figure 2), nasal bone,
both medial walls and floors of orbits (Figures 2 and 3),
as reported on CT by radiologist and confirmed by the
maxillofacial team responsible for patient.
Initially patient was managed in the trauma room by
bilateral anterior nasal packs, and oro-facial lacerations
were closed as appropriate, under an umbrella of intra-
venous Augmentin plus Dexamethasone, patient was
shifted to Trauma ITU for neurological and eye observa-
tion.
Copyright © 2013 SciRes. OPEN AC CESS