K. Koneri et al. / Open Journal of Gastroenterology 3 (2013) 227-230
Copyright © 2013 SciRes.
230
[3] Bioulac-Sage, P., Balabaud, C. and Wanless, I. (2000)
Focal nodular hyperplasia and hepatocellular adenoma. In:
Bosman, F., Ed., WHO classification of tumours of the
digestive system. 4th Edition, IARC, Lyon, 198-204.
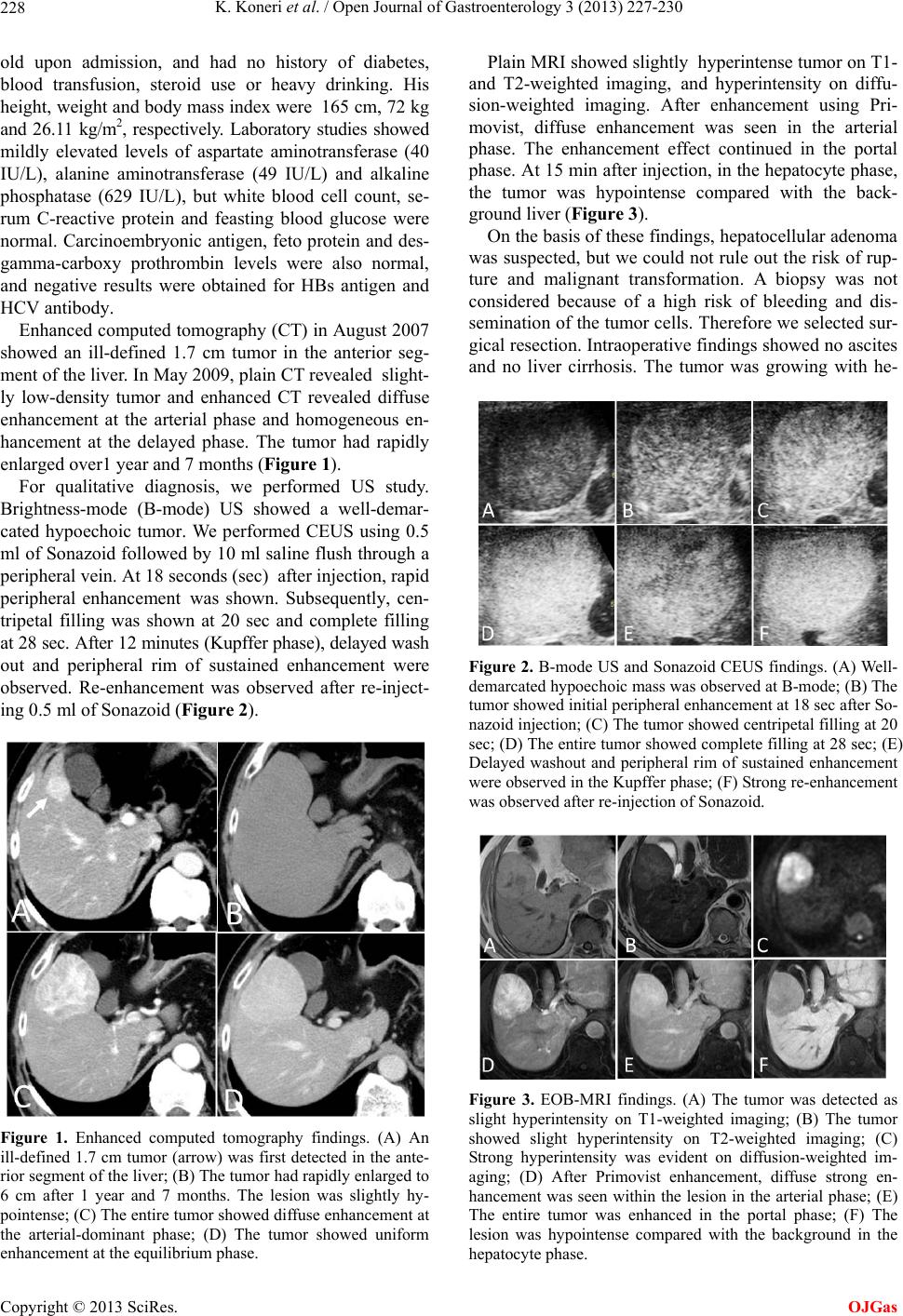
increased expression of inflammatory proteins (SAA and
CRP) is detected in tumor hepatocytes. Our case showed
a typical pattern, both histologically and immunohistolo-
gically. [4] Rebouissou, S., Amessou, M., Couchy, G., Poussin, K.,
Imbeaud, S., Pilati, C., Izard, T., Balabaud, C., Bioulac-
Sage, P. and Zucman-Rossi, J. (2009) Frequent in-frame
somatic deletions activate gp130 in inflammatory heap-
tocellular tumours. Nature, 457, 200-204.
doi:10.1038/nature07475
A molecular gain-of-function mutation in the IL-6
pathway results in marked inflammation in IHCA. In a
recent report, a gain-of-function mutation in glycoprotein
130, a co-receptor for the IL-6 receptor, was reported in
60% of IHCAs [4]. A gain-of-function mutation in STAT-
3, downstream in the IL-6 pathway, also occurs in 8% of
IHCAs [9]. These mutations play an important role in the
pathogenesis of IHCA. In this regard, attention should be
paid to the findings of further research.
[5] Sasaki, M., Yoneda, N., Kitamura, S., Sato, Y. and Na-
kanuma, Y. (2011) Characterization of hepatocellular ade-
noma based on the phenotypic classification: The Kana-
zawa experience. Hepatology Research, 41, 982-988.
doi:10.1111/j.1872-034X.2011.00851.x
Regarding the malignant potential of IHCA, Dokmak
et al. reported on 122 HCA patients, finding IHCA in 66
patients and malignant transformation in 7 cases (10.6%)
[10]. They also mentioned that maleness was a risk factor
of malignant transformation, and ≥5 cm in diameter was
associated with a higher risk of intratumoral hemorrhage
[10].We consider that rapid enlargement in our case can
be attributed to the intratumoral hemorrhage without trans-
forming to the malignancy.
[6] Paradis, V., Champault, A., Ronot, M., Deschamps, L.,
Valla, D.C., Vidaud, D., Vilgrain, V., Belghiti, J. and
Bedossa, P. (2007) Telangiectatic adenoma: An entity as-
sociated with invreased body mass index and inflamma-
tion. Hepatology, 46, 140-146. doi:10.1002/hep.21684
[7] Katabathina, V.S., Menias, C.O., Shanbhogue, A.K.P.,
Fagirdar, F., Paspulati, R.M. and Prasad, S.R. (2011) Ge-
netics and imaging of hepatocellular adenomas: 2011
update. AbdGast Imaging, 31, 1529-1543.
As another option for treatment, hepatic arterial chemo-
embolization has also been reported [11]. However, tu-
mor behavior has not been completely elucidated, and so
have the concerns about malignant transformation. More-
nover, the tumor ruptured cannot be dispelled. We think
surgical resection is the most adequate treatment at the
present.
[8] Laumonier, H., Cailliez, H., Balabaud, C., Possenti, L.,
Zucman-Rossi, J., Bioulac-Sage, P. and Trillaud, H. (2012)
Role of contrast-enhanced sonography in differentiation
of subtypes of hepatocellular adenoma: Correlation with
MRI findings. American Journal of Roentgenology, 199,
341-348. doi:10.2214/AJR.11.7046
[9] Pliati, C., Amessou, M., Bihl, M.P., Balabaud, C., Nhieu,
J.T., Paradis, V., Nault, J.C., Izard, T., Bioulac-Sage, P.,
Couchy, G., et al. (2011) Somatic mutations activating
STAT3 in human inflammatory hepatocellular adenomas.
Journal of Experimental Medicine, 208, 1359-1366.
doi:10.1084/jem.20110283
REFERENCES
[1] Bioulac-Sage, P., Rebouissou, S., Thomas, C., Blanc, J.F.,
Saric, J., Cunha, A.S., Rullier, A., Cubel, G., Couchy, G.,
Imbeaud, S., et al. (2007) Hepatocellular adenoma sub-
type classification using molecular markers and immuno-
histochemistry. Hepatology, 46, 740-748.
doi:10.1002/hep.21743
[10] Dokmak, S., Paradis, V., Vilgrain, V., Sauvanet, A., Far-
ges, O., Valla, D., Bedossa, P. and Belghiti, J. (2009) A
single-center surgical experience of 122 patients with
single and multiple hepatocellular adenomas. Gastroen-
terology, 137, 1698-1705.
doi:10.1053/j.gastro.2009.07.061
[2] Zucman-Rossi, J., Jeannot, E., Nhieu, J.T., Scoazec, J.Y.,
Guettier, C., Rebouissou, S., Bacq, Y., Leteurtre, E., Pa-
radis, V., Michalak, S., et al. (2006) Genotype-phenotype
correlation in hepatocellular adenoma: New classification
and relationship with HCC. Hepatology, 43, 515-524.
doi:10.1002/hep.21068
[11] Stoot, J.K., van de Linden, E., Terpstra, O.T. and Scha-
apherder, A.F. (2007) Life-saving therapy for haemor-
rhaging liver adenomas using selective arterial emboliza-
tion. British Journal of Surgery, 94, 1249-1253.
doi:10.1002/bjs.5779
OJGas