Vol.1, No.1, 1-3 (2013) Open Journal of Therapy and Rehabilitation
http://dx.doi.org/10.4236/ojtr.2013.11001
Sitting position improves consciousness level in
patients with cerebral disorders
Takashi Moriki1, Takeshi Nakamura 1*, Daisuke Kojima1, Hiroy oshi Fujiwara2, Fumihiro Ta jima 1
1Department of Rehabilitation Medicine, Wakayama Medical University, Wakayama, Japan;
*Corresponding Author: take-n@wakayama-med.ac.jp
2Department of Orthopedics, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kyoto, Japan
Received 2 May 2013; revised 3 June 2013; accepted 12 June 2013
Copyright © 2013 Takashi Moriki et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Cerebral disorders are of ten associated with dis-
turbance of consciousness. Since the latter could
alter the prognosis of physical function, early
improvement of consciousness level is impor-
tant. The present study tested the hypothesis
that sitting position improves disturbances of
consciousness in patients with cerebral disor-
ders. The subject s were 17 p atient s with cerebra l
disorders and disturbances of consciousness.
The consciousness level was evaluated in su-
pine position and following a change to sitting
position. The consciousness level was evalu-
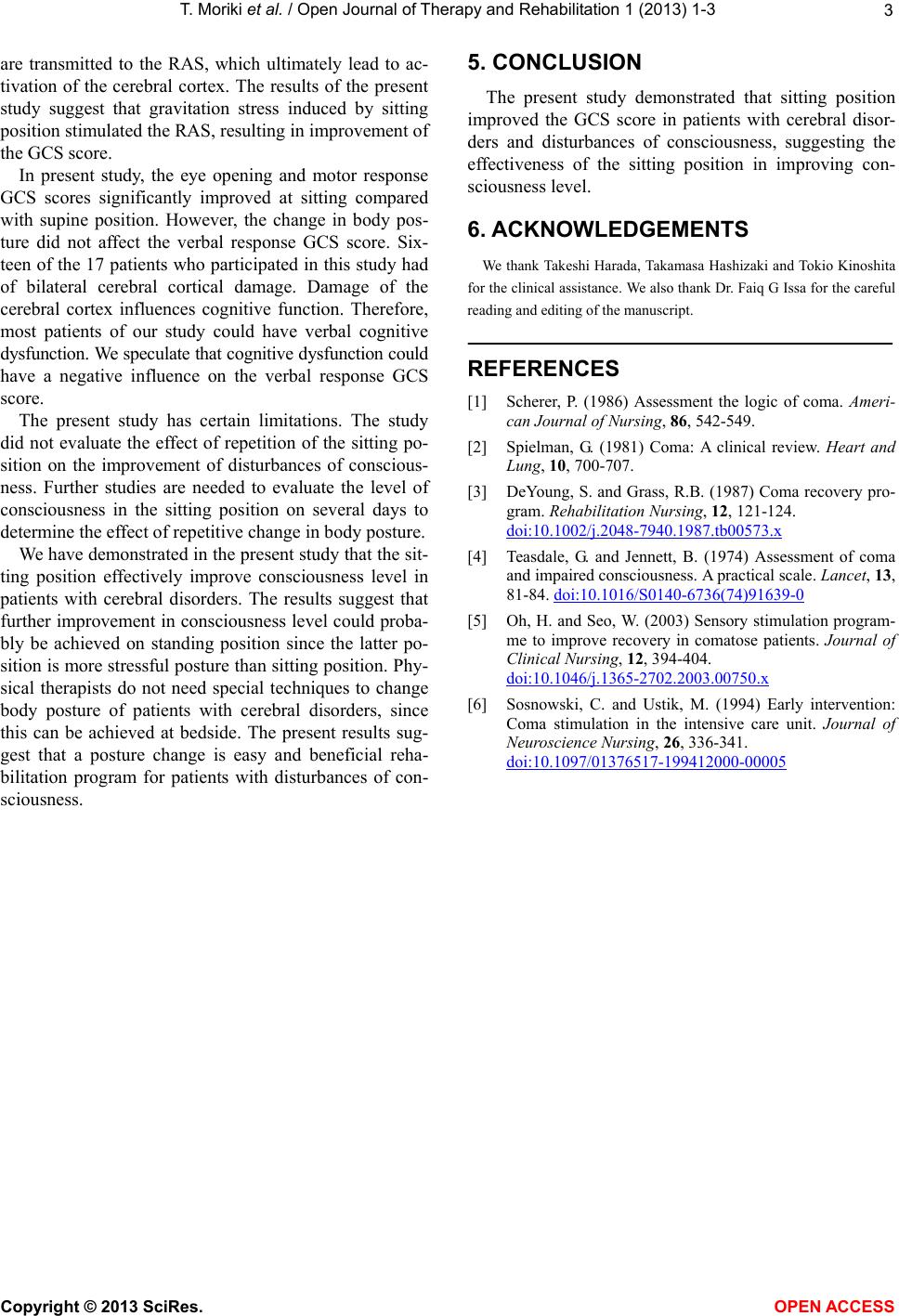
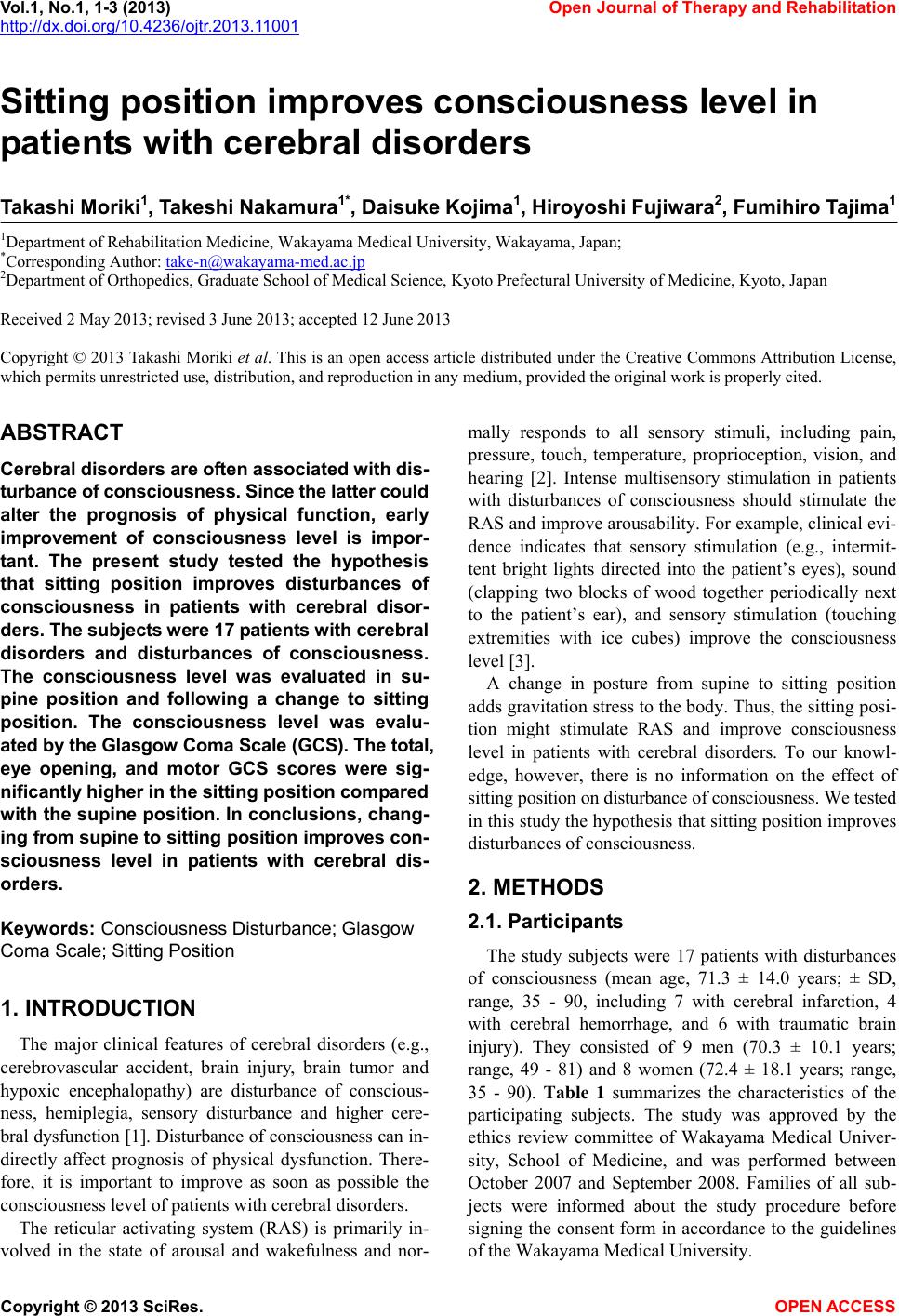
ated by the Glasgow Coma Scale (GCS). The tot al,
eye opening, and motor GCS scores were sig-
nificantly higher in the sitting position compared
with the supine position. In conclusions, chang-
ing from supine to sitting position impro ves con-
sciousness level in patients with cerebral dis-
orders.
Keywords: Consciousness Disturban ce ; Glasgow
Coma Scale; Sitting Position
1. INTRODUCTION
The major clinical features of cerebral disorders (e.g.,
cerebrovascular accident, brain injury, brain tumor and
hypoxic encephalopathy) are disturbance of conscious-
ness, hemiplegia, sensory disturbance and higher cere-
bral dysfunction [1]. Disturbance of consciousness can in-
directly affect prognosis of physical dysfunction. There-
fore, it is important to improve as soon as possible the
consciousness level of patients with cerebral disorders.
The reticular activating system (RAS) is primarily in-
volved in the state of arousal and wakefulness and nor-
mally responds to all sensory stimuli, including pain,
pressure, touch, temperature, proprioception, vision, and
hearing [2]. Intense multisensory stimulation in patients
with disturbances of consciousness should stimulate the
RAS and improve arousabilit y. For example, clinical evi-
dence indicates that sensory stimulation (e.g., intermit-
tent bright lights directed into the patient’s eyes), sound
(clapping two blocks of wood together periodically next
to the patient’s ear), and sensory stimulation (touching
extremities with ice cubes) improve the consciousness
level [3].
A change in posture from supine to sitting position
adds gravitation stress to the body. Thus, the sitting p osi-
tion might stimulate RAS and improve consciousness
level in patients with cerebral disorders. To our knowl-
edge, however, there is no information on the effect of
sitting position on disturbance of consciousness. We tested
in this study the hypo thesis that sitting pos ition improves
disturbances of consci o us ness.
2. METHODS
2.1. Participants
The study subjects were 17 patients with disturbances
of consciousness (mean age, 71.3 ± 14.0 years; ± SD,
range, 35 - 90, including 7 with cerebral infarction, 4
with cerebral hemorrhage, and 6 with traumatic brain
injury). They consisted of 9 men (70.3 ± 10.1 years;
range, 49 - 81) and 8 women (72.4 ± 18.1 years; range,
35 - 90). Table 1 summarizes the characteristics of the
participating subjects. The study was approved by the
ethics review committee of Wakayama Medical Univer-
sity, School of Medicine, and was performed between
October 2007 and September 2008. Families of all sub-
jects were informed about the study procedure before
signing the consent form in accordance to the guidelines
of the Wakayama Medical University.
Copyright © 2013 SciRes. OPEN ACCESS