Vol.2, No.6, 341-344 (2013) Case Reports in Clinical Medicine
http://dx.doi.org/10.4236/crcm.2013.26092
Glottic foreign bodies in infants: A series of
four cases
Aayush Mittal1*, Rahul Bhargava2, Sunil Kumar2, Jatinder Kumar Sahni2
1Department of Otorhinolaryngology-Head & Neck Surgery, Hind Institute of Medical Sciences & Shekhar Hospital, Lucknow, India;
*Corresponding Author: aayush_mittal@yahoo.com
2Department of Otorhinolaryngology-Head & Neck Surgery, Lady Hardinge Medical College, New Delhi, India;
dr.rahul.bhargava@gmail.com, suku321@rediffmail.com, drjksahni@yahoo.co.in
Received 9 July 2013; revised 5 August 2013; accepted 12 August 2013
Copyright © 2013 Aayush Mittal et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Foreign body in glottis especially in infants is
rare. Retrieval of foreign body is a rather simple
procedure but sharing of the airway with the
anaesthetist and impeding complication makes
it more challenging and dangerous. Making a
diagnosis of foreign body is most challenging in
delayed cases. Complete history and detailed phy-
sical examination along with high index of sus-
picion, in cases of persistent cough, fever, non-
resolving respiratory infection, are needed to
rule out airway especially laryngeal foreign body.
This series of 4 cases is being reported because
of the rarity of the glott is fore ign b od y in infants.
Keyw ords: Foreign Body; Bronchoscop y ; Infant;
Glottis
1. INTRODUCTION
Aspiration of foreign bodies in trachea-bronchial tree
is common. Most patients are younger than 4 years old
[1]. In literature, incidence of foreign body of the larynx
has been reported from 0.7% to 6.1% among all aero-di-
gestive foreign bodies [2-4]. Delay in diagnosis of the
foreign body in airway has the potential to make a diffi-
cult situation even more serious [5].
2. PATIENTS AND METHODS
We reviewed the data of 79 patients with suspected
history of foreign body aspiration who presented to the
ENT casualty and pediatric emergency during a period of
one year from August 2011 to August 2012.
3. RESULTS
In 6/79 (7.59%) patients foreign bodies were retrieved
from glottis, in among these 4/6 (66.67%) patients were
under the age group of one year. All the four patients
presented with the complaint of breathing difficulty of
two days to two months duration (Table 1). Two of them
had a history of choking and change in voice while two
of them had a history of coughing and cyanosis. One of
the patients was being treated for upper respiratory tract
infection in some peripheral hospital with antibiotics and
nebulisation for two months. Another patient was re-
ferred from the pediatric department for non-resolving
respiratory distress of more than one week, the child had
undergone fibreoptic laryngoscopy and was reported to
be normal.
On examination all children were having respiratory
distress of varying proportion however apparent suprast-
ernal and intercostal retractions with biphasic stridor was
present in 2 of the patients. Children were afebrile hav-
ing no cyanosis. No abnormal cry or palpatory thud was
noted over the trachea in any case. On auscultation bilat-
eral air entry was equal in all cases with conducted sound
in 2 cases. Rest of ENT examination as well as systemic
examination was unremarkable.
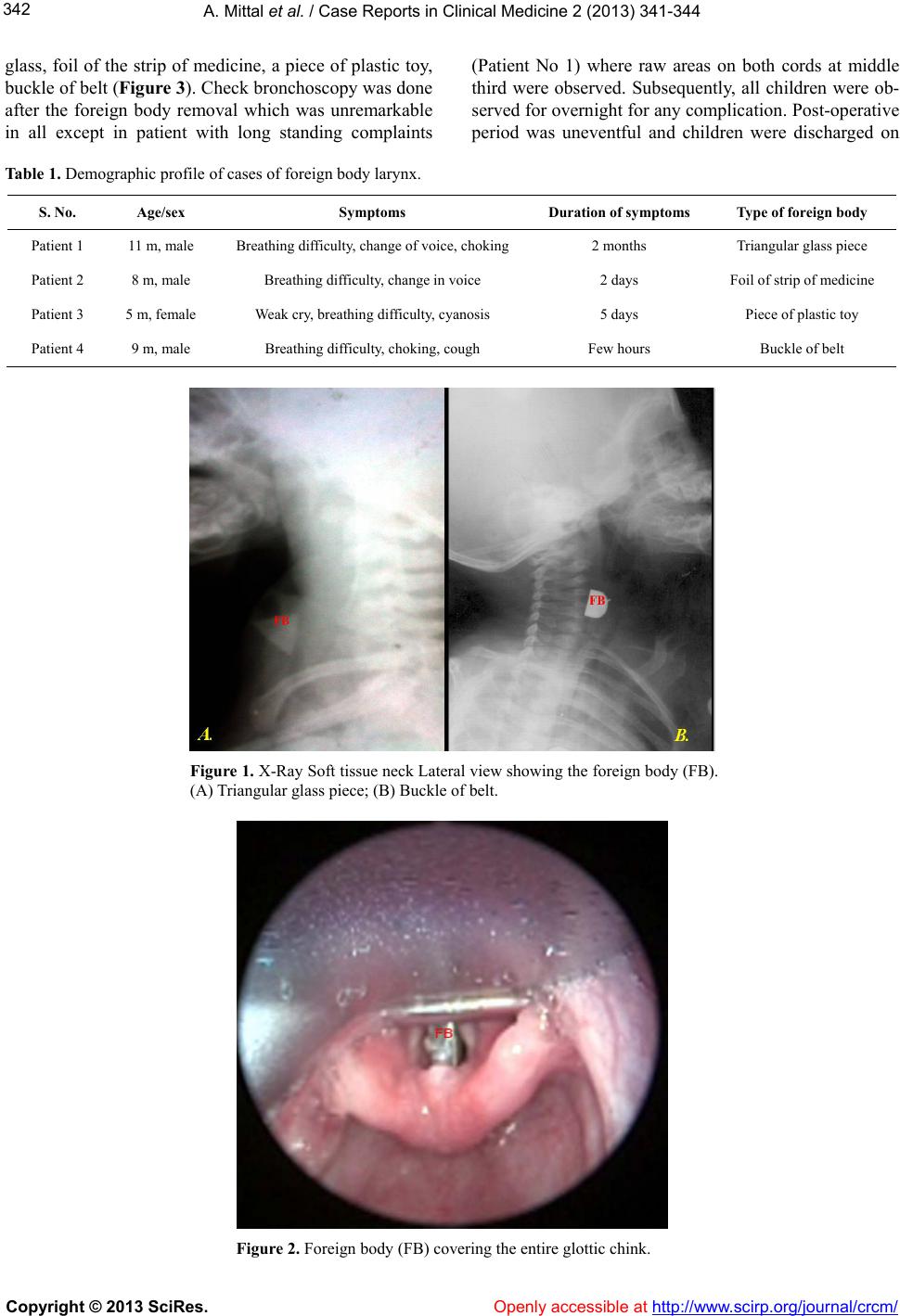
Routine haematological and urine examinations were
normal. X-ray of antero-posterior and lateral view of soft
tissue neck revealed foreign body in the larynx in only
three patients (Figure 1). Considering the possibility for-
eign body these children were subjected to microlaryn-
goscopy/bronchoscopy under general anesthesia on emer-
gency basis.
During the anesthesia, the children were induced using
inhalational sevoflurane only with oral mask. No endo-
tracheal tube was introduced throughout the procedure.
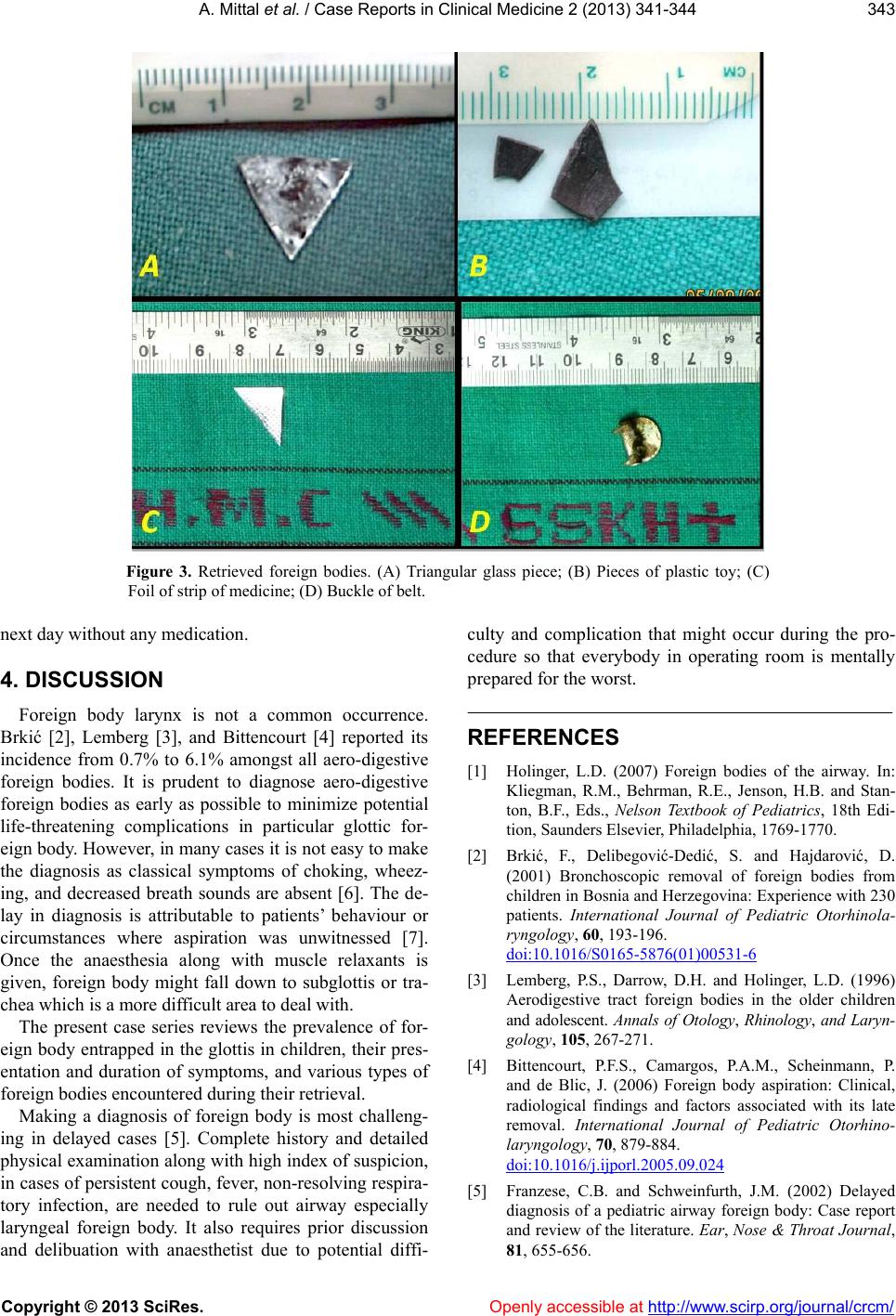
Under deep inhalational anesthesia, direct laryngoscopy
was done with videolaryngoscope and the foreign body
was visualised entrapped in the endolarynx (Figure 2),
which were removed using the appropriate forceps. The
retrieved foreign bodies included a triangular piece of
Copyright © 2013 SciRes. Openly accessible at http://www.sc irp.or g/journal/crcm/