Clinical and Dosimetric Implications of Air Gaps between Bolus and Skin Surface during Radiation Therapy 1255
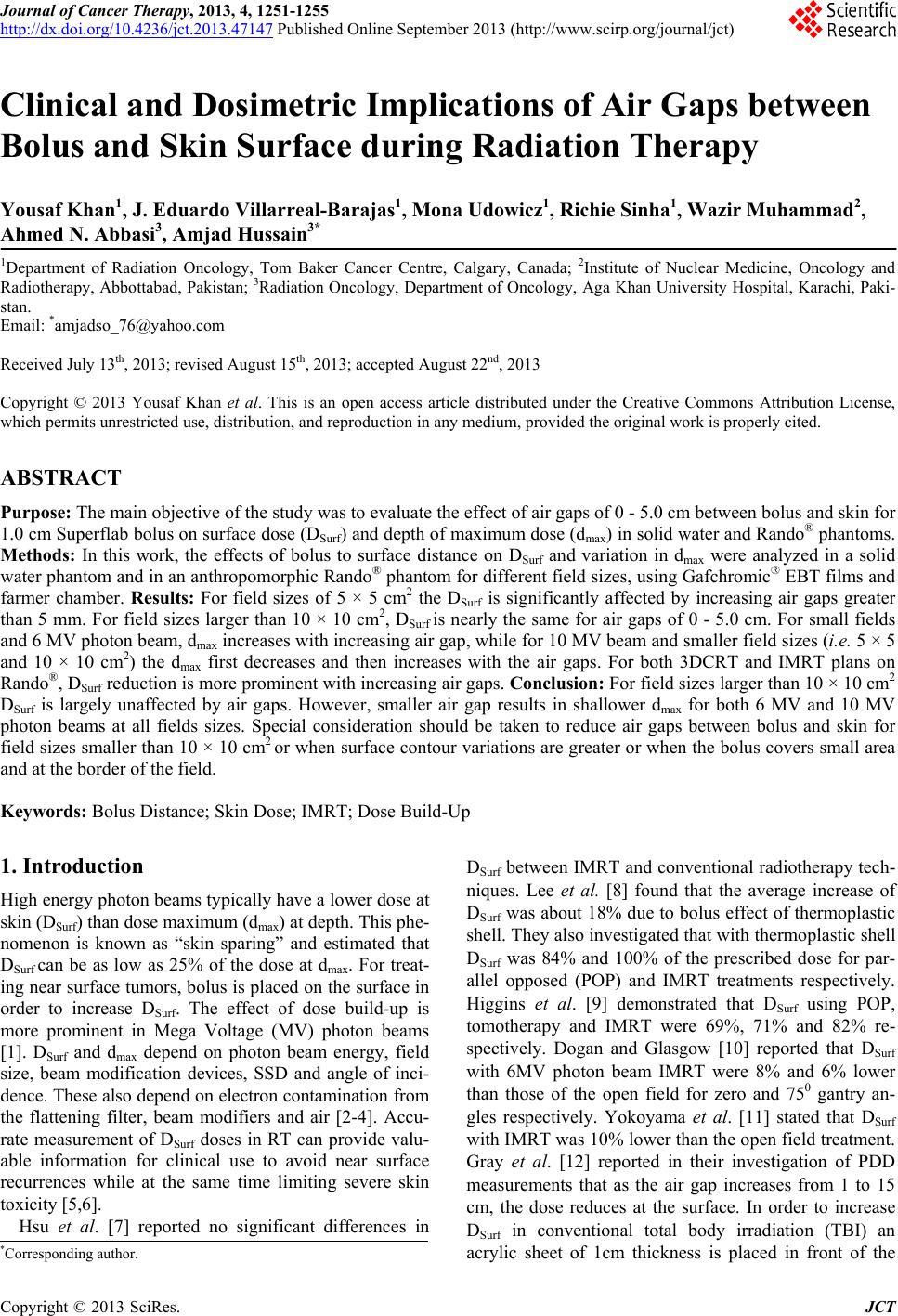
Figure 5. (a) Dose build up characteristics on skin surface for an IMRT 6 MV X-ray beam with 1cm of bolus material at 0 -
5.0 cm air gaps; (b) Reduction in dose caused by varying air gaps under 1 cm of bolus for a 4-fields box 3DCRT plan.
gaps with bolus is less affected for large field sizes such
as 15 × 15 cm
2 and greater. For larger field sizes DSurf
greater than 95% was observed for larger air gapes of 5
cm as well. For IMRT and 3DCRT plans delivered to
Rando®, 94% DSurf was observed for 1 cm air gap. Based
on our results, special consideration is required when
field sizes are smaller and surface contour variations are
greater or when the bolus cover small area and at the
border of the field. In general it is observed that the
closer the bolus to the phantom surface is, the shallower
the dmax is for both 6 MV and 10 MV photon beams and
all fields sizes. For both energies dmax is approximately
proportional to air gaps.
REFERENCES
[1] F. M. Khan, “The Physics of Radiation Therapy,” Lippin-
cott Williams & Wilkins, Philadelphia, 2010, p. 144.
[2] M. Stroka, J. Reguła and W. Łobodziec, “The Influence
of the Bolus-Surface Distance on the Dose Distribution in
the Build-Up Region,” Reports of Practical Oncology &
Radiotherapy, Vol. 15, No. 6, 2010, pp. 161-164.
doi:10.1016/j.rpor.2010.09.003
[3] K. I. Aneta, Ł. Włodzimierz, D. Marcin, N. Dorota and I.
Tomasz, “Dose Distribution Homogeneity in Two TBI
Techniques—Analysis of 208 Irradiated Patients Con-
ducted in Stanislaw Leszczynski Memorial Hospital, Ka-
towice,” Reports of Practical Oncology & Radiotherapy,
Vol. 17, No. 6, 2012, pp. 367-375.
doi:10.1016/j.rpor.2012.07.013
[4] J. B. Martin, C. Tsang and Y. Peter, “Effects on Skin
Dose from Unwanted Air Gaps under Bolus in Photon
Beam Radiotherapy,” Radiation Measurements, Vol. 32,
No. 3, 2000, pp. 201-204.
doi:10.1016/S1350-4487(99)00276-0
[5] S. H. Hsu, R. Kulasekere and P. L. Roberson, “Analysis
of Variation in Calibration Curves for Kodak XV Radio-
graphic Film Using Model-Based Parameters,” Journal of
Applied Clinical Medical Physics, Vol. 11, No. 4, 2010,
pp. 222-237.
[6] K. Alireza, B. Peter, Y. Ellen, et al., “Beam Spoilers ver-
sus Bolus for 6 mv Photon Treatment of Head and Neck
Cancers,” Medical Dosimetry, Vol. 25, No. 3, 2000, pp.
127-131. doi:10.1016/S0958-3947(00)00038-8
[7] S. H. Hsu, P. L. Roberson, Y. Chen, et al., “Assessment
of Skin Dose for Breast Chest Wall Radiotherapy as a
Function of Bolus Material,” Physics in Medicine & Bi-
ology, Vol. 53, No. 10, 2008, pp. 2593-2606.
doi:10.1088/0031-9155/53/10/010
[8] N. Lee, C. Chuang, J. M. Quivey, et al., “Skin Toxicity
Due to IMRT for Head-and-Neck Carcinoma,” Interna-
tional Journal of Radiation Oncology Biology Physics,
Vol. 53, No. 3, 2002, pp. 630-637.
doi:10.1016/S0360-3016(02)02756-6
[9] P. D. Higgins, E. H. Han, J. L. Yuan and C. K. Lee,
“Evaluation of Surface and Superficial Dose for Head and
Neck Treatments Using Conventional or IMRT Tech-
niques,” Physics in Medicine & Biology, Vol. 52, 2007,
pp. 1135-46. doi:10.1088/0031-9155/52/4/018
[10] N. Dogan and Glasgow, “Surface and Build-Up Region
Dosimetry for Obliquely Incident IMRT 6MV X Rays,”
Medical Physics, Vol. 30, No. 12, pp. 3091-3096.
doi:10.1118/1.1625116
[11] S. Yokoyama, P. L. Roberson, D. W. Litzenberg, et al.,
“Surface Buildup Dose Dependence on Photon Field De-
livery Technique for IMRT,” Journal of Applied Clinical
Medical Physics, Vol. 5, No. 2, 2004, pp. 71-81.
doi:10.1120/jacmp.2020.21706
[12] A. Gray, L. D. Oliver and P. N. Johnston, “The Accuracy
of the Pencil Beam Convolution and Anistropic Ana-
lytical Algorithms in Predicting the Dose Effects Due to
Attenuation from Immobilization Devices and Large Air
Gaps,” Medical Physics, Vol. 36, No. 7, 2009, pp. 3181-
3191. doi:10.1118/1.3147204
[13] A. Kassaee, Y. Xiao, P. Bloch, et al., “Doses near the
Surface during Total-Body Irradiation with 15 MV X-
Rays,” International Journal of Cancer, Vol. 96, 2001, pp.
125-130. doi:10.1002/ijc.10349
Copyright © 2013 SciRes. JCT