N. ANDRADE ET AL.
Copyright © 2013 SciRes. SS
404
gele et al. [19] also suggested that routine peritoneal
closure should be discarded, despite its association with
low morbidity related to fever and infection [19].
On the other hand, Cheong et al. [4] concluded in an
extensive literature review that there are no differences
between peritoneal closure and non-closure in lower ab-
dominal incisions with regards to comorbidities such as
infections, fever and peritoneal adhesion formation,
among others [3]. Weerawetwat et al. [8] also described
that in women submitted to caesarean section with and
without peritoneum closure there are no statistically sig-
nificant differences, despite their higher incidence in the
group whose peritoneum was closed [8].
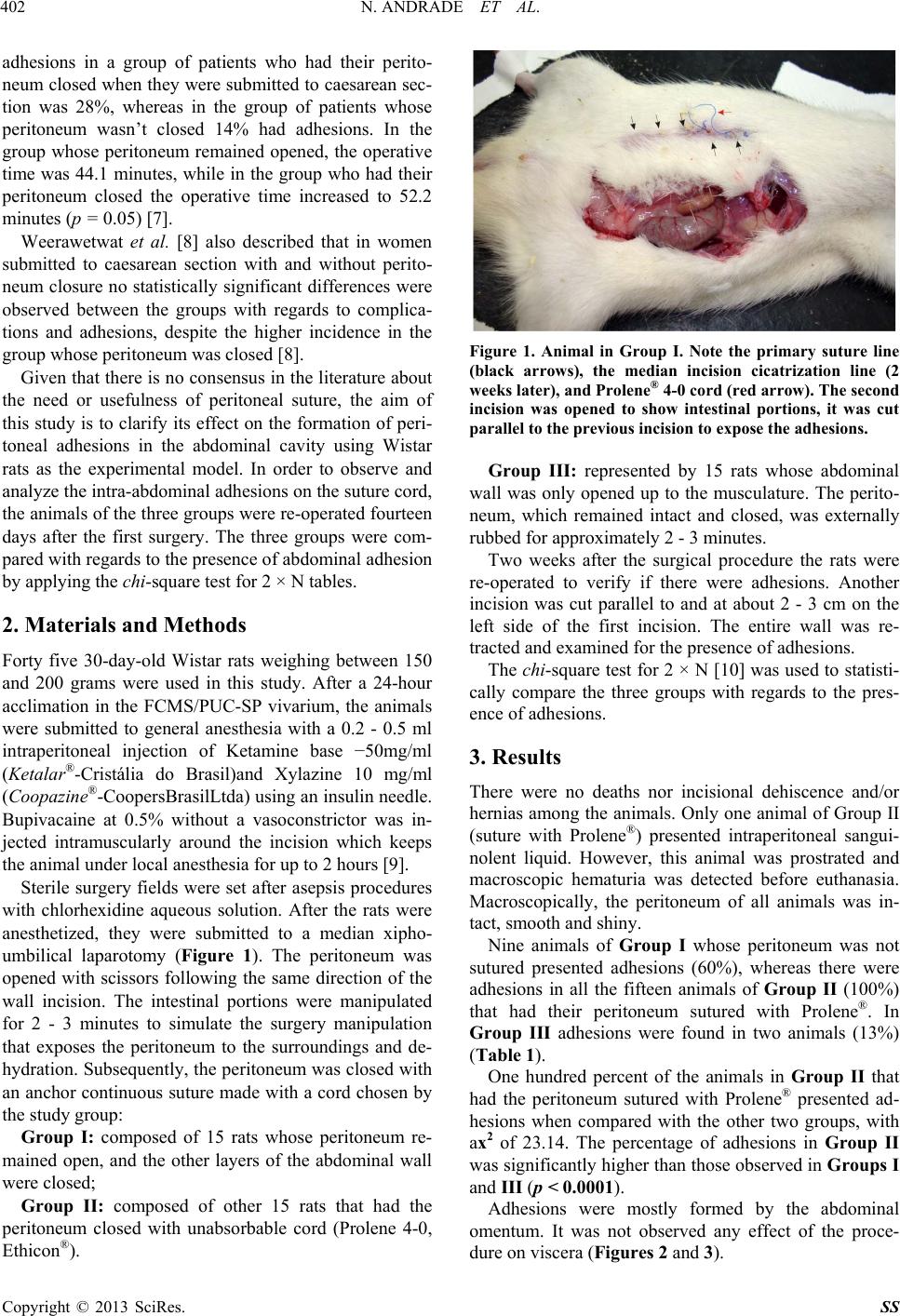
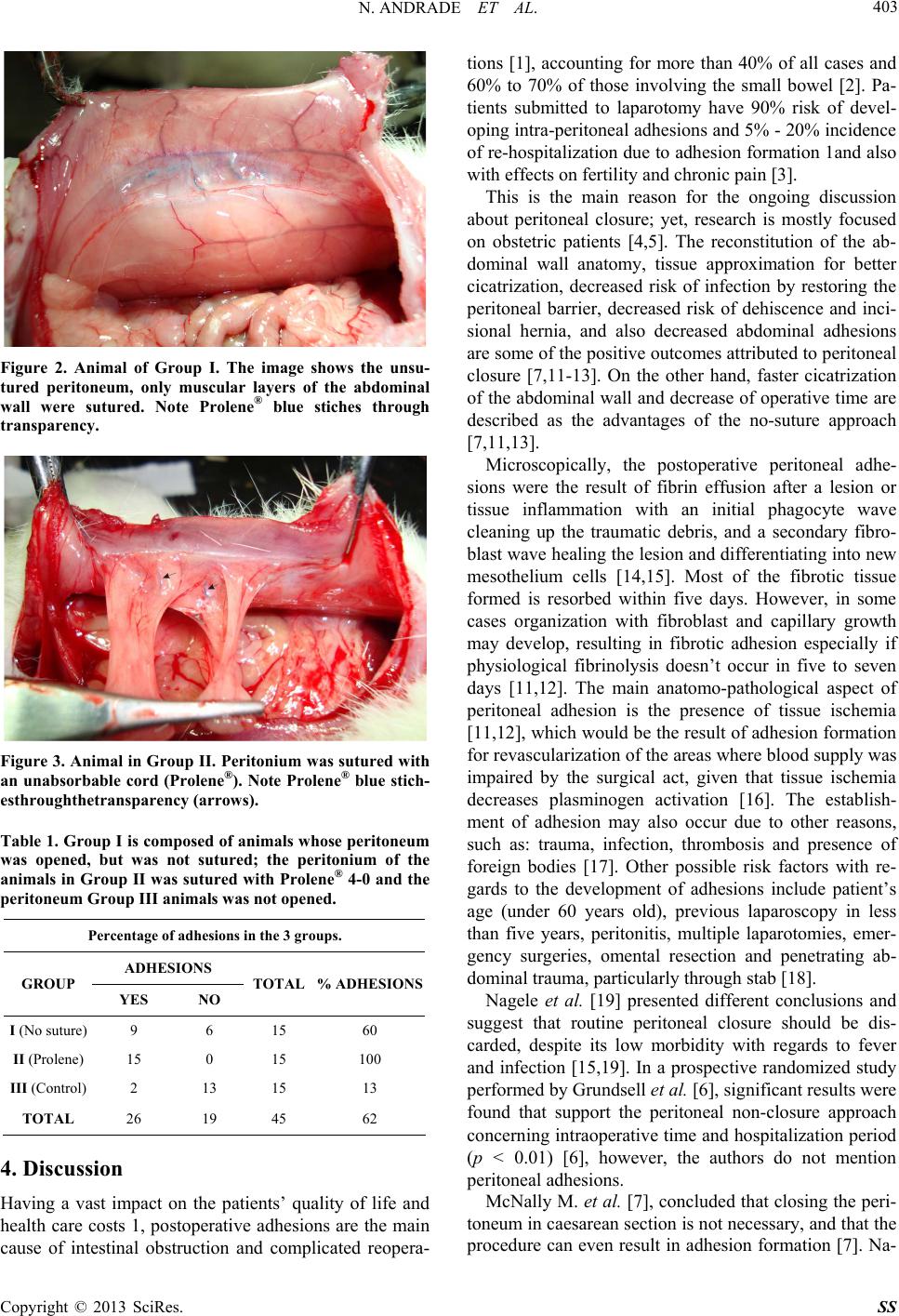
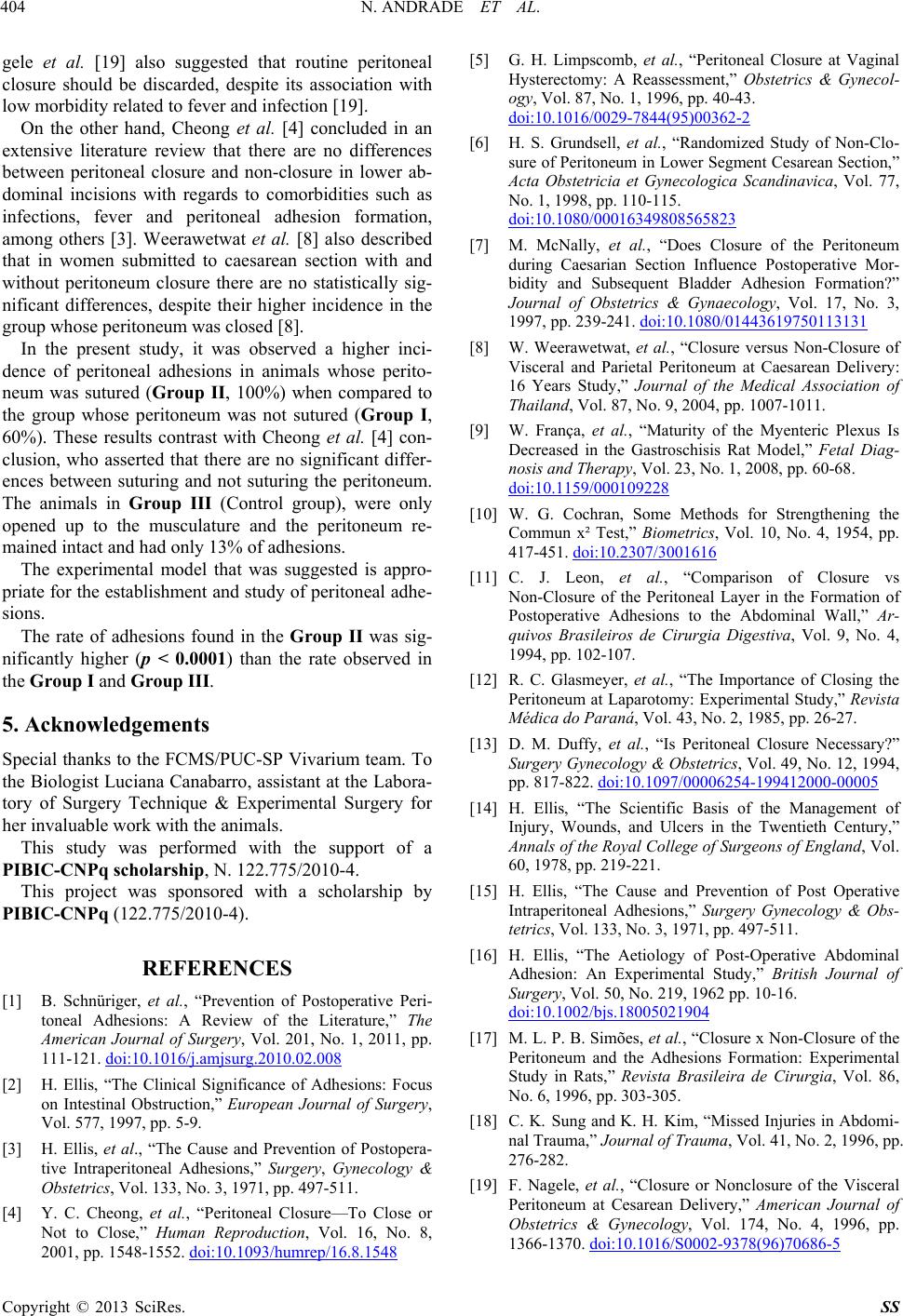
In the present study, it was observed a higher inci-
dence of peritoneal adhesions in animals whose perito-
neum was sutured (Group II, 100%) when compared to
the group whose peritoneum was not sutured (Group I,
60%). These results contrast with Cheong et al. [4] con-
clusion, who asserted that there are no significant differ-
ences between suturing and not suturing the peritoneum.
The animals in Group III (Control group), were only
opened up to the musculature and the peritoneum re-
mained intact and had only 13% of adhesions.
The experimental model that was suggested is appro-
priate for the establishment and study of peritoneal adhe-
sions.
The rate of adhesions found in the Group II was sig-
nificantly higher (p < 0.0001) than the rate observed in
the Group I and Group III.
5. Acknowledgements
Special thanks to the FCMS/PUC-SP Vivarium team. To
the Biologist Luciana Canabarro, assistant at the Labora-
tory of Surgery Technique & Experimental Surgery for
her invaluable work with the animals.
This study was performed with the support of a
PIBIC-CNPq scholarship, N. 122.775/2010-4.
This project was sponsored with a scholarship by
PIBIC-CNPq (122.775/2010-4).
REFERENCES
[1] B. Schnüriger, et al., “Prevention of Postoperative Peri-
toneal Adhesions: A Review of the Literature,” The
American Journal of Surgery, Vol. 201, No. 1, 2011, pp.
111-121. doi:10.1016/j.amjsurg.2010.02.008
[2] H. Ellis, “The Clinical Significance of Adhesions: Focus
on Intestinal Obstruction,” European Journal of Surgery,
Vol. 577, 1997, pp. 5-9.
[3] H. Ellis, et al., “The Cause and Prevention of Postopera-
tive Intraperitoneal Adhesions,” Surgery, Gynecology &
Obstetrics, Vol. 133, No. 3, 1971, pp. 497-511.
[4] Y. C. Cheong, et al., “Peritoneal Closure—To Close or
Not to Close,” Human Reproduction, Vol. 16, No. 8,
2001, pp. 1548-1552. doi:10.1093/humrep/16.8.1548
[5] G. H. Limpscomb, et al., “Peritoneal Closure at Vaginal
Hysterectomy: A Reassessment,” Obstetrics & Gynecol-
ogy, Vol. 87, No. 1, 1996, pp. 40-43.
doi:10.1016/0029-7844(95)00362-2
[6] H. S. Grundsell, et al., “Randomized Study of Non-Clo-
sure of Peritoneum in Lower Segment Cesarean Section,”
Acta Obstetricia et Gynecologica Scandinavica, Vol. 77,
No. 1, 1998, pp. 110-115.
doi:10.1080/00016349808565823
[7] M. McNally, et al., “Does Closure of the Peritoneum
during Caesarian Section Influence Postoperative Mor-
bidity and Subsequent Bladder Adhesion Formation?”
Journal of Obstetrics & Gynaecology, Vol. 17, No. 3,
1997, pp. 239-241. doi:10.1080/01443619750113131
[8] W. Weerawetwat, et al., “Closure versus Non-Closure of
Visceral and Parietal Peritoneum at Caesarean Delivery:
16 Years Study,” Journal of the Medical Association of
Thailand, Vol. 87, No. 9, 2004, pp. 1007-1011.
[9] W. França, et al., “Maturity of the Myenteric Plexus Is
Decreased in the Gastroschisis Rat Model,” Fetal Diag-
nosis and Therapy, Vol. 23, No. 1, 2008, pp. 60-68.
doi:10.1159/000109228
[10] W. G. Cochran, Some Methods for Strengthening the
Commun x² Test,” Biometrics, Vol. 10, No. 4, 1954, pp.
417-451. doi:10.2307/3001616
[11] C. J. Leon, et al., “Comparison of Closure vs
Non-Closure of the Peritoneal Layer in the Formation of
Postoperative Adhesions to the Abdominal Wall,” Ar-
quivos Brasileiros de Cirurgia Digestiva, Vol. 9, No. 4,
1994, pp. 102-107.
[12] R. C. Glasmeyer, et al., “The Importance of Closing the
Peritoneum at Laparotomy: Experimental Study,” Revista
Médica do Paraná, Vol. 43, No. 2, 1985, pp. 26-27.
[13] D. M. Duffy, et al., “Is Peritoneal Closure Necessary?”
Surgery Gynecology & Obstetrics, Vol. 49, No. 12, 1994,
pp. 817-822. doi:10.1097/00006254-199412000-00005
[14] H. Ellis, “The Scientific Basis of the Management of
Injury, Wounds, and Ulcers in the Twentieth Century,”
Annals of the Royal College of Surgeons of England, Vol.
60, 1978, pp. 219-221.
[15] H. Ellis, “The Cause and Prevention of Post Operative
Intraperitoneal Adhesions,” Surgery Gynecology & Obs-
tetrics, Vol. 133, No. 3, 1971, pp. 497-511.
[16] H. Ellis, “The Aetiology of Post-Operative Abdominal
Adhesion: An Experimental Study,” British Journal of
Surgery, Vol. 50, No. 219, 1962 pp. 10-16.
doi:10.1002/bjs.18005021904
[17] M. L. P. B. Simões, et al., “Closure x Non-Closure of the
Peritoneum and the Adhesions Formation: Experimental
Study in Rats,” Revista Brasileira de Cirurgia, Vol. 86,
No. 6, 1996, pp. 303-305.
[18] C. K. Sung and K. H. Kim, “Missed Injuries in Abdomi-
nal Trauma,” Journal of Trauma, Vol. 41, No. 2, 1996, pp.
276-282.
[19] F. Nagele, et al., “Closure or Nonclosure of the Visceral
Peritoneum at Cesarean Delivery,” American Journal of
Obstetrics & Gynecology, Vol. 174, No. 4, 1996, pp.
1366-1370. doi:10.1016/S0002-9378(96)70686-5