Open Journal of Gastroenterology, 2013, 3, 249-251 OJGas
doi:10.4236/ojgas.2013.34042 Published Online August 2013 (http://www.scirp.org/journal/ojgas/)
Gallbladder carcinoma associated with anomalous union of
pancreatobiliary ductal system*
Sun Young Yi
Division of Gastroenterology, Internal Medicine, School of Medicine, Ewha Womans University, Seoul, South Korea
Email: syy@ewha.ac.kr
Received 11 June 2013; revised 16 July 2013; accepted 28 July 2013
Copyright © 2013 Sun Young Yi. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
A 64-year-old woman was admitted with mild right
upper quadrant abdominal pain. Her physical ex-
amination revealed a moderately nourished female
with normal vital sign and no evidence of jaundice or
anemia. Preoperative diagnosis was choledochal cyst
with anomalous union of pancreaticobiliary duct
(AUPBD), long Y-shaped type and gallbladder (GB)
cancer. An extended cholecystectomy, excision of the
common bile duct and biliary diversion via Roux-en
Y hepaticojejunostomy was performed. The gallblad-
der cancer showed invasion to perimuscular connec-
tive tissue and no extension beyond serosa. Twelve
months after curative resection, the patient had no
evidence of tumor recurrence.
Keywords: Choledochal Cyst; Gallbladder Cancer
1. INTRODUCTION
In anomalous union of pancreaticobiliary duct (AUPBD),
the common chann el is abnormally long and the connec-
tion between the common bile duct and pancreatic duct is
outside of the duodenal wall [1]. Th is congen ital d isord er
is frequently associated with choledochal cystst [1]. More-
over, AUPBD is prone to have benign as well as malign-
nant complications including carcinoma of biliary tract
[2]. I describe here a case of a choledochal cyst com-
bined with Y-shaped AUPBD that was detected in a pa-
tient in her sixties as a primary cancer of the gallbladder.
2. CASE REPORT
A 64-year-old woman was admitted with mild right up-
per quadrant abdominal pain. On abdominal physical
examination, no palpable mass or tenderness was noted.
Laboratory results revealed an elevated serum aspartate
aminotransferase of 472 IU/L, alanine aminotransferase
of 240 IU/L, alkaline phosphatase of 677 IU/L and total
bilirubin of 4.0 mg%. Serum carcinoembryonic antigen
(CEA) was within normal limits and serum carbohydrate
antigen 19-9 (CA19-9) level was slightly elevated (61.3
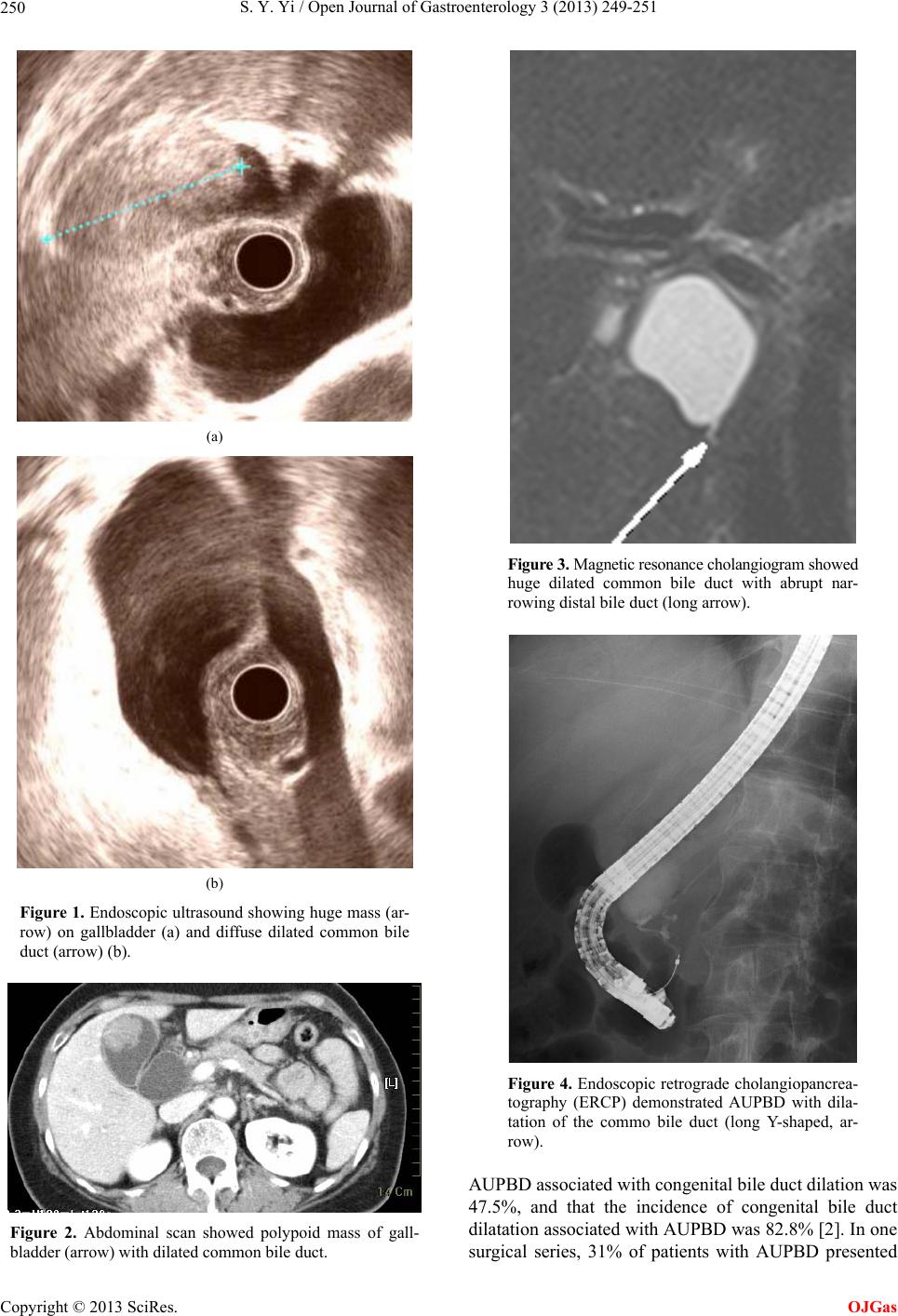
IU/L). Endoscopic ultrasound and abdominal computed
tomography showed moderate dilated gallbladder with
huge mass (38 mm) and marked dilated common bile
duct (CBD) and abruptly narrowed far distal CBD (Fig-
ures 1 and 2). Endoscopic retrograde cholangiopancrea-
tography (ERCP) and magnetic resonance cholangiopan-
creatogram (MRCP) revealed choledochal cyst with ano-
malous union of pancreatobiliary system (Figures 3 and
4). This patient presented with gallbladder mass and
choledochal cyst associated with AUPBD, lon g Y-shaped
type. An extended cholecystectomy, excision of the com-
mon bile duct and biliary d iversion via Roux-en Y heap-
ticojejunostomy was performed. On pathologic evalua-
tion, the CBD was markedly dilated, measuring 3 cm in
inner circumferences and 6 cm in length, and choledo-
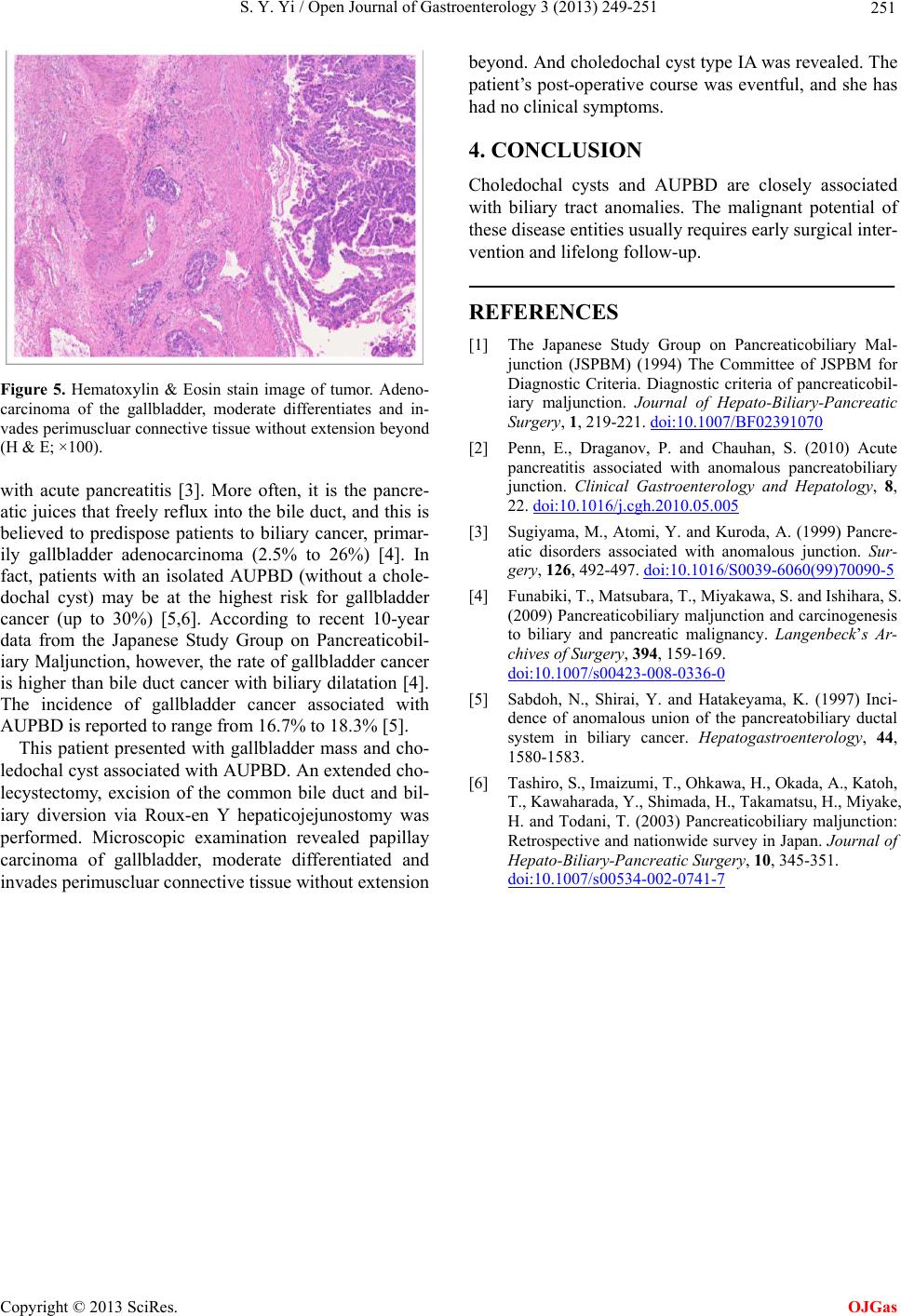
chal cyst type IA was revealed. Microscopic examination
revealed papillay carcinoma of gallbladder, moderately
differentiated and invades peri muscluar connective tissue
without extensio n beyond (Figure 5). The patient’s post-
operative course was eventful, and she has had no clini-
cal symptoms. Twelve months after curative resection,
the patient had no evidence of tumor recurrence.
3. DISCUSSION
AUPBD is a congenital malformation of the pancreato-
biliary tree in which the confluence of the common bile
duct and pancreatic duct is outside the duodenal wall.
The mode of anomalous union is classified into two
types: the pancreatico-choledochal (P-C) type, in which
the main pancreatic duct enters the common bile duct,
and the C-P type, where the CBD enters the main pan-
creatic duct [1]. AUPBD has been regarded to be the
etiologic factor of the choledochal cyst. However, chole-
dochal cyst is not always associated with AUPBD.
*No conflicts of interest exis
.
Published Online August 2013 in SciRes. http://www.scirp.org/journal/ojgas