Marital Status and HIV Prevalence in Nigeria: Implications for Effective Prevention Programmes for Women
212
survey in Nigeria that provided population-based esti-
mates of HIV prevalence in Nigeria. Survey participants
were selected across the 36 states and the Federal Capital
Territory (FCT) of Nigeria through a multi-stage prob-
ability cluster sampling techn iqu e at three levels.
Eligible respondents were female aged 15 - 49 years
and male aged 15 - 64 years. Selection was based on the
sampling frame of enumeration areas which is main-
tained by the Nigerian National Population Commission
(NPC). List of localities was provided by NPC and strati-
fied into major or big towns, medium towns and rural
according to the 2006 Population Census. Localities
where the surveys were conducted were selected from
this list comprising of a mixture of the three main cate-
gories with more of rural localities according to the 2006
Nigeria population distribution.
A structured questionnaire which was pre-tested was
administered to the respondents. Research personnel
were trained with the aim of acquainting them with the
survey instruments. Questions were adapted from UN-
AIDS general population HIV & AIDS indicator and the
Demographic and Health Survey questionnaires. Due to
the language complexity in Nigeria (with over 250 lan-
guages), questionnaire was designed primarily in English
Language. Translations of keywords into local languages
were done at a central level training to enhance uniform-
ity and standardisation of questionnaire administration.
Enumerators, including HIV & AIDS counsellors/testers
were versed both in English and the local languages of
the communities where they worked. For ethical appro-
priateness, the survey instruments and materials received
the approval of the Federal and State Ministries of Health
in Nigeria before implementation through the Nigerian
Institute of Medical Research. Consent of the respon-
dents was obtained individually and they were ade-
quately informed of the survey objectives upon which an
individual has the right to participate or otherwise with-
out any fear of intimidation. A total of 11,822 respon-
dents were selected for the survey but only 11,521 re-
sponded to the questionnaire.
An HIV pre-test (to all selected eligible respondents)
and post-test (only for those that obliged HIV testing)
counselling was offered, while results of the test was
provided orally but referrals to facilities for further con-
firmation and possible placement on treatment for those
that were positive. At the end of data co llection exercise,
the HIV test results were further confirmed on the dried
blood samples collected from respondents, in a well-eq-
uipped laboratory by an external consultant.
2.2. Data
Overall, 5360 women were interviewed in the 2007
NARHS. Of these, only 4195 agreed to be tested after the
HIV pre-test counselling. Therefore, all analyses in this
paper were based on the 4195 female respondents that
answered the behavioural questionnaire and accepted
HIV testing. Marital status was grouped into “Never mar-
ried, Currently married/cohabiting, and formerly mar-
ried (i.e. separated, divorced and widowed)”. In general,
the mean age of the respondents was 27.8 years with a
standard deviation (SD) of 9.34. Mean ages according to
the marital status are 19.8 years (SD = 4.90) for never
married, 30.5 years (SD = 8.61) for currently mar-
ried/cohabiting, and 35.9 years (SD = 9.33) for formerly
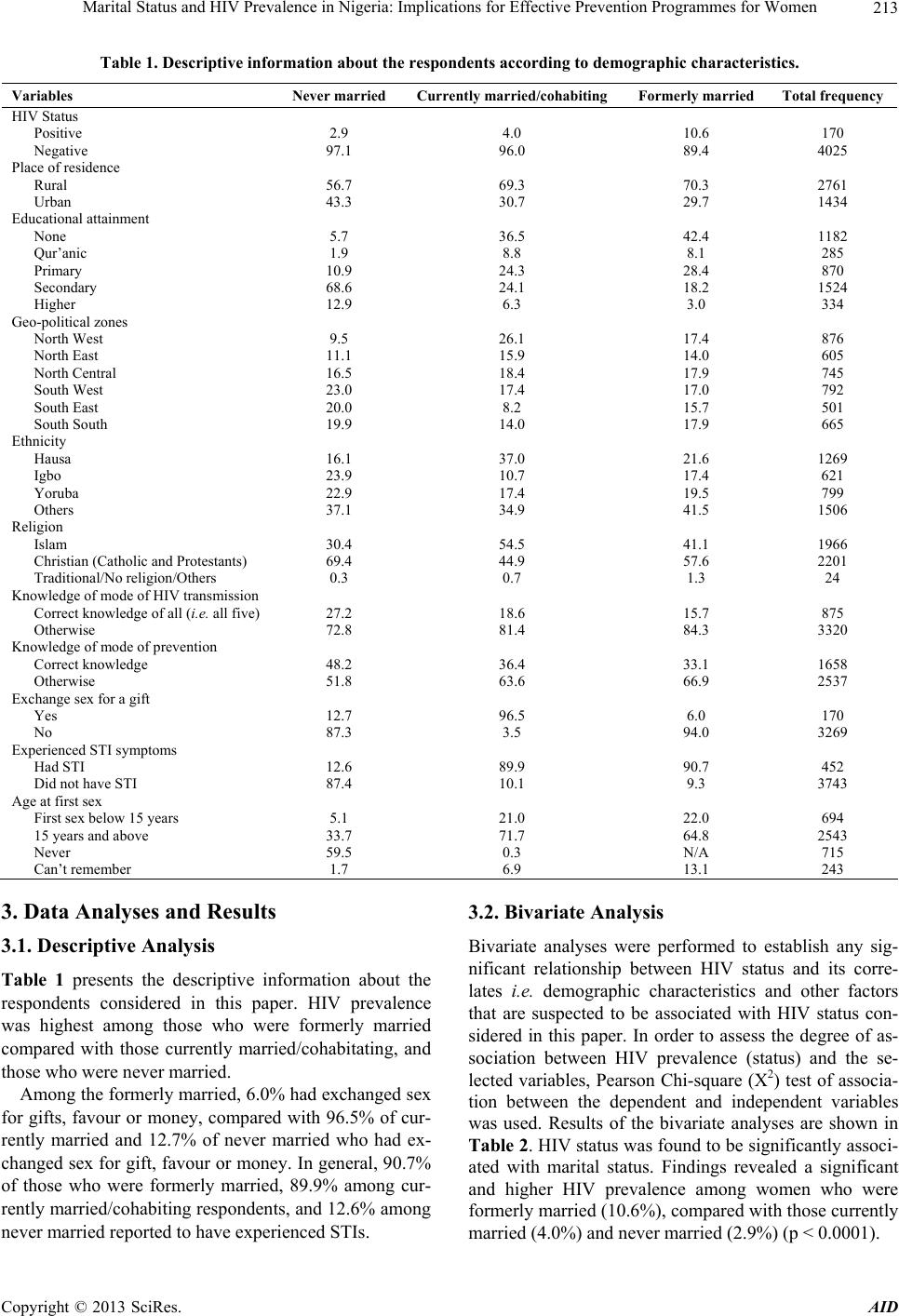
married. Table 1 presents the distribution of the respon-
dents according to marital status and selected character-
istics.
2.2.1. Depend ent Variable
The outcome variable of interest in this study is the result
of the HIV test conducted among respondents who were
interviewed and volunteered to be tested. For the purp ose
of this analysis, response indicating positive HIV test
was scored “1” and “0” otherwise.
2.2.2. Independent Variables
The key independent variables in this paper are: “marital
status”, “location of residence”, “geo-political zones”,
“age”, “tribe”, “age at first sex”, “experience of sexually
transmitted infections (STIs)”, “multiple partnering”,
“transactional sex i.e. sex in exchange for gifts/favour”,
religion, “k nowledge of HIV p revention ”, “knowledge of
HIV transmission”, and “education”. Marital status with
never married as reference category. Place of residence:
urban and rural (reference category). Others include
educational attainment: Qur’anic/primary, secondary,
higher, and no formal education (reference category).
Nigeria is divided into six geo-political zones: North
West, North East, South West, South East, South South
and North Central (the North Central zone was used as
the reference). Respondents’ age was grouped into four
categories; 15 - 19 years, 20 - 24 years, 25 - 34 years,
and 35 - 49 years (reference). Tribe was put into: Hau sa,
Igbo, Yoruba, and others (reference). Religion was clas-
sified into three; Christianity, Islam and others (refer-
ence).
Background characteristics (demographic variables)
and other correlates of HIV prevalence which are impor-
tant predictors were adjusted for in multiple logistic re-
gression models. These include location, marital status,
education, geo-political zones, respondents’ age, tribe,
religion, knowledge about modes of transmission and
prevention of HIV and AIDS, and sexual behavioural
indicators such as age at sexual debut, multiple sexual
partnering; sex in exchange for gifts, favour or money,
and self-report of sexually transmitted infections in the
las 12 months. t
Copyright © 2013 SciRes. AID