A. Y. Taha / Case Reports in Clinical Medicine 2 (2013) 285-290 289
[17]. El-Kushmal et al. achieved 100% success rate with
FOB, moreover, rigid videobronchoscopy was used by
the same authors from Jordan in a group of 28 patients
and could achieve a 100% success as well [16].
Looking at the Turkish experience with headscarf pin
aspiration, we find that a 100% su ccess was achieved by
Gencer M. et al. [13] while it was much lower in the
other 2 studies (25% [14] and 3.2% [15]). The RB, on
the other hand was more frequently used and more suc-
cessful in the latter 2 studies (99% [14] and 90% [15]).
These differences may be related to different training an d
skills of the authors. Surgery was the last resort and very
occasionally needed in the reviewed studies, a finding
similar to ours [14,15,17].
The experience in the west highly supports the utility
and safety of FOB for removal of bronchial FBs [5,10,
11]. Both Swanson K.L. et al. and Boyd M. et al.; Ame-
rican authors, conclude that FOB is effective both in the
diagnosis & treatment of FBs [5,10]. The study from
Mexico is even more interesting. Fifty n ine ch ild ren ag ed
9 months to 16 years with different bronchial FBs were
all bronchoscoped using FOB to remove FBs. It was suc-
cessful in 91.3% of patients. The authors thus conclude
that FOB must be taken into account as an initial thera-
peutic method for FB removal in infants and chil dren [11].
The other reviewed studies from Asia and Europe re-
port excellent results with FOB and bronch ial FBs [1,6 ,7 ,
12,19]. Chin-Wing Y.U. from Honk Kong states that
most FBs in adults can be removed with FOB; RB is
occasionally needed [1].
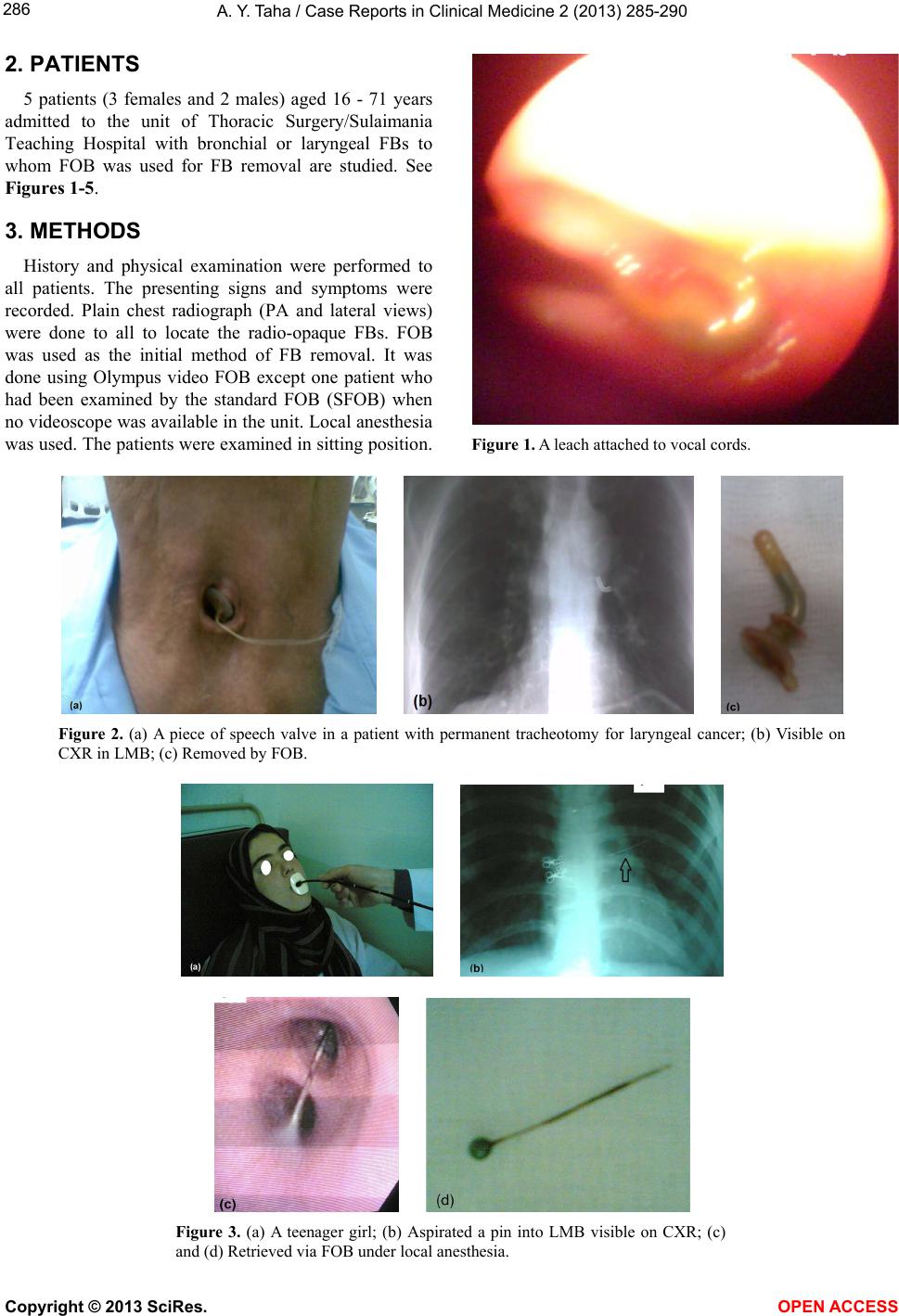
The second patient in this study was a man of 71 with
total laryngectomy and permanent tracheotomy done for
cancer of the larynx 10 years earlier. He had presented
with an aspirated piece of speech valve. This FB was re-
moved successfully by FOB through the tracheotomy
stoma. The literature confirms the difficulties encoun-
tered in the fixation of prostheses for voice rehabilitation
after laryngectomy [20].
6. CONCLUSION
Though RB is a time tested safe and effective proce-
dure for FB removal which is in use all over the world;
FOB can also be used safely provided the operator has
adequate skill in RB, the latter should be readily avail-
able in case a difficulty is encountered with FOB. It is
especially helpful when an adult patient has a doubtful
diagnosis of FB aspiration and the risk of GA necessary
for RB is to be avoided. To increase its success rate,
FOB use should be coupled with the necessary equip-
ments like special FB forceps and fluoroscopy.
REFERENCES
[1] Chin-Wing, Y.U. (2012) Rigid bronchoscopy—A physic-
cian’s perspective. Hong Kong Respiratory Medicine. The
official website of HKTS, ACCP HK & Macau, HKLF.
[2] Elhassani, N.B. (1978) Aspirated tracheobronchial for-
eign bodies in infants. Annals of the Royal College of
Surgeons of England, 23, 310-314.
[3] Hussein. W.M. (1984) Tracheobronchial foreign bodies in
pediatric age group. Journal of the Faculty of Medicine,
Baghdad, 26, 63-72.
[4] Abdulameer, M.H. (2010) Foreign bodies inhalation. Jour-
nal of the Faculty of Medicine, Baghdad, 52, 255-258.
[5] Swanson, K.L. and Edell, E.S. (2001) Tracheobronchial
foreign bodies. Chest Surgery Clinics of North America,
11, 861-872.
[6] Lan, R.S., Lee, Ch., Chiang, Y.C. and Wang, W.J. (1989)
Use of fiberoptic bronchoscopy to retrieve bronchial for-
eign bodies in adults. American Review of Respiratory
Disease, 140, 1734-1737. doi:10.1164/ajrccm/140.6.1734
[7] Donado Una, J.R., de Miguel Poch, E., Casado Lopez,
M.E. and Alfaro Abreu, J.J. (1998) Fiberoptic broncho-
scopy in extraction of tracheobronchial foreign bodies in
adults. Arch Bronchopneumo l, 34, 76-81.
[8] Muhammad, T.D., Saad, M.M., Bahaa, M.A. and Omer,
R.H. (2010) Tracheo-bronchial foreign bodies inhalation
in Al-Anbar Governorate. Kufa Medical Journal, 13, 248-
262.
[9] Akhtar, S. and Ul Hak, I. (2006) An experience with
leeches in the aero-digestive tract.
http://www.pafmj.org/showdetails.php?id=60&t=c
[10] Boyd, M., Chatterjee, A., Chiles, C. and Chin Jr., R.
(2009) Tracheobronchial foreign body aspiration in adults.
Southern Medical Journal, 102, 171-174.
doi:10.1097/SMJ.0b013e318193c9c8
[11] Ramirez-Figueroa, J.L., Gochicoa-Rangel, L.G, Ramirez-
San Juan, D.H. and Vargas, M.H. (2005) Foreign body
removal by flexible fiberoptic bronchoscopy in infants
and children. Pediatric Pulmonology, 40, 392-397.
doi:10.1002/ppul.20242
[12] Mise, K., Jurcev Savicevic, A., Pavlov, N. and Jankovic,
N. (2009) Removal of tracheobronchial foreign bodies in
adults using flexible bronchoscopy: Experience 1995-
2006. Surgical Endoscopy, 23, 1360-1364.
doi:10.1007/s00464-008-0181-9
[13] Gencer, M., Ceylan, E. and koksal, N. (2007) Extraction
of pins from the airway with flexible bronchoscopy. Res-
piration, 74, 674-679.
[14] Hasdiraz, L., Bicer, C., Bilgin, M. and Oguzkaya, F. (2006)
Turban pin aspiration: Non-asphyxiating tracheobronchial
foreign body in young Islamic women. Thoracic and
Cardiovascular Surgeon, 54, 273-275.
doi:10.1055/s-2006-923954
[15] Kaptanoglu, M., Dogan, K., Onen, A. and Kunt, N. (1999)
Turban pin aspiration; a potential risk for young Islamic
girls. International Journal of Pediatric Otorhinolaryn-
gology, 48, 131-135.
[16] El-Kushman, H.M., Sharara, A.M., Sa Ada, M.A. and
Hijazi, Ma. (2007) Tracheobronchial straight metallic pin
aspiration in young Jordanian females. Saudi Medical
Journal, 28, 913-916.
Copyright © 2013 SciRes. OPEN ACCESS