Clinical Criteria for Airway Assessment: Correlations with Laryngoscopy and Endotracheal Intubation Conditions
Copyright © 2013 SciRes. OJAnes
325
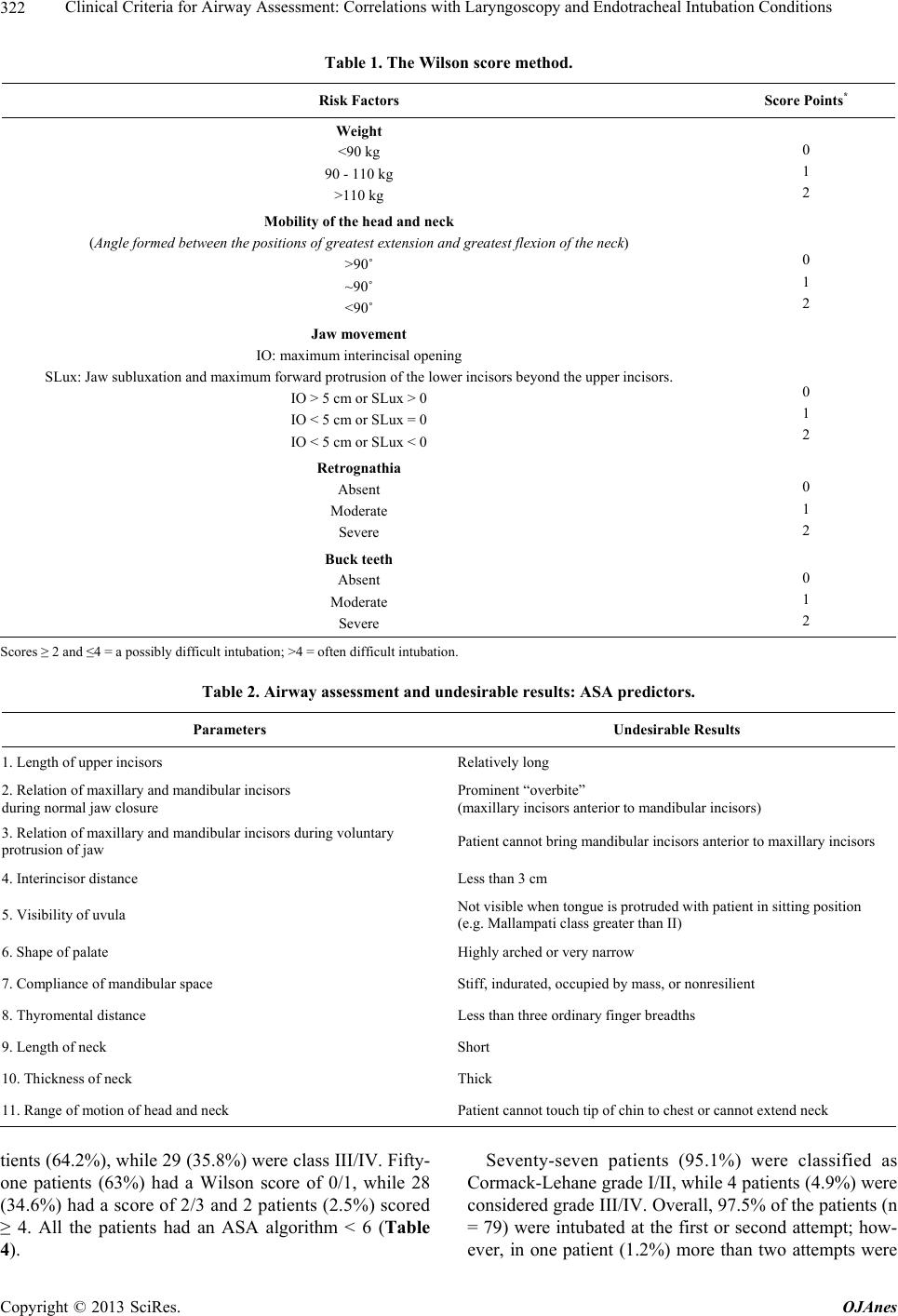
Since the Wilson score takes various factors and ana-
tomical characteristics into consideration rather than just
one as in the case of the Mallampati classification, sensi-
tivity and specificity tend to be higher. Moreover, the
characteristics evaluated are well defined and well de-
scribed, leaving less margin for subjectivity during the
exam. This brings the various studies closer methodol-
ogically, ensuring that the results are in general compa-
rable.
Some limitations of the present study must be men-
tioned. The total number of patients in the sample (81) is
considered small for a study involving events that are
relatively rare in the general population such as the case
of a difficult airway. This may have been responsible for
the lack of statistical significance in some of our results.
Since this is a teaching and training institute for anesthe-
siologists, most of the data were collected by trainee
physicians. Nevertheless, although data were collected
by different individuals throughout the study period, all
were duly trained for this function by the authors. Be-
cause the intubations were performed by resident physi-
cians, the number of attempts recorded may have been
less in some cases if the procedure had been performed
by an experienced anesthesiologist. It should be empha-
sized that in the patient in whom intubation was unsuc-
cessful by conventional laryngoscopy, the anesthesiolo-
gist responsible for the case also failed to intubate the
patient and was obliged to resort to the use of a gum
elastic bougie to successfully conclude the procedure.
The present study concludes that the Wilson score,
despite being seldom used in clinical practice, is a highly
sensitive predictor of a difficult airway, although its
specificity is low. Further studies with larger sample
sizes are required to confirm these findings and to obtain
statistically significant results for the other indexes eva-
luated.
REFERENCES
[1] S. R. Mallampati, S. P. Gatt, L. D. Gugino, S. P. Desai, B.
Waraksa, D. Freiberger and P. L. Liu, “A Clinical Sign to
Predict Difficult Endotracheal Intubation: A Prospective
Study,” Canadian Anaesthetists’ Society Journal, Vol. 32,
No. 4, 1985, pp. 429-434.
[2] G. L. Samsoon and J. R. Young, “Difficult Endotracheal
Intubation: A Retrospective Study,” Anaesthesia, Vol. 42,
No. 5, 1987, pp. 487-490.
doi:10.1111/j.1365-2044.1987.tb04039.x
[3] T. Shiga, Z. Wajima, T. Inoue and A. Sakamoto, “Pre-
dicting Difficult Intubation in Apparently Normal Pa-
tients. A Meta-Analysis of Bedside Screening Test Per-
formance,” Anesthesiology, Vol. 103, No. 2, 2005, pp.
429-437. doi:10.1097/00000542-200508000-00027
[4] L. H. Lundstrøm, M. Vester-Andersen, A. M. Møller, S.
Charuluxananan, J. L’hermite and J. Wetterslev, “Poor
Prognostic Value of the Modified Mallampati Score: A
Meta-Analysis Involving 177 088 Patients,” British Jour-
nal of Anaesthesia, Vol. 107, No. 5, 2011, pp. 659-667.
doi:10.1093/bja/aer292
[5] J. L. Apfelbaum, C. A. Hagberg, R. A. Caplan, C. D. Blitt,
R. T. Connis, D. G. Nickinovich, C. A. Hagberg, R. A.
Caplan, J. L. Benumof, F. A. Berry, C. D. Blitt, R. H.
Bode, F. W. Cheney, R. T. Connis, O. F. Guidry, D. G.
Nickinovich and A. Ovassapian, “Practice Guidelines for
Management of the Difficult Airway: An Updated Report
by the American Society of Anesthesiologists Task Force
on Management of the Difficult Airway,” Anesthesiology,
Vol. 118, No. 2, 2013, pp. 251-270.
doi:10.1097/ALN.0b013e31827773b2
[6] K. B. Greenland, M. J. Edwards and N. J. Hutton, “Ex-
ternal Auditory Meatus-Sternal Notch Relationship in
Adults in the Sniffing Position: A Magnetic Resonance
Imaging Study,” British Journal of Anaesthesia, Vol. 104,
No. 2, 2010, pp. 268-269. doi:10.1093/bja/aep390
[7] M. E. Wilson, D. Spiegelhalter, J. A. Robertson and P.
Lesser, “Predicting Difficult Intubation,” British Journal
of Anaesthesia, Vol. 61, No. 2, 1988, pp. 211-216.
doi:10.1093/bja/61.2.211
[8] M. Adamus, S. Fritscherova, L. Hrabalek, T. Gabrhelik, J.
Zapletalova and V. Janout, “Mallampati Test as a Predic-
tor of Laryngoscopic View,” Biomedical Papers of the
Medical Faculty of the University Palacký, Vol. 154, No.
4, 2010, pp. 339-344. doi:10.5507/bp.2010.051
[9] A. Lee, L. T. Fan, T. Gin, M. K. Karmakar and W. D.
Ngan Kee, “A Systematic Review (Meta-Analysis) of the
Accuracy of the Mallampati Tests to Predict the Difficult
Airway,” Anesthesia and Analgesia, Vol. 102, No. 6, 2006,
pp. 1867-1878. doi:10.1213/01.ane.0000217211.12232.55
[10] R. Domi, “A Comparison of Wilson Sum Score and
Combination Mallampati, Tiromental and Sternomental
Distances for Predicting Difficult Intubation,” Macedo-
nian Journal of Medical Sciences, Vol. 2, No. 2, 2009, pp.
141-144. doi:10.3889/MJMS.1857-5773.2009.0045