M. E. Asuquo et al. / Case Reports in Clinical Medicine 2 (2013) 2 91-293
Copyright © 2013 SciRes. OPEN ACCESS
293
commonest site of tuberculous lymphadenopathy re-
ported was cervical. Its involvement of cervical lymph
nodes has been known a long time as Scrofula or the
Kings Evil [9]. Olu-Eddo and Omoti reported lympha-
denopathy as the single commonest cause of cervical
lymphadenopathy constituting 35% of cases [4], and in
Saudi Arabia, Al-Sohaibani reported 28% [10]. This com-
munication describes a huge tuberculous lymphadeno-
pathy in an HIV seronegative patient in an uncommon
location for tuberculous cervical lymphadenopathy.
Tuberculous lymphadenopathy is largely confined to
the cervical lymph nodes mostly because tonsils and ade-
noids provide an easy portal of entry for inhaled myco-
bacteria [5]. It may also result from lymphatic or ha-
ematogenous dissemination from an original focus in the
lungs [5], our patient had no identifiable dental or oral
lesion. However, some lesions may be healed without
being detected and may be the case in our patient whose
evaluation revealed no primary focus despite the huge
Submental lymphadenopathy.
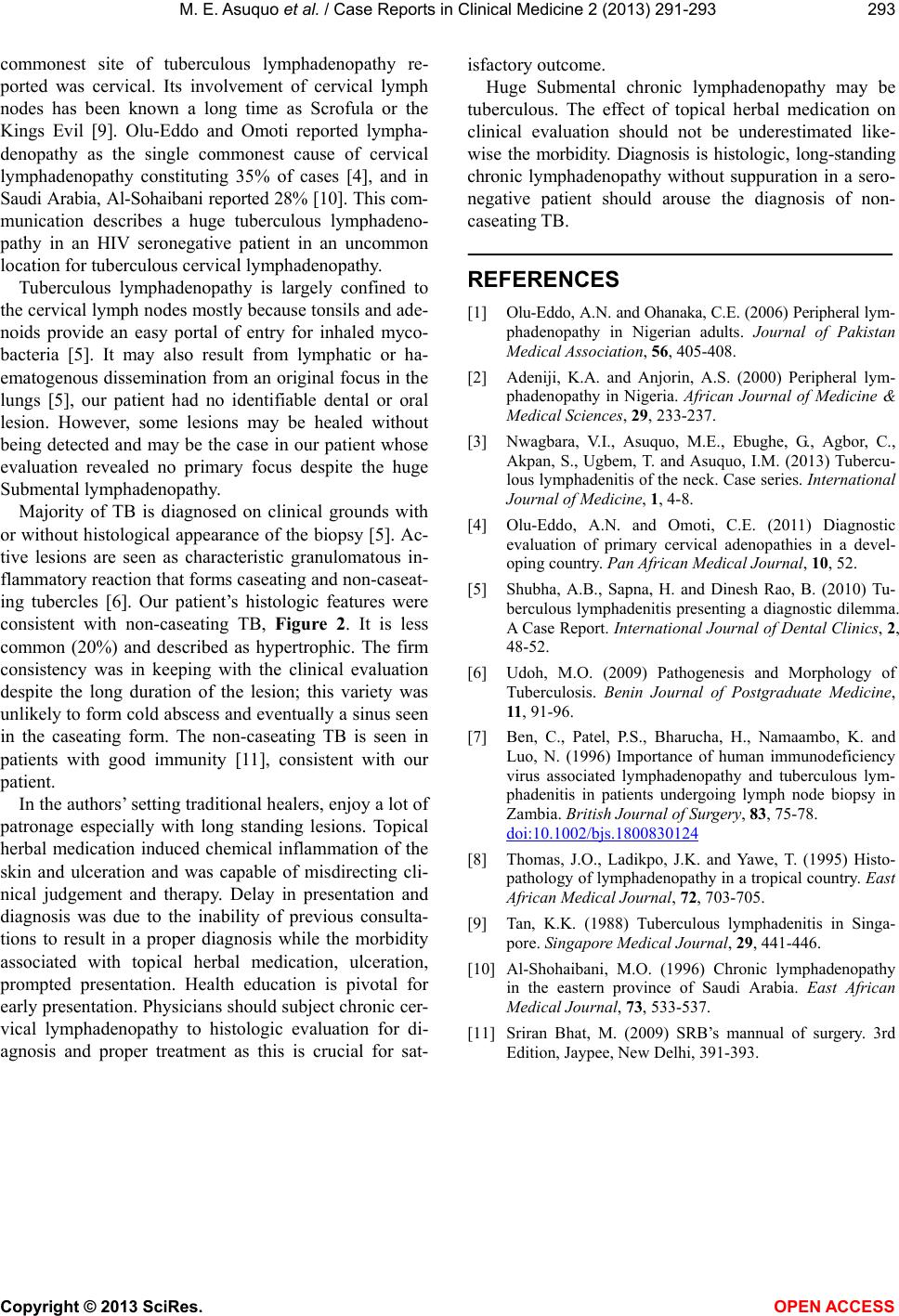
Majority of TB is diagnosed on clinical grounds with
or without histological appearance of the biopsy [5]. Ac-
tive lesions are seen as characteristic granulomatous in-
flammatory reaction that forms caseating and non-caseat-
ing tubercles [6]. Our patient’s histologic features were
consistent with non-caseating TB, Figure 2. It is less
common (20%) and described as hypertrophic. The firm
consistency was in keeping with the clinical evaluation
despite the long duration of the lesion; this variety was
unlikely to form cold ab scess and eventually a sinus seen
in the caseating form. The non-caseating TB is seen in
patients with good immunity [11], consistent with our
patient.
In the authors’ setting tradition al healers, enjo y a lot of
patronage especially with long standing lesions. Topical
herbal medication induced chemical inflammation of the
skin and ulceration and was capable of misdirecting cli-
nical judgement and therapy. Delay in presentation and
diagnosis was due to the inability of previous consulta-
tions to result in a proper diagnosis while the morbidity
associated with topical herbal medication, ulceration,
prompted presentation. Health education is pivotal for
early presentation. Physicians should subject chronic cer-
vical lymphadenopathy to histologic evaluation for di-
agnosis and proper treatment as this is crucial for sat-
isfactory outcome.
Huge Submental chronic lymphadenopathy may be
tuberculous. The effect of topical herbal medication on
clinical evaluation should not be underestimated like-
wise the morbidity. Diagnosis is histologic, long-standing
chronic lymphadenopathy without suppuration in a sero-
negative patient should arouse the diagnosis of non-
caseating TB.
REFERENCES
[1] Olu-Eddo, A.N. and Ohanaka, C.E. (2006) Peripheral ly m-
phadenopathy in Nigerian adults. Journal of Pakistan
Medical Association, 56, 405-408.
[2] Adeniji, K.A. and Anjorin, A.S. (2000) Peripheral lym-
phadenopathy in Nigeria. African Journal of Medicine &
Medical Sciences, 29, 233-237.
[3] Nwagbara, V.I., Asuquo, M.E., Ebughe, G., Agbor, C.,
Akpan, S., Ugbem, T. and Asuquo, I.M. (2013) Tubercu-
lous lymphadenitis of the neck. Case series. International
Journal of Medicine, 1, 4-8.
[4] Olu-Eddo, A.N. and Omoti, C.E. (2011) Diagnostic
evaluation of primary cervical adenopathies in a devel-
oping country. Pan African Medical Journal, 10, 52.
[5] Shubha, A.B., Sapna, H. and Dinesh Rao, B. (2010) Tu-
berculous lymphadenitis presenting a diagnostic dilemma.
A Case Report. International Journal of Dental Clinics, 2,
48-52.
[6] Udoh, M.O. (2009) Pathogenesis and Morphology of
Tuberculosis. Benin Journal of Postgraduate Medicine,
11, 91-96.
[7] Ben, C., Patel, P.S., Bharucha, H., Namaambo, K. and
Luo, N. (1996) Importance of human immunodeficiency
virus associated lymphadenopathy and tuberculous lym-
phadenitis in patients undergoing lymph node biopsy in
Zambia. British Journal of Surgery, 83, 75-78.
doi:10.1002/bjs.1800830124
[8] Thomas, J.O., Ladikpo, J.K. and Yawe, T. (1995) Histo-
pathology of lymphadenopathy in a tropical country. East
African Medical Journal, 72, 703-705.
[9] Tan, K.K. (1988) Tuberculous lymphadenitis in Singa-
pore. Singapore Medical Journal, 29, 441-446.
[10] Al-Shohaibani, M.O. (1996) Chronic lymphadenopathy
in the eastern province of Saudi Arabia. East African
Medical Journal, 73, 533-537.
[11] Sriran Bhat, M. (2009) SRB’s mannual of surgery. 3rd
Edition, Jaypee, New Delhi, 391-393.