A. Mushtaq et al. / Advances in Bioscience and Biotechnology 4 (2013) 866-871
870
the prognosis of HCV infection. One study showed that
serum ALT levels, especially the AST levels were cou-
pled with liver damage [26]. Usually it is considered that
patients with chronic HCV having high HCV RNA titers
and abnormal ALT levels show active HCV reproduction
in liver and have higher risk of liver injury. Moreover,
ALT level is used for indication of histological liver
damage and a factor for starting therapy or to check anti-
viral therapy response in chronic hepatitis C [27]. We
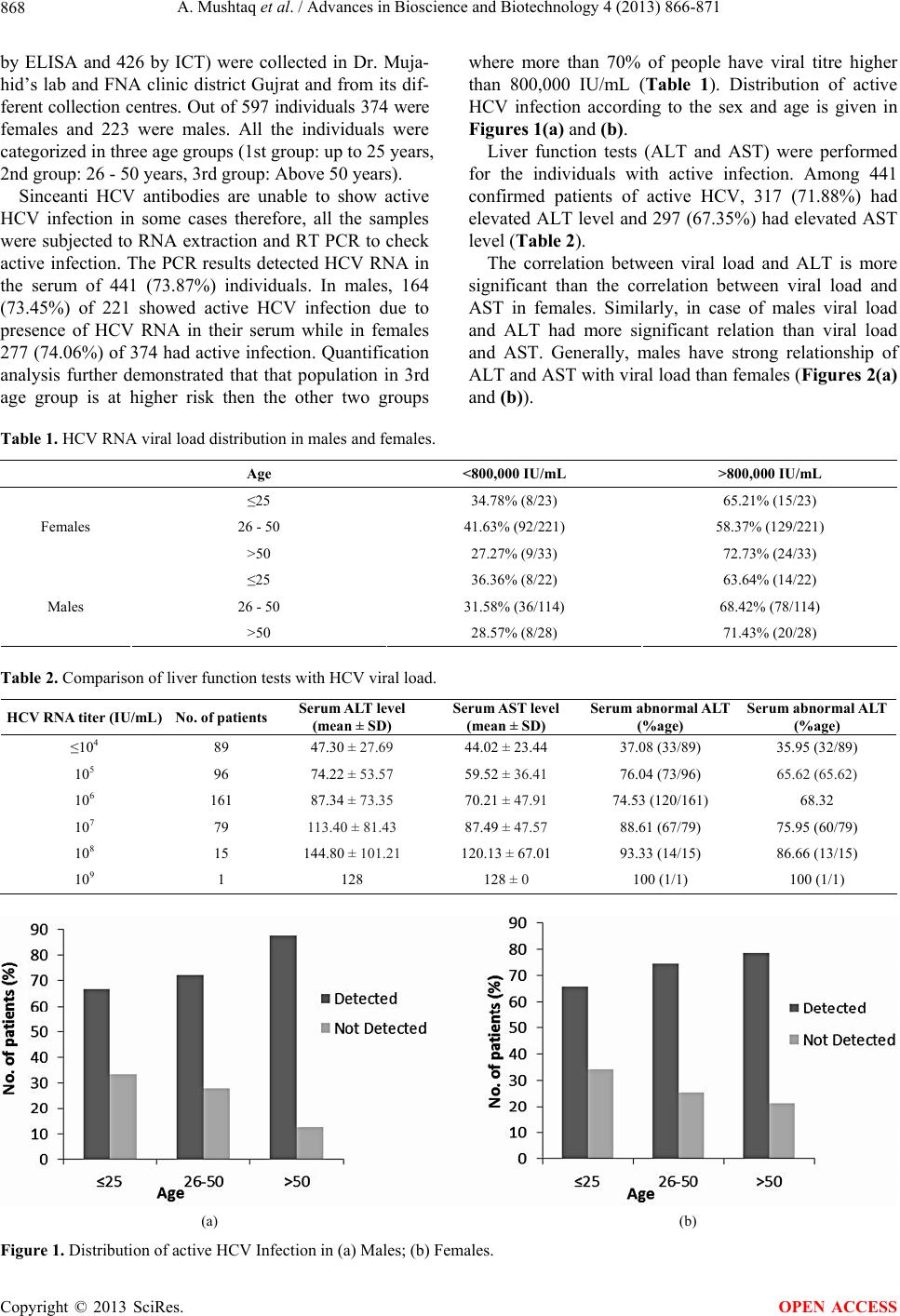
found that 71.88% patients with active HCV infection
had elevated ALT level in their sera. As there are almost
25% of patients with active HCV infection having per-
sistently normal ALT values [18]. We found 67.35% indi-
viduals with active HCV infection having elevated AST
levels.
Patients with low viral load have 2.7 times more inci-
dence of SVR than individuals with high viral load [28].
It is also prominent that individuals with high viral load
show decreased response to antiviral therapy than indi-
viduals with low viral load and early prognosis reveals
low HCV RNA viral load. Patients with high viral load
should be treated for 24 weeks and those with low viral
load might be treated for 16 weeks if there HCV RNA
PCR is undetectable at 4th week of treatment [29,30].
Our results indicate that 36.5% (161/441) have low viral
load while 63.49% (280/441) have high viral load.
5. CONCLUSION
The prevalence of active HCV infection in anti HCV
individuals increases with the increase in age. Individu-
als up to 25 years had less number of anti HCV antibod-
ies and HCV RNA in their blood while with the increase
in age the chances of active HCV infection increase and
viral load also increases. Individuals with age >50 years
have highest percentage of HCV RNA titer in anti HCV
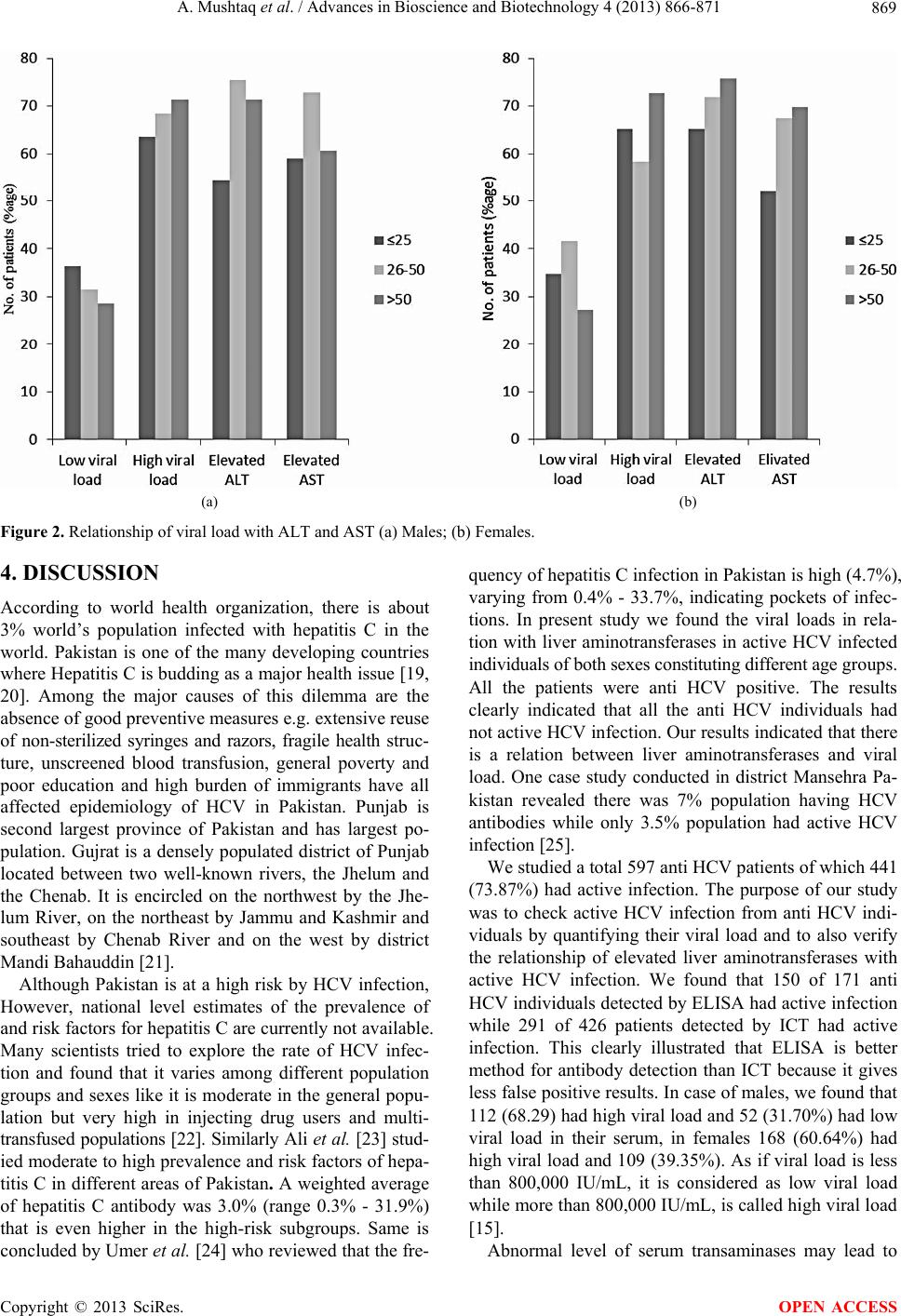
individuals. The viral load has a strong relationship with
liver enzymes (ALT and AST). With the increase in viral
load, the ALT and AST levels also increase in most cases
but in some cases of active HCV infection ALT and AST
levels remain normal.
6. ACKNOWLEDGEMENTS
We acknowledge support by the German Research Foundation and the
Open Access Publication Funds of the Göttingen University.
REFERENCES
[1] Alter, H.J. and Seeff, L.B. (2000) Recovery, persistence.
and sequelae in hepatitis C virus infection: A perspective
on long-term outcome. Seminars in Liver Disease, 20, 17-
35. doi:10.1055/s-2000-9505
[2] Freeman, A.J., Dore, G.J., Law, M.G., Thorpe, M., Von
Overbeck, J., Lloyd, A.R., Marinos, G. and Kaldor, J.M.
(2001) Estimating progression to cirrhosisin chronic he-
patitis C virus infection. Hepatology, 34, 809-816.
doi:10.1053/jhep.2001.27831
[3] Smith, D.B., Mellor, J., Jarvis, L.M., et al. (1995) Varia-
tion of the hepatitis C virus 5’ non-coding region: Impli-
cations for secondary structure, virus detection and typing:
The International HCV Collaborative Study Group. Jour-
nal of General Virology, 76, 1749-1761.
doi:10.1099/0022-1317-76-7-1749
[4] Global Burden of Disease (GBD) for Hepatitis (2004)
The Global Burden of Hepatitis C Working Group. Phar-
macology, 44, 20-29.
[5] El-Zanaty, F. and Way, A. (2009) Egypt demographic
and health survey 2008. Ministry of Health, El-Zanaty
and Associates, and Macro International, Cairo.
[6] Williams, I. (1999) Epidemiology of hepatitis C in the
United States. American Journal of Medicine, 107, 2S-9S.
doi:10.1016/S0002-9343(99)00373-3
[7] Waheed, Y., Shafi, T., Safi, S.Z. and Qadri, I. (2009)
Hepatitis C virus in Pakistan: A systematic review of pre-
valence, genotypes and risk factors. World Journal of
Gastroenterology, 15, 5647-5653.
doi:10.3748/wjg.15.5647
[8] Caritter, R.L. and Emerson, S.S. (1997) Therapy of hepa-
titis—Meta analysis of interferon alpha 2b trials. Hepa-
tology, 26, 835-885.
[9] Fox, R.K. and Wright, T.L. (2003) Viral hepatitis: Cur-
rent diagnosis and treatment. Gastroenterology, 2, 446-
562.
[10] Sherman, M., Shafran, S., Burak, K., Doucette, K., Wong,
W., Girgrah, N., Yoshida, E., Renner, E., Wong, P. and
Deschênes, M. (2007) Management of chronicnhepatitis
C: Consensus guidelines. Canadian Journal of Gastroen-
terology, 21, 25C-34C.
[11] Yoshioka, K., Kakumu, S. and Wakita, T. (1992) Detec-
tion of hepatitis C virus bypolymerase chain reaction and
response to interferon-a therapy: Relationship to geno-
types of hepatitis C virus. Hepatology, 16, 293-299.
doi:10.1002/hep.1840160203
[12] Ahmad, W., Ijaz, B., Javed, T.F., Jahan, S., Shahid, I.,
Khan, F.M. and Hassan, S. (2010) HCV genotype distri-
bution and possible transmission risks in Lahore, Pakistan.
World Journal of Gastroenterology, 16, 4321-4328.
doi:10.3748/wjg.v16.i34.4321
[13] Lee, Y.S., Yoon, S.K., Chung, E.S., Bae, S.H., Choi, J.Y.,
Han, J.Y., Chung, K.W., Sun, H.S., Kim, B.S. and Kim,
B.K. (2001) The relationship of histologic activity to se-
rum ALT, HCV genotype and HCV RNA titers in chro-
nic hepatitis C. Journal of Korean Medical Science, 16,
585-591.
[14] Dienstag, J.L. and Alter, H.J. (1986) Non-A, non-B hepa-
titis: Evolving epidemiologic and clinical perspective.
Seminars in Liver Disease, 6, 67-81.
doi:10.1055/s-2008-1040795
[15] Tassopoulos, N.C. (1999) Treatment of patients with
chronic hepatitis C and normal ALT levels. Journal of
Hepatology, 31, 193-196.
doi:10.1016/S0168-8278(99)80400-0
[16] Carreno, V. (2006)Occult hepatitis C virus infection: A
Copyright © 2013 SciRes. OPEN ACCESS