Comparison between Distractor Application on Both Radial & Ulnar Side and Radial Side
Only for Fracture Distal Radius with Ulnar Styloid Fracture
232
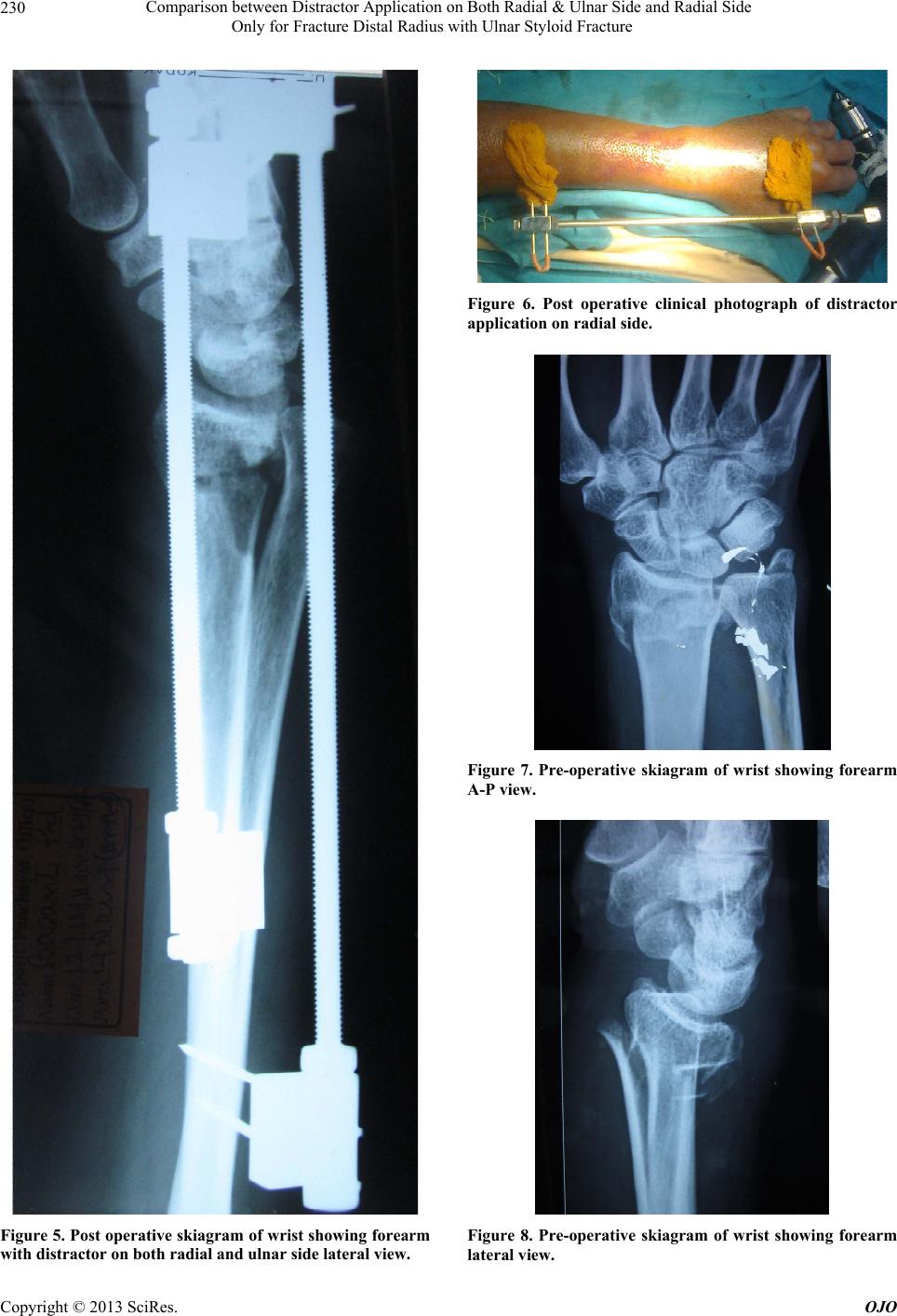
Table 3. Intra-carpal step off.
Intra-carpal
step off <2 mm Intra-carpal
step off >2 mm P-value
Group A 5 11
Group B 12 4 0.0320
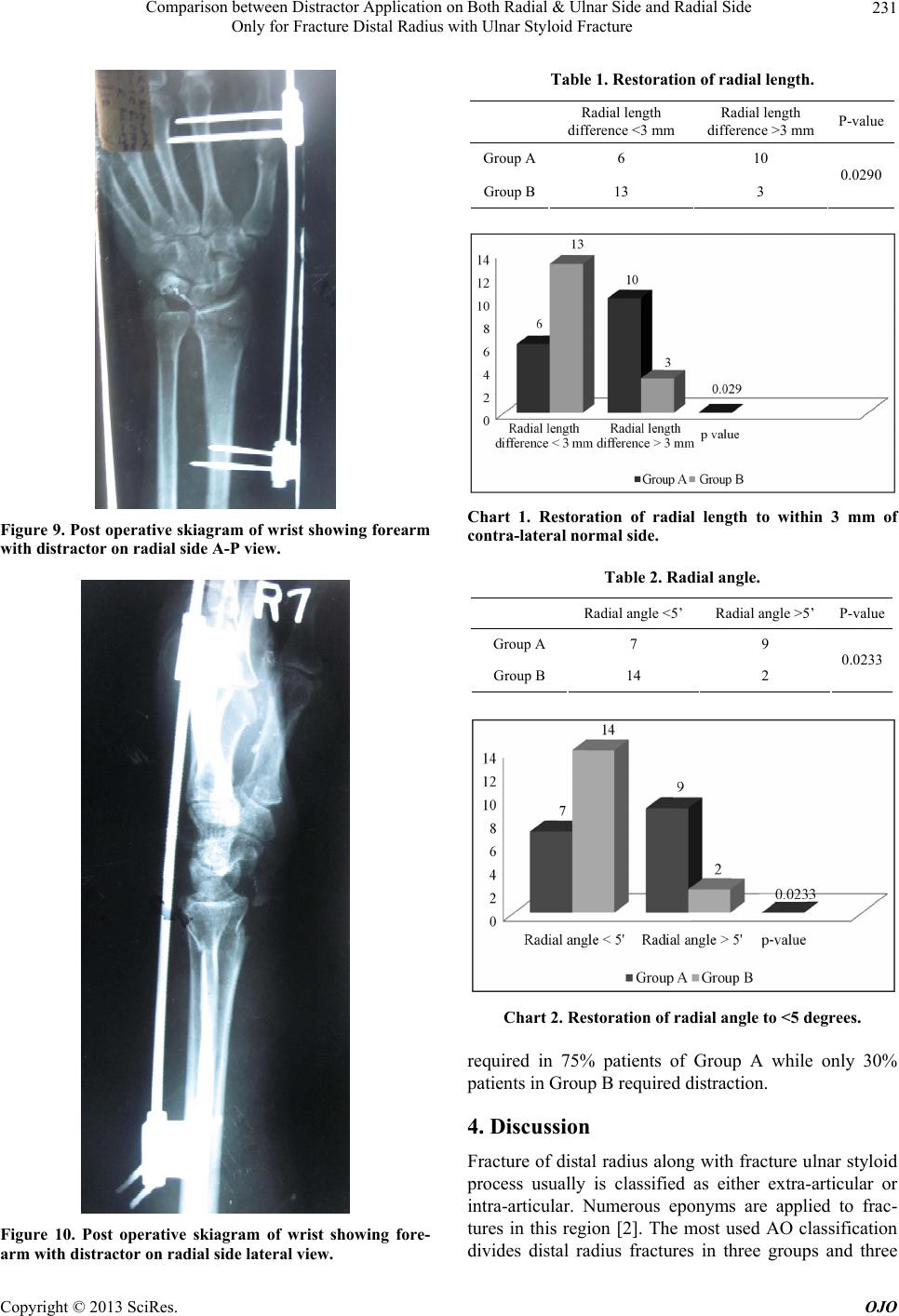
Chart 3. Intra-carpal step off.
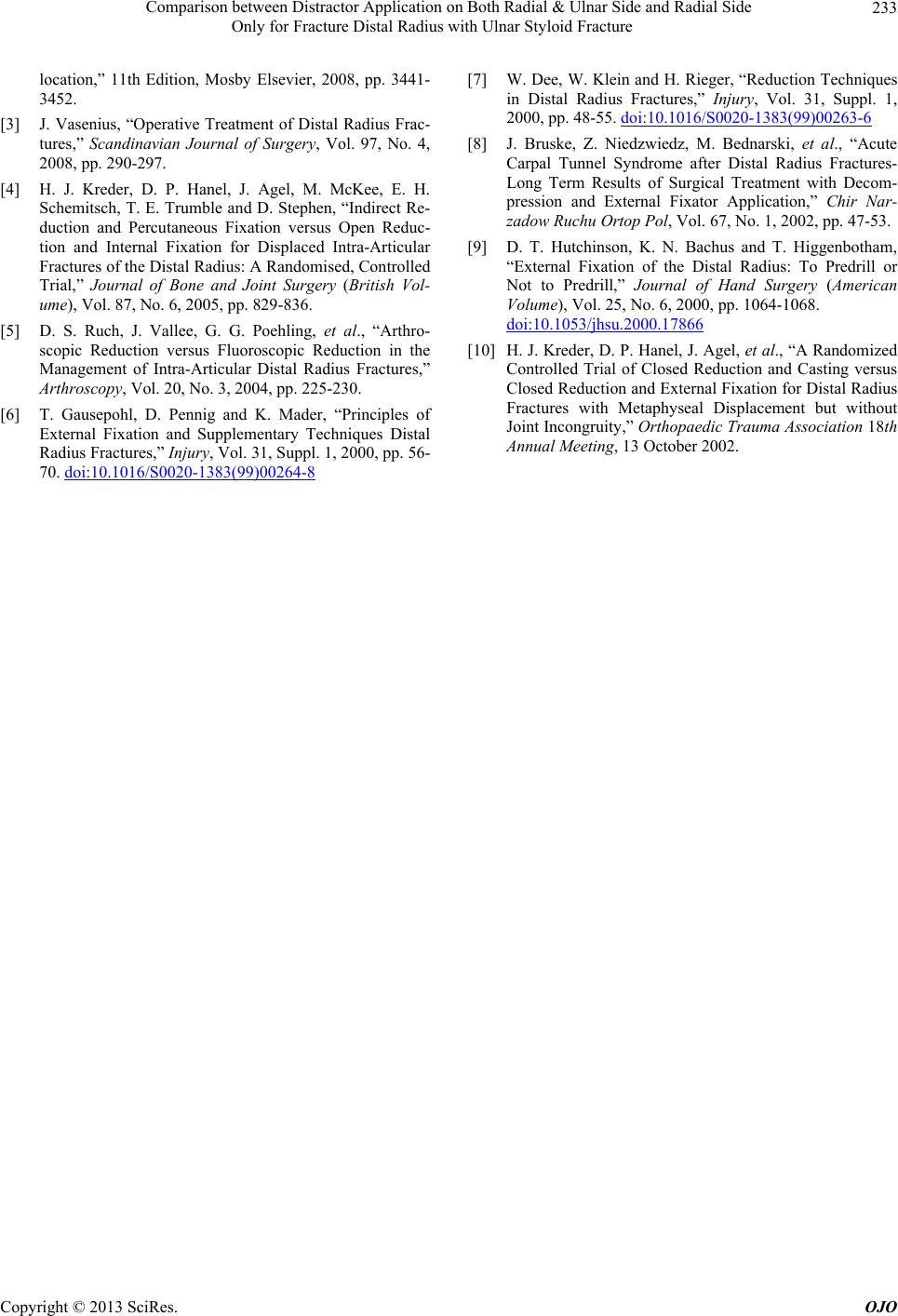
Table 4. Palmar tilt.
Normal palmar tilt
(0 degree ) Abnormal
palmar tilt P-value
Group A 6 10
Group B 15 1 0.0021
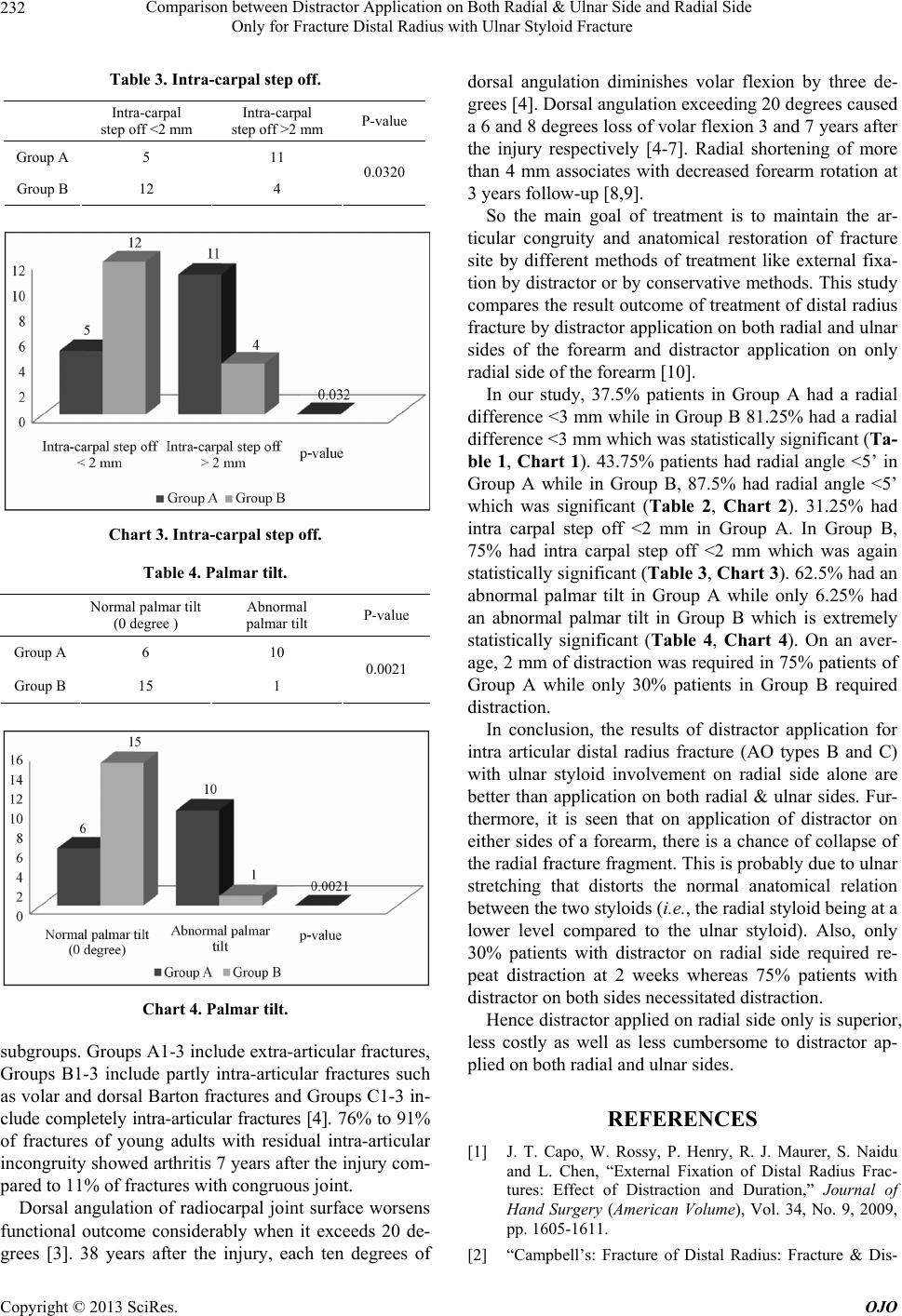
Chart 4. Palmar tilt.
subgroups. Groups A1-3 include extra-articular fractures,
Groups B1-3 include partly intra-articular fractures such
as volar and dorsal Barton fractures and Groups C1-3 in-
clude completely intra-articular fractures [4]. 76% to 91%
of fractures of young adults with residual intra-articular
incongruity showed arthritis 7 years after the injury com-
pared to 11% of fractures with congruous joint.
Dorsal angulation of radiocarpal joint surface worsens
functional outcome considerably when it exceeds 20 de-
grees [3]. 38 years after the injury, each ten degrees of
dorsal angulation diminishes volar flexion by three de-
grees [4]. Dorsal angulation exceeding 20 degrees caused
a 6 and 8 degrees loss of volar flexion 3 and 7 years after
the injury respectively [4-7]. Radial shortening of more
than 4 mm associates with decreased forearm rotation at
3 years follow-up [8,9].
So the main goal of treatment is to maintain the ar-
ticular congruity and anatomical restoration of fracture
site by different methods of treatment like external fixa-
tion by distractor or by conservative methods. This study
compares the result outcome of treatment of distal radius
fracture by distractor application on both radial and ulnar
sides of the forearm and distractor application on only
radial side of the forearm [10].
In our study, 37.5% patients in Group A had a radial
difference <3 mm wh ile in Group B 81.25% had a radial
difference <3 mm which was statistically significant (Ta-
ble 1, Chart 1). 43.75% patients had radial angle <5’ in
Group A while in Group B, 87.5% had radial angle <5’
which was significant (Table 2, Chart 2). 31.25% had
intra carpal step off <2 mm in Group A. In Group B,
75% had intra carpal step off <2 mm which was again
statistically significant (Tab le 3, Chart 3). 62.5% had an
abnormal palmar tilt in Group A while only 6.25% had
an abnormal palmar tilt in Group B which is extremely
statistically significant (Table 4, Chart 4). On an aver-
age, 2 mm of distraction was required in 75% patients of
Group A while only 30% patients in Group B required
distraction.
In conclusion, the results of distractor application for
intra articular distal radius fracture (AO types B and C)
with ulnar styloid involvement on radial side alone are
better than application on both radial & ulnar sides. Fur-
thermore, it is seen that on application of distractor on
either sides of a forearm, there is a chance of collapse of
the radial fracture fragment. This is probably due to ulnar
stretching that distorts the normal anatomical relation
between the two styloids (i.e., the radial styloid being at a
lower level compared to the ulnar styloid). Also, only
30% patients with distractor on radial side required re-
peat distraction at 2 weeks whereas 75% patients with
distractor on both sides necessitated distraction.
Hence distractor applied on radial side only is superior,
less costly as well as less cumbersome to distractor ap-
plied on both radial and ulnar sides.
REFERENCES
[1] J. T. Capo, W. Rossy, P. Henry, R. J. Maurer, S. Naidu
and L. Chen, “External Fixation of Distal Radius Frac-
tures: Effect of Distraction and Duration,” Journal of
Hand Surgery (American Volume), Vol. 34, No. 9, 2009,
pp. 1605-1611.
[2] “Campbell’s: Fracture of Distal Radius: Fracture & Dis-
Copyright © 2013 SciRes. OJO