Open Journal of Ophthalmology, 2013, 3, 73-75
http://dx.doi.org/10.4236/ojoph.2013.33018 Published Online August 2013 (http://www.scirp.org/journal/ojoph) 73
Necrotizing Scleritis Associated with 5-Fluorouracil and
Sub-Tenon’s Block in Patient with Previous
Trabeculectomy: A Case Report
Tuan A. Tran1*, Jeremy O’Connor2, Xavier Fagan3, Tu Tran2, Dan Nguyen2
1Department of Politecnico Ophthalmology, Sydney Eye Hospital , Sydney, Austra lia; 2Department of Glaucoma, Victorian Eye and
Ear Hospital, Melbourne, Australia; 3Department of Medical Ophthalmology, Victorian Eye and Ear Hospital, Melbourne, Australia.
Email: *tuantran86@gmail.com
Received April 24th, 2013; revised May 30th, 2013; accepted June 17th, 2013
Copyright © 2013 Tuan A. Tran et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Necrotizing scleritis is the most severe form of scleritis with a significant threat to vision and globe integrity. It can be
infectious, surgically induced necrotizing scleritis (SINS) or systemic autoimmune associated. We report a case of ne-
crotizing scleritis associated with 5-fluorouracil (5-FU) at the site of sub tenon’s block in a patient with previous trabe-
culectomy. To our knowledge, this is the first reported case of necro tizing scleritis associated with 5-FU. This may im-
plicate alternative approaches to local anaesthetic techniques when using adjunctive 5-FU.
Keywords: Necrotizing Scleritis; 5-Fluorouracil; Sub-Tenon’s Block; Glaucoma
1. Case Report
A 74-year-old man with a 43-year history of primary
open angle glaucoma (POAG) had recent bilateral
trabeculectomies with Mitomycin C (MMC) (0.2 mg/ml
for 3 minutes). Regular reviews demonstrated well func-
tioning blebs and each trabeculectomy was followed up
with three sub-conjunctival 5-FU injections. Medical
history included non-insulin dependent diabetes.
He subsequently developed a right eye cataract and
underwent routine phacoemulsification and intraocular
lens insertion with a temporal clear corn eal wound. Peri-
operative sub-conjunctival 5-FU (5 mg/0.1ml) was in-
jected in the superior fornix above the bleb to minimise
bleb fibrosis. The operation was performed with a sub-
Tenon’s block through an inferonasal conjunctival inci-
sion with 4 ml of lignocaine 2%.
On day one post-operative review, visual acuity with
pinhole (VA-PH) was 6/12 (20/40), intraocular pressure
(IOP) was 12 mmHg and examination was otherwise
unremarkable. He was started on two hourly topical
Prednisolone Acetate 1% and Phenylephrine Hydroch-
loride 0.12% (Prednefrin Forte 1%, Allergan Aust. Pty
Ltd) and four times daily chloramphenicol 0.5%.
On week one post-operative review, significant pain
was noted. Examination revealed VA-PH reduced to 6/18
(20/60), IOP was 14 mmHg. At the site of sub-Tenon’s
block, there was a localised lesion of episcleritis with a
focal area of avascular sclera. No further 5-FU was given
and he was commenced on oral Ibuprofen 400 mg three
times a day.
The following week, VA-PH was 6/12 (20/40), IOP
remained at 14 mmHg and the non-healing conjunctival
defect persisted. There was significant pain preventing
the patient from sleep, which instigated surg ical debride-
ment under peribulbar block. Swabs were taken for
microscopy and culture whilst debrided conjunctival and
Tenon’s tissue were sent for histopathology. Due to a
possible infective cause the conjunctival defect was not
closed.
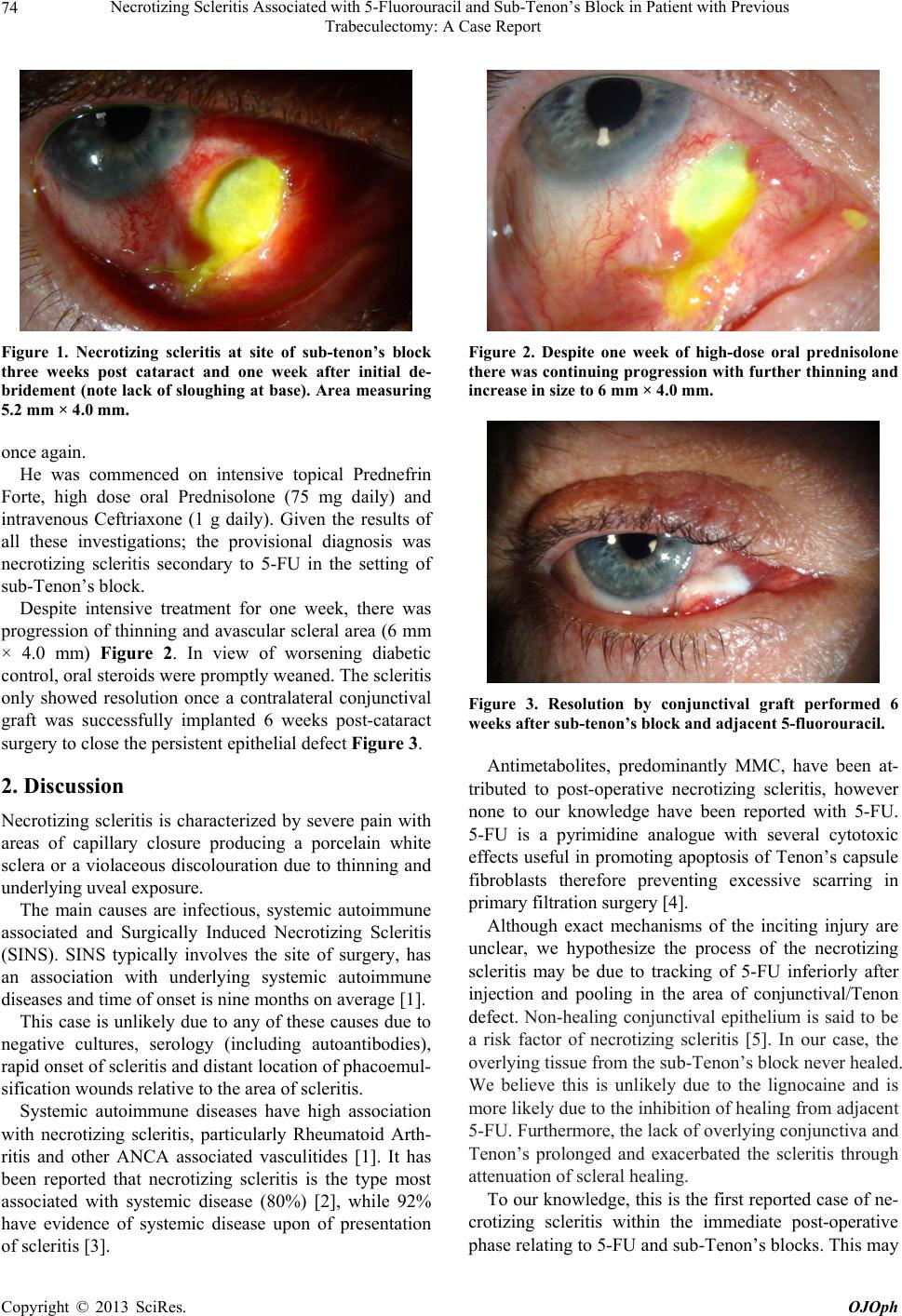
One week post-debridement, pain persisted accompa-
nied with a reduction in VA to 6/36 (20/120) whilst IOP
was 10 mmHg. The area of avascular sclera increased in
size, measuring 5.2 mm × 4.0 mm Figure 1. C ultures
showed no growths while histology demonstrated non-
specific inflammation and no fungal elements.
He was admitted for further investigations and treat-
ment. Vasculitic, autoimmune, treponemal/syphilis and
TB tests were negative. A second debridement was per-
formed. Repeat conjunctival, episcleral and scleral bio-
psies demonstrated unremarkable cultures and histology
*Corresponding a uthor.
Copyright © 2013 SciRes. OJOph