K. W. Kang et al. / Case Reports in Clinical Medicine 2 (2013) 345-347
Copyright © 2013 SciRes. Openly accessible at http://www.sc irp.or g/journal/crcm/
347
setting of an extravascular infection in an immunocom-
promised host [8]. In the present case, the patient with
poorly controlled diabetes complained of only ocular
symptom and brain CT showed no infectious cerebral
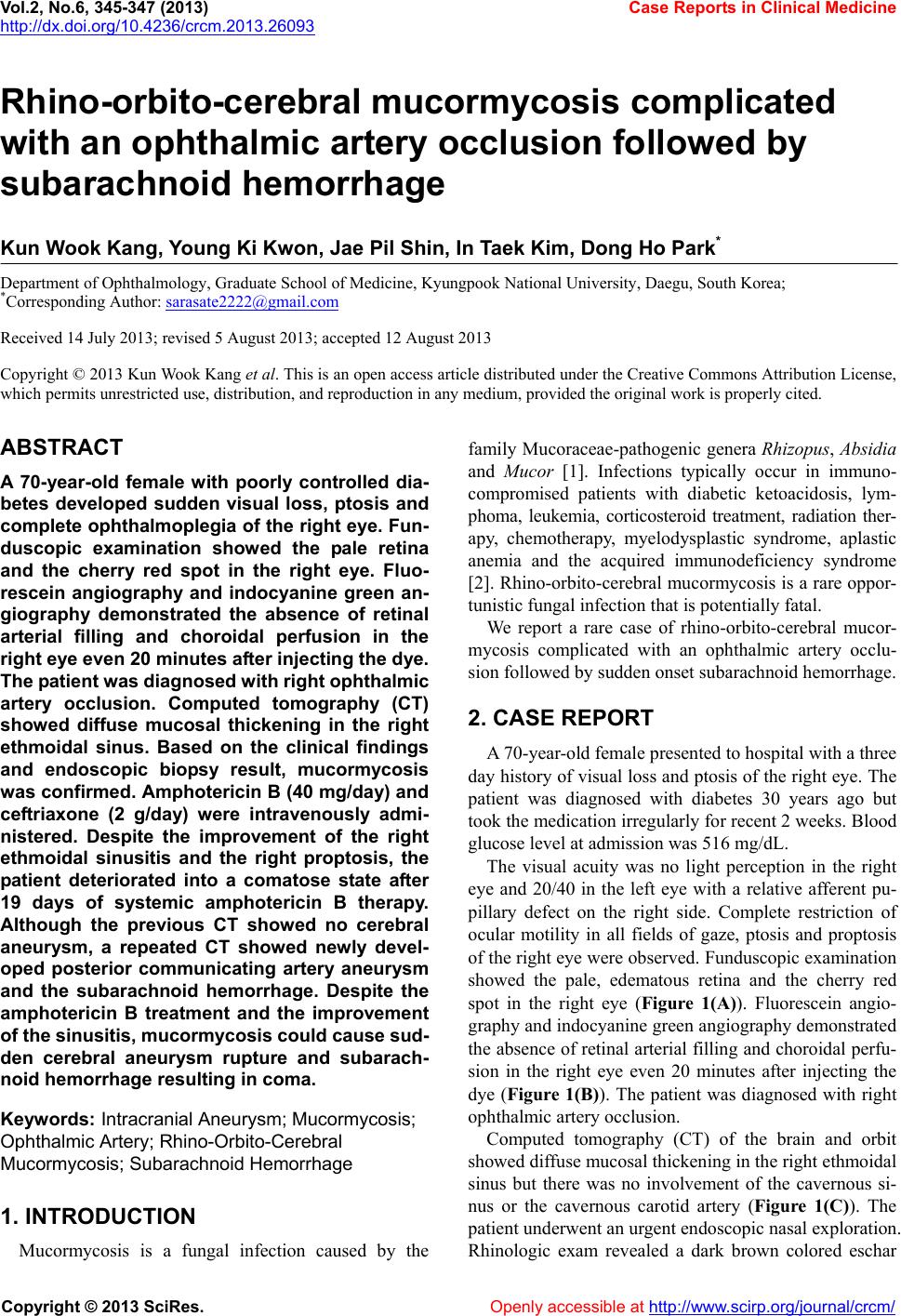
aneurysm at admission. After 9 days of systemic ampho-
tericin B therapy, brain CT showed the improvement of
the proptosis of the right eye and the resolution of mu-
cosal thickening of ethmoidal sinus. However, 19 days
after systemic amphotericin B therapy, the patient dete-
riorated into a comatose state. Brain CT showed the dif-
fuse subarachnoid hemorrhage with a right temporal lobe
hematoma due to ruptured aneurysm. Within 19 days,
new cerebral aneurysm developed and progressed rapidly.
It supported our su spicion of a fungal aneur ysm.
REFERENCES
[1] Koc, Z., Koc, F., Yerdelen, D. and Ozdogu, H. (2007)
Rhino-orbital-cerebral mucormycosis with different cere-
bral involvements: Infarct, hemorrhage, and ophthalmo-
plegia. International Journal of Neuroscience, 117, 1677-
1690. doi:10.1080/00207450601050238
[2] Haliloglu, N.U., Yesilirmak, Z., Erden, A. and Erden, I.
(2008) Rhino-orbito-cerebral mucormycosis: Report of
two cases and review of the literature. Dentomaxillofacial
Radiology, 37, 161-166. doi:10.1259/dmfr/14698002
[3] Yang, S.W., Kim, S.Y., Chung, J. and Kim, K.B. (2000)
Two cases of orbital infarction syndrome. Korean Journal
of Ophthalmology, 14, 107-111.
[4] Hussain, S., Salahuddin, N., Ahmad, I., Salahuddin, I. and
Jooma, R. (1995) Rhinocerebral invasive mycosis: Oc-
currence in immunocompetent individuals. European Jour-
nal of Radiology, 20, 151-155.
doi:10.1016/0720-048X(95)00644-6
Survival of mucormycosis with intracerebral involve-
ment was thought to be virtually impossible un til the first
case of clinical recovery reported in 1955 [9]. The intro-
duction of amphotericin B in the 1960s reduced mortality
from 70% to 40% [10]. Nevertheless, the prognosis of
rhino-orbito -cerebral mucormycosis remains poo r and 20
to 50% of patients expire [11]. In the present case, the
ethmoidal sinusitis and the proptosis of the right eye
were improved after amphotericin B treatment. However
the subarachnoid hemorrhage due to ruptured aneurysm
occurred in a short period. Although endovascular coil
embolization of posterior communicating artery and cra-
niotomy for subarachnoid hemorrhage were performed,
the patient was still comatose.
[5] Zimmerman, C.F., Van Patten, P.D., Golnik, K.C., Kopit-
nik Jr., T.A. and Anand, R. (1995) Orbital infarction syn-
drome after surgery for intracranial aneurysms. Ophthal-
mology, 102, 594-598.
[6] Chimelli, L. and Mahler-Araujo, M.B. (1997) Fungal
infections. Brain Pathology, 7, 613-627.
d oi:1 0.1111/j .1750-3639.1997.tb01078.x
[7] Peterus, T., Teguh, T. and Daofu, D. (2004) Fatal strokes
in patients with rhino-orbito-cerebral mucormycosis and
associated vasculopathy. Scandinavian Journal of Infec-
tious Diseases, 36, 643-648.
doi:10.1080/00365540410020794
In conclusion, systemic amphotericin B antifungal
treatment improves the sinusitis and the proptosis. Nev-
ertheless, new cerebral aneurysm can develop in a short
period and it can cause subarachnoid hemorrhage. Oph-
thalmologists shou ld raise the suspicion of the infectious
mycotic cerebral aneurysm and the subarachnoid hem-
orrhage resulting in coma, even if the sinusitis is im-
proved after amphotericin B treatment.
[8] Asari, S., Nishimoto, A. and Murakami, M. (1988) A rare
case of cerebral aspergillus aneurysm at the site of tem-
porary clip application. No Shinkei Geka, 16, 1079-1082.
[9] Harris, J.S. (1955) Mucormycosis; report of a case. Pedi-
atrics, 16, 857-867.
[10] Shah, P.D., Peters, K.R. and Reuman, P.D. (1997) Recov-
ery from rhinocerebral mucormycosis with carotid artery
occlusion: A pediatric case and review of the literature
Pediatric Infectious Disease Journal, 16, 68-71.
doi:10.1097/00006454-199701000-00015
4. ACKNOWLEDGEMENTS
This research was supported by the Basic Science Research Program
through the National Research Foundation of Korea (NRF) funded by
the Ministry of Education, Science and Technology (2012004585) and
by the Korea Health Technology R&D Project, Ministry of Health &
Welfare, Repu blic of Korea (A111345).
[11] Toumi, A., Larbi Ammari, F., Loussaief, C., Hadhri, R.,
Ben Brahim, H., Harrathi, K., Ben Romdhane, F., Koubaa,
J. and Chakroun, M. (2012) Rhino-orbito-cerebral mucor-
mycosis: Five cases. Médecine et Maladies Infectieuses,
42, 591-598. doi:10.1016/j.medmal.2012.10.001