 Open Journal of Urology, 2013, 3, 194-199 http://dx.doi.org/10.4236/oju.2013.35036 Published Online September 2013 (http://www.scirp.org/journal/oju) Urologic Laparoscopic Surgeries in Elderly: Analysis of Pre-Operative Risk Factors and Postoperative Complications* Sompol Permpongkosol Division of Urology, Department of Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand Email: sompolpermpong@gmail.com Received June 15, 2013; revised July 18, 2013; accepted July 26, 2013 Copyright © 2013 Sompol Permpongkosol. This is an open access article distributed under the Creative Commons Attribution Li- cense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Purpose: The aging of the population leads to increases in the prevalence of symptomatic urologic diseases. The aim of this study is the analysis of pre-operative risk factors and postoperative complications in patients over the age of 60 years undergoing elective laparoscopic urologic surgery. Patients and Methods: A retrospective study was conducted of 113 patients 60 years of age or older who underwent urologic laparoscopic surgery by a single surgeon (SP). The pre- operative physical status and systemic complications, operation time, postoperative complications, postoperative hospi- tal stay and other clinical features of the patients were reviewed. Complications were classified according to the re- cently revised Clavien classification system. Statistical analysis was done using Univariate analysis and the Fisher Ex- act test. Results: Laparoscopic urologic surgery was performed on 113 patients 60 years old and over, with an average age of 69.6 years. Associated diseases were found in 92% of them. Pelvic surgery (65; 57.5%) was the main reason for surgery. There were 5 (4.4%) conversions to open surgery and 0% mortality. The overall complication rate was 10 pa- tients (8.8%). Among 9 (7.96%) patients with post-operative complications; Grade I, II, IIIa, IIIb and IV complications were observed in 1.77%, 12.8%, 3.53%, 0.88% and 0.88% of cases, respectively. Sex with male, operative time ≥ 250 min and cancer had high risk ratio (2.76, 2.11 and 3.02, respectively); however the correlations of all of preoperative risk factors and postoperative complications showed no statistically significant differences. Conclusions: Laparoscopic surgical treatment of urologic disease in elderly patients performed is feasible and well tolerated, with low perioperative morbidity and a good overall survival rate. Pre-operative risk factors may not influence postoperative complications in patients over the age of 60 years undergoing elective laparoscopic urologic surgery. Keywords: Urologic; Laparoscopic Surgery; Elderly; Complications; Risk Factors; Clavien Classification System 1. Introduction As the life-span of humans has increased, the prevalence of urologic disease has also increased with age. The es- timated population of Thai elderly (60 and over) at the midyear of 2009 was 7,274,000 and life expectancy at sixty for males and females was 19.4 and 21.9, respect- ively [1]. As a result, the number of elderly patients re- quiring urologic surgical procedures, particularly laparo- scopic surgical procedures, is increasing [2]. During the last decade, laparoscopic procedures have increasingly become part of the standard surgical armamentarium in many urological centers and new applications for laparo- scopy continue to be reported [3]. Despite lack of eluci- dation of full-risk profiles, Efron et al. suggested that laparoscopic approaches should be considered regardless of a patient’s age [4]. Therefore, it is important to ana- lyze and continue updating laparoscopic surgical treat- ment in the elderly. To our knowledge, there are many reports of laparo- scopic nephrectomy in elderly patients [5-8]. Neverthe- less, the current role of laparoscopic urologic surgery in older patients, especially in pelvic surgeries, has not been reported. To evaluate pre-operative risk factors and post- operative complications, we reported our experience of laparoscopic urologic surgery, early postoperative mor- bidity and analysis of pre-operative risk factors and post- operative complications in patients over the age of 60 *Conflict of interest: None declared. C opyright © 2013 SciRes. OJU  S. PERMPONGKOSOL 195 years undergoing elective laparoscopic urologic surgery. 2. Patients and Methods We performed a retrospective review of a cohort of 113 consecutive patients who were aged at least 60 years at the time of undergoing laparoscopic urologic procedures, between July 2006 and December 2012 by a single sur- geon (SP). This study was approved by Faculty of Medi- cine, Ramathibodi hospital, Mahidol University Review Board. Parameters examined included patient demo- graphics, preoperative physical status and co-morbidities, complications, estimated blood loss (EBL), operative time, the American Society of Anesthesiologists score (ASA) class, and length of hospitalization were taken from hospital and outpatient records. Complications were defined as in previous reports [9-12]: death was defined as any death that occurred within 30 days or any death at all related to the surgical procedure within 90 days. In addition, all complications were classified according to the Clavien classification system revised by Dindo et al. [13]. The original classi- fication system consisted of four severity grades. The recently revised system emphasizes the risk and inva- siveness of the therapy used to treat a complication and comprises mainly four important modifications: 1) life- threatening complications were differentiated from com- plications treated in the ward; 2) CNS complications were included in the same category (Grade IV); 3) the length of hospital stay is no longer considered in the ranking; and 4) complications that can potentially lead to long-lasting disability are highlighted by a suffix “d” (for “disability”). Consequently the new classification system comprises five severity grades. Age, BMI and operative time are expressed as mean (±SD). Hospital stay, creatinine and EBL are shown as median and range (min-max), because of non-normal distribution, and the categorical variables as percentage. Univariate analysis with Risk ratio (95% confidence in- terval; CI) were performed to analyze the correlation of sex, age, body mass index, ASA score, hospital stay, creatinine, type of surgery, operative time, blood transfu- sion, estimated blood loss and cancer with complications. Fisher’s exact test was performed to analyze the correla- tion of age and operative time, estimated blood loss or hospital stay. A p-value < 0.05 was considered statisti- cally significant. 3. Results The characteristics of patients were listed in Table 1. The majority of laparoscopic urologic surgeries on the elderly in this series are on men (84; 74.3%). The mean patient age was 69.6 yrs (60 - 91 yrs) and the mean body mass index (BMI) was 24.4 kg/m [2] (17.6 - 32.8). Asso- ciated diseases were found in 92% of the patients; the main diseases being hypertension (76; 67.25%) dyslipi- demia (33; 29.2%) and diabetes mellitus type II (29; 25.67%). All cases were done by transperitoneal incision and admitted electively. (Table 2) Non-pelvic surgery (39; 43.5%), pelvic surgery (65; 57.5 %) and both non-pelvic and pelvic simultaneously (9; 7.96%) were undertaken. For non pelvic surgery (39), we performed 17 nephrou- reterectomies (43.6%), 8 nephrectomies (20.5%) and 7 renal cyst ablations (17.95%). Laparoscopic radical pro- statectomy (48; 73.85%) and laparoscopic radical cys- tectomy with ileal conduit (9; 13.85%) respectively were the main pelvic surgeries (65). The mean operative time was 250.8 min (100 - 540 min) and the mean blood loss was 568.7 ml (50 - 3500 ml). Blood transfusion treatment was given to 37 patients (32.7%). The main reasons for conversion to open sur- gery (5; 44%) were technical difficulty and lack of pro- gress with the operation. The overall complication rate was 8.8% (10/113); 1 (0.88%) patient with intraoperative complications included rectal injury. Among 9 (7.96%) patients with post-operative complications; Grade I, II, IIIa, IIIb and IV complications were observed in 1.77%, 12.8%, 3.53%, 0.88% and 0.88% of cases, respectively. Lumbosacral plexopathy [1] and anastomotic urine leak- age were included in Grade I. Grade II included cases of deep vein thrombosis [1]. Urinoma [2], anastomotic stric- tures [1] and postoperative wound infections requiring secondary suture [1] were included in the Grade IIIa category. Grade IIIb included incisional hernia [1]. Sep- sis requiring ICU management in one patient was of Grade IV. Complications were shown sex with male (RR 2.76, 95% CI 0.36 to 21.14, p-value 0.328), operative time ≥ 250 min (RR 2.1, 95% CI 0.6 to 7.44, p-value 0.201), and cancer (RR 3.02, 95% CI 0.39 to 23.19, p-value 0.234) had high risk ratio. However, the correlations of none of the preoperative risk factors or postoperative complications were statistically significant different (Ta- ble 3). When stratified by age < 70 and ≥70 years old, no statistically significant difference was found in opera- tive time, estimated blood loss or hospital stay (Table 4). The mortality rate in our series was 0%. The mean hos- pital stay was 6 (1 - 60) days. 4. Discussion Laparoscopic surgery has proved to be a secure and fea- sible technique in the treatment of benign renal pathol- ogy in pediatric patients with satisfactory results [14-16]. Actually the indications are expanding to reconstructive procedures, with promising results, and selected onco- logic procedures. In contras, several aspects of laparo- t Copyright © 2013 SciRes. OJU 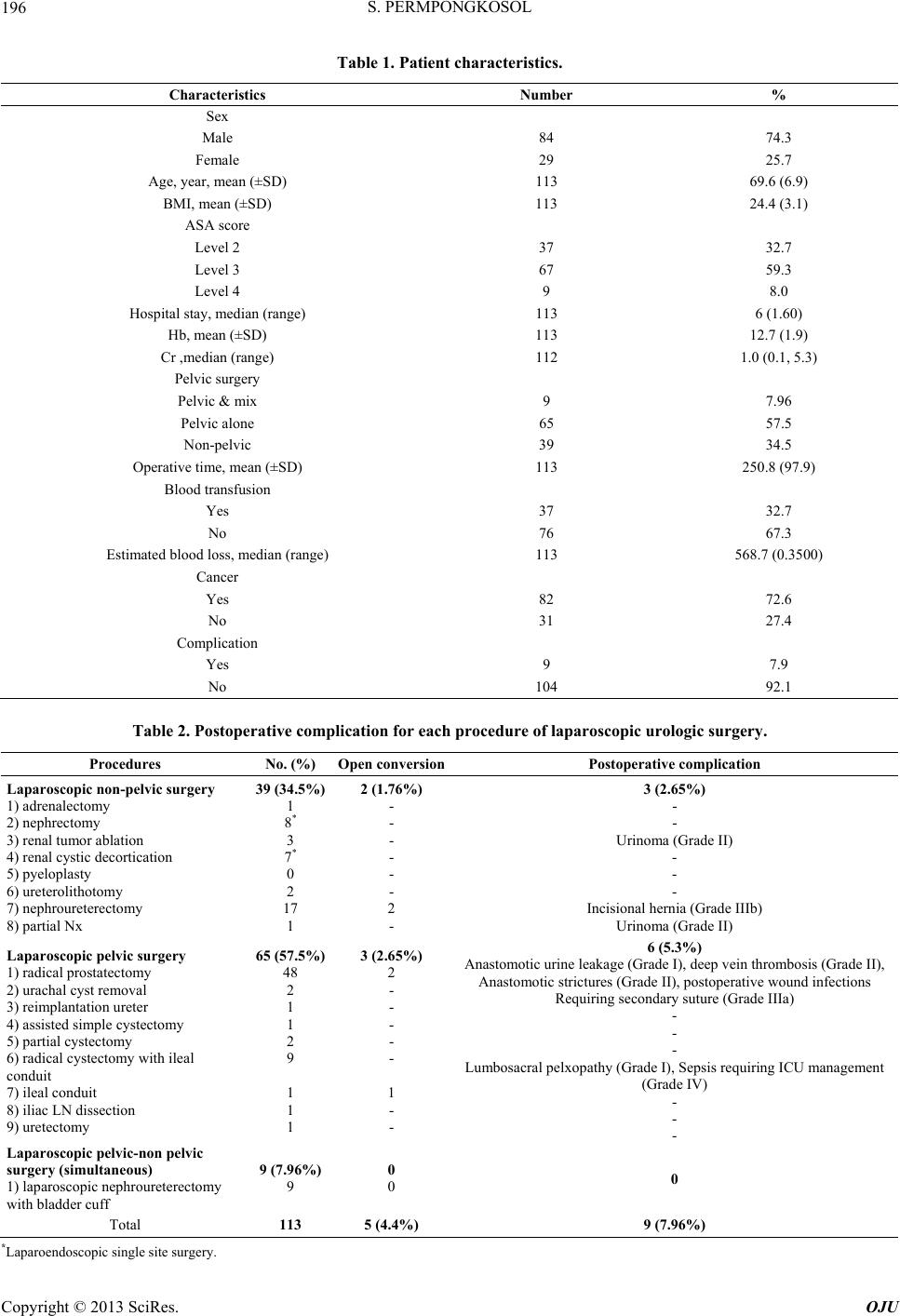 S. PERMPONGKOSOL Copyright © 2013 SciRes. OJU 196 Table 1. Patient characteristics. Characteristics Number % Sex Male 84 74.3 Female 29 25.7 Age, year, mean (±SD) 113 69.6 (6.9) BMI, mean (±SD) 113 24.4 (3.1) ASA score Level 2 37 32.7 Level 3 67 59.3 Level 4 9 8.0 Hospital stay, median (range) 113 6 (1.60) Hb, mean (±SD) 113 12.7 (1.9) Cr ,median (range) 112 1.0 (0.1, 5.3) Pelvic surgery Pelvic & mix 9 7.96 Pelvic alone 65 57.5 Non-pelvic 39 34.5 Operative time, mean (±SD) 113 250.8 (97.9) Blood transfusion Yes 37 32.7 No 76 67.3 Estimated blood loss, median (range) 113 568.7 (0.3500) Cancer Yes 82 72.6 No 31 27.4 Complication Yes 9 7.9 No 104 92.1 Table 2. Postoperative complication for each procedure of laparoscopic urologic surgery. Procedures No. (%) Open conversionPostoperative complication Laparoscopic non-pelvic surgery 1) adrenalectomy 2) nephrectomy 3) renal tumor ablation 4) renal cystic decortication 5) pyeloplasty 6) ureterolithotomy 7) nephroureterectomy 8) partial Nx 39 (34.5%) 1 8* 3 7* 0 2 17 1 2 (1.76%) - - - - - - 2 - 3 (2.65%) - - Urinoma (Grade II) - - - Incisional hernia (Grade IIIb) Urinoma (Grade II) Laparoscopic pelvic surgery 1) radical prostatectomy 2) urachal cyst removal 3) reimplantation ureter 4) assisted simple cystectomy 5) partial cystectomy 6) radical cystectomy with ileal conduit 7) ileal conduit 8) iliac LN dissection 9) uretectomy 65 (57.5%) 48 2 1 1 2 9 1 1 1 3 (2.65%) 2 - - - - - 1 - - 6 (5.3%) Anastomotic urine leakage (Grade I), deep vein thrombosis (Grade II), Anastomotic strictures (Grade II), postoperative wound infections Requiring secondary suture (Grade IIIa) - - - Lumbosacral pelxopathy (Grade I), Sepsis requiring ICU management (Grade IV) - - - Laparoscopic pelvic-non pelvic surgery (simultaneous) 1) laparoscopic nephroureterectomy with bladder cuff 9 (7.96%) 9 0 0 0 Total 113 5 (4.4%) 9 (7.96%) *Laparoendoscopic single site surgery. 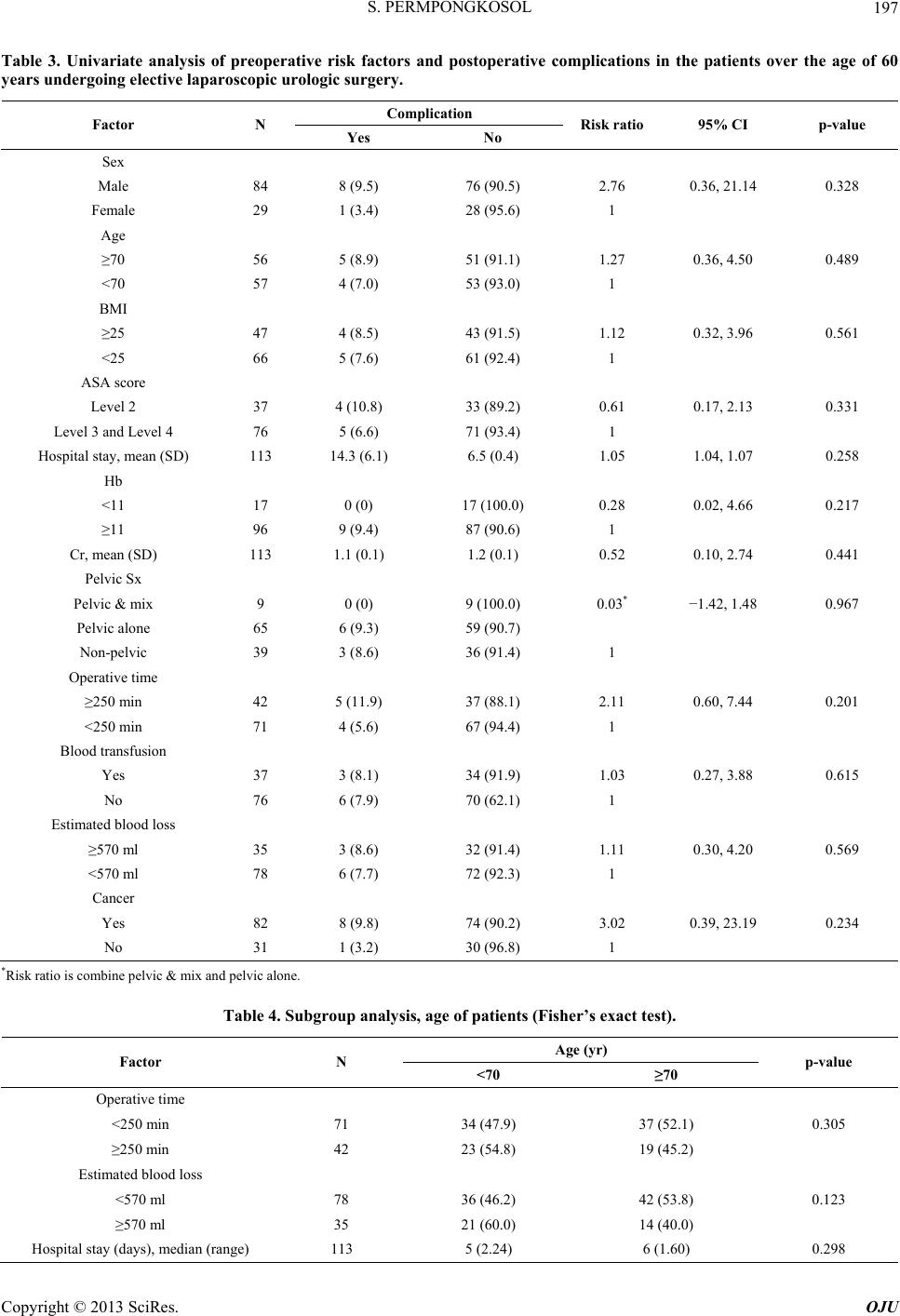 S. PERMPONGKOSOL 197 Table 3. Univariate analysis of preoperative risk factors and postoperative complications in the patients over the age of 60 years undergoing elective laparoscopic urologic surgery. Complication Factor N Yes No Risk ratio 95% CI p-value Sex Male 84 8 (9.5) 76 (90.5) 2.76 0.36, 21.14 0.328 Female 29 1 (3.4) 28 (95.6) 1 Age ≥70 56 5 (8.9) 51 (91.1) 1.27 0.36, 4.50 0.489 <70 57 4 (7.0) 53 (93.0) 1 BMI ≥25 47 4 (8.5) 43 (91.5) 1.12 0.32, 3.96 0.561 <25 66 5 (7.6) 61 (92.4) 1 ASA score Level 2 37 4 (10.8) 33 (89.2) 0.61 0.17, 2.13 0.331 Level 3 and Level 4 76 5 (6.6) 71 (93.4) 1 Hospital stay, mean (SD) 113 14.3 (6.1) 6.5 (0.4) 1.05 1.04, 1.07 0.258 Hb <11 17 0 (0) 17 (100.0) 0.28 0.02, 4.66 0.217 ≥11 96 9 (9.4) 87 (90.6) 1 Cr, mean (SD) 113 1.1 (0.1) 1.2 (0.1) 0.52 0.10, 2.74 0.441 Pelvic Sx Pelvic & mix 9 0 (0) 9 (100.0) 0.03* −1.42, 1.48 0.967 Pelvic alone 65 6 (9.3) 59 (90.7) Non-pelvic 39 3 (8.6) 36 (91.4) 1 Operative time ≥250 min 42 5 (11.9) 37 (88.1) 2.11 0.60, 7.44 0.201 <250 min 71 4 (5.6) 67 (94.4) 1 Blood transfusion Yes 37 3 (8.1) 34 (91.9) 1.03 0.27, 3.88 0.615 No 76 6 (7.9) 70 (62.1) 1 Estimated blood loss ≥570 ml 35 3 (8.6) 32 (91.4) 1.11 0.30, 4.20 0.569 <570 ml 78 6 (7.7) 72 (92.3) 1 Cancer Yes 82 8 (9.8) 74 (90.2) 3.02 0.39, 23.19 0.234 No 31 1 (3.2) 30 (96.8) 1 *Risk ratio is combine pelvic & mix and pelvic alone. Table 4. Subgroup analysis, age of patients (Fisher’s exact test). Age (yr) Factor N <70 ≥70 p-value Operative time <250 min 71 34 (47.9) 37 (52.1) 0.305 ≥250 min 42 23 (54.8) 19 (45.2) Estimated blood loss <570 ml 78 36 (46.2) 42 (53.8) 0.123 ≥570 ml 35 21 (60.0) 14 (40.0) Hospital stay (days), median (range) 113 5 (2.24) 6 (1.60) 0.298 Copyright © 2013 SciRes. OJU  S. PERMPONGKOSOL Copyright © 2013 SciRes. OJU 198 scopy impose unique physiologic stresses and, as such, may alter surgical risk to the geriatric patient [17-19]. The incidence of hypertension, atherosclerosis, and chro- nic pulmonary complications are all elevated in patients aged 65 and older [20,21]. Hypertension is among the diseases that are most significantly increased in our re- port. Therefore, patients should be carefully selected for one of the surgical treatments according to their health, fitness, wishes and the experience of the referred centre. Advanced age is not an absolute contraindication for many laparoscopic procedures. To our knowledge, a lot of cohort studies [2,8] report only non pelvic urologic surgeries in elderly patients. Varkarakis et al. [8] and Lai et al. [7] described outcomes in patients aged 75 years or older undergoing laparoscopic nephrectomy which show- ed no differences in the complication rates, blood loss and operative times [9]. Evaluation of the pre-operative risk factors and post- operative complications are important factors in selecting surgical treatment for elderly patients. Despite the higher percentage of underlying disease in our series, urologic laparoscopy with elderly patients presenting with urinary problems is a safe modality in a university hospital, with no evidence of increased morbidity and mortality. In the current report most of the postoperative complications were Grade II (12.8%) as minor complications. There was only one Grade IV (0.88%) case; which is similar to many reports [22-24]. According to Zhao et al.’s reports [2], overall, there was no statistically significant increase in perioperative complications related to age and patients 75 and older, but they had a significantly longer stay than patients be- tween 65 and 74 years. Our report demonstrated that sex with male, operative time ≥ 250 min and cancer had high risk ratio (2.76, 2.11 and 3.02, respectively). Neverthe- less, there was no correlation of sex, age, body mass in- dex, ASA score, hospital stay, creatinine, type of surgery, operative time, blood transfusion, estimated blood loss and cancer with complications in these studies. Procedures involving pelvic anatomy (urachus, blad- der and prostate bladder) necessitate that the patient is in the Trendelenburg position which will affect cerebro- vascular, respiratory and hemodynamic homeostasis [4, 25]. The complications of laparoscopic pelvic surgery (65; 57.5%) seem to be more than those of laparoscopic non-pelvic surgery in the current report. A major reason for converting to an open procedure, or choosing to perform an open procedure in the first place, is presence of inflammation [4] due to complicated disease. This reason should well explain why the opera- tion was technically difficulty and did not progress in our conversion cases. Conversion should never be regarded as a failure, but as a decision to perform the safest, most- appropriate procedure for a patient, especially for older patients at the highest risk of complications. Our report demonstrated that age has minimal impact on the outcome for elderly patients who undergo laparo- scopic surgery for urologic disease. When stratified by age < 70 and ≥70 years old, no statistically significant difference was found in operative time, estimated blood loss or hospital stay. There are limitations with regard to the small sample, but this study is the first report of la- paroscopic urologic surgery in elderly patients that speci- fies the type of surgeries as pelvic and non-pelvic sur- geries. 5. Conclusion Laparoscopic surgery is a safe and accepted procedure in patients over 60 years of age with urologic disease. There was no significant increase in perioperative complica- tions related to age, and pre-operative risk factors may not influence postoperative complications in patients over the age of 60 years undergoing elective laparoscopic urologic surgery. 6. Acknowledgements The author thanks Terry King for his assistance prepar- ing the article and Assoc. Prof. Sasitorn Yongcharoen for the statistical analysis. REFERENCES [1] Institute for Population and Social Research MU, “All about Population,” 2009. www.ipsr.mahidol.ac.th [2] L. C. Zhao, R. A. Rubenstein, I. Y. Vardi, C. Tenggard- jaja, N. Smith and R. B. Nadler, “Effect of Advanced Age on Laparoscopic Urologic Procedures,” Journal of En- dourology, Vol. 21, No. 1, 2007, pp. 62-64. doi:10.1089/end.2006.9997 [3] R. Ganzer, R. Rabenalt, M. C. Truss, S. Papadoukakis, M. Do, A. Blana, et al., “Evaluation of Complications in En- doscopic Extraperitoneal Radical Prostatectomy in a Mo- dular Training Programme: A Multicentre Experience,” World Journal of Urology, Vol. 26, No. 6, 2008, pp. 587- 593. doi:10.1007/s00345-008-0291-y [4] D. T. Efron and J. S. Bender, “Laparoscopic Surgery in Older Adults,” Journal of the American Geriatrics Soci- ety, Vol. 49, No. 5, 2001, pp. 658-663. doi:10.1046/j.1532-5415.2001.49130.x [5] M. Harano, M. Eto, A. Yokomizo, K. Tatsugami, M. Hamaguchi and S. Naito, “The Efficacy of Laparoscopic Radical Nephrectomy for Renal Cell Cancer in the Eld- erly: An Oncological Outcome Analysis,” International Journal of Urology, Vol. 15, No. 7, 2008, pp. 577-581. doi:10.1111/j.1442-2042.2008.02054.x [6] T. H. Hsu, L. M. Su, L. E. Ratner and L. R. Kavoussi, “Laparoscopic Donor Nephrectomy in the Elderly Pa- tient,” Urology, Vol. 60, No. 3, 2002, pp. 398-401. doi:10.1016/S0090-4295(02)01769-7  S. PERMPONGKOSOL 199 [7] F. C. Lai, E. L. Kau C. S. Ng and G. J. Fuchs, “Laparo- scopic Nephrectomy Outcomes of Elderly Patients in the 21st Century,” Journal of Endourology, Vol. 21, No. 11, 2007, pp. 1309-1313. doi:10.1089/end.2007.9885 [8] I. Varkarakis, R. Neururer, T. Harabayashi, G. Bartsch and R. Peschel, “Laparoscopic Radical Nephrectomy in the Elderly,” BJU International, Vol. 94, No. 4, 2004, pp. 517-520. doi:10.1111/j.1464-410X.2004.04994.x [9] S. Permpongkosol, P. Ungbhakorn and C. Leenanupunth, “Laparo-Endoscopic Single Site (LESS) Management of Benign Kidney Diseases: Evaluation of Complications,” Journal of the Medical Association of Thailand, Vol. 94, No. 1, 2011, pp. 43-49. [10] S. Permpongkosol, G. C. Lima, C. A. Warlick, M. E. Allaf, I. M. Varkarakis, H. S. Bagga, et al., “Postchemo- therapy Laparoscopic Retroperitoneal Lymph Node Dis- section: Evaluation of Complications,” Urology, Vol. 69, No. 2, 2007, pp. 361-365. doi:10.1016/j.urology.2006.10.020 [11] S. Permpongkosol, R. E. Link, L. M. Su, F. R. Romero, H. S. Bagga, C. P. Pavlovich, et al., “Complications of 2775 Urological Laparoscopic Procedures: 1993 to 2005,” Journal of Urology, Vol. 177, No. 2, 2007, pp. 580-585. doi:10.1016/j.juro.2006.09.031 [12] G. H. Ballantyne, J. Svahn, R. F. Capella, J. F. Capella, H. J. Schmidt, A. Wasielewski, et al., “Predictors of Pro- longed Hospital Stay Following Open and Laparoscopic Gastric Bypass for Morbid Obesity: Body Mass Index, Length of Surgery, Sleep Apnea, Asthma, and the Meta- bolic Syndrome,” Obesity Surgery, Vol. 14, No. 8, 2004, pp. 1042-1050. doi:10.1381/0960892041975460 [13] D. Dindo, N. Demartines and P. A. Clavien, “Classifica- tion of Surgical Complications: A New Proposal with Evaluation in a Cohort of 6336 Patients and Results of a Survey,” Annals of Surgery, Vol. 240, No. 2, 2004, pp. 205-213. doi:10.1097/01.sla.0000133083.54934.ae [14] J. Dingemann and B. M. Ure, “Systematic Review of Level 1 Evidence for Laparoscopic Pediatric Surgery: Do Our Procedures Comply with the Requirements of Evi- dence-Based Medicine?” European Journal of Pediatric Surgery, 2013 Feb 26. [15] R. Vecchio, S. Marchese and E. Intagliata, “Pediatric Laparoscopic Splenectomy in a Department of General Surgery,” Updates in Surgery, 2012 Nov 30. [16] F. T. Denes, A. Tavares, E. D. Monteiro, J. de Bessa Jr., A. M. Giron, F. A. Queiroz Filho, et al., “Laparoscopic renal Surgery in Infants and Children: Is It a Feasible and Safe Procedure for All Pediatric Age Groups?” Interna- tional Brazilian Journal of Urology, Vol. 34, No. 6, 2008, pp. 739-746. doi:10.1590/S1677-55382008000600009 [17] J. Majeski, “Laparoscopic Cholecystectomy in Geriatric Patients,” The American Journal of Surgery, Vol. 187, No. 6, 2004, pp. 747-750. doi:10.1016/j.amjsurg.2003.11.031 [18] P. Fornara, C. Doehn and D. Jocham, “Laparoscopic Ne- phrectomy in Geriatric Patients: Comparison with Con- ventional Nephrectomy,” Zeitschrift für Gerontologie und Geriatrie, Vol. 33, No. 5, 2000, pp. 388-395. doi:10.1007/s003910070036 [19] J. M. Velasco, V. L. Vallina, D. J. Esposito and S. Theo- dore, “Laparoscopic Herniorrhaphy in the Geriatric Popu- lation,” The American Journal of Surgery, Vol. 64, No. 7, 1998, pp. 633-637. [20] J. A. Lujan, F. Sanchez-Bueno, P. Parrilla, R. Robles, J. A. Torralba and R. Gonzalez-Costea, “Laparoscopic vs Open Cholecystectomy in Patients Aged 65 and Older,” Surgical Laparoscopy & Endoscopy, Vol. 8, No. 3, 1998, pp. 208-210. doi:10.1097/00019509-199806000-00009 [21] I. Gunka, J. Dostalik, L. Martinek, P. Gunkova, M. Mazur and P. Vavra, “Advanced Age—Indication or Contrain- dication for Laparoscopic Colorectal Surgery?” Rozhledy v Chirurgii, Vol. 89, No. 10, 2010, pp. 628-633. [22] M. Burchardt and J. U. Stolzenburg, “Complications in Laparoscopic Urology,” World Journal of Urology, Vol. 26, No. 6, 2008, pp. 521-522. doi:10.1007/s00345-008-0353-1 [23] C. C. Passerotti, H. T. Nguyen, A. B. Retik and C. A. Peters, “Patterns and Predictors of Laparoscopic Compli- cations in Pediatric Urology: The Role of Ongoing Sur- gical Volume and Access Techniques,” Journal of Urol- ogy, Vol. 180, No. 2, 2008, pp. 681-685. doi:10.1016/j.juro.2008.04.042 [24] G. Vallancien, X. Cathelineau, H. Baumert, J. D. Doublet and B. Guillonneau, “Complications of Transperitoneal Laparoscopic Surgery in Urology: Review of 1311 Pro- cedures at a Single Center,” Journal of Urology, Vol. 168, No. 1, 2002, pp. 23-26. doi:10.1016/S0022-5347(05)64823-9 [25] D. M. Gainsburg, “Anesthetic Concerns for Robotic-As- sisted Laparoscopic Radical Prostatectomy,” Minerva Anestesiologica, Vol. 78, No. 5, 2012, pp. 596-604. Copyright © 2013 SciRes. OJU
|