 Open Journal of Depression 2013. Vol.2, No.3, 24-31 Published Online August 2013 in SciRes (http://www.scirp.org/journal/ojd) http://dx.doi.org/10.4236/ojd.2013.23006 Copyright © 2013 SciRes. 24 The Relationship between Prenatal Stress, Depression, Cortisol and Preterm Birth: A Review Kiran Shaikh1*, Shahirose Premj i2, Khurshid Khowaja3, Suzanne Tough4, Ambreen Kazi5, Shaneela Khowaja6 1Aga Khan University School of Nu rsing and Midwifery, Karachi, Pakistan 2University of Calgary, Alberta, Canada 3Director of Nursing Al Noor Hospital, Al Ain and Associate Professor, Aga Khan University, Karachi, Pakistan 4Department of Pediatrics an d C ommunity Health, University of Calgary, Alberta, Canada 5Department of Community Health Sciences, Aga Khan University, Karachi, Pakistan 6Aga Khan University School of Nu rsing and Midwifery, Karachi, Pakistan Email: *kiran.shaikh@aku.edu Received May 20th, 2013; revised June 22nd, 2013; accepted July 3rd, 2013 Copyright © 2013 Kiran Shaikh et al. This is an open access article distributed under the Creative Commons At- tribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Preterm birth is one of the most common adverse pregnancy outcomes. Maternal risk factors such as stress and depression have been associated with preterm birth. Preterm infants are at a higher risk of poor growth and neuro developmental outcomes. The objective of this paper is to examine the relationship be- tween maternal stress, depression, cortisol level, and preterm birth. Preterm birth is one of the most com- mon adverse pregnancy outcomes with a global prevalence of 9.6% and one of the major contributors to infant mortality and morbidity. The association between psychosocial stress and preterm birth, although examined for more than 25 years, has not yet been fully established. A systemic review was conducted in which research studies and review articles from 1970 to 2012, published in English, focusing on human subjects, and addressing the relationship between stress, depression, cortisol and preterm birth were in- cluded in this review. The studies examining the relationship between stress, cortisol levels and preterm birth have shown inconsis tent findings that may be explained by varied study designs, differences in defin- ing and measuring stress, timing of stress measurement, sample characteristics, and study designs. The relationship between stress, cortisol levels and preterm birth may be multifactorial and complex with premature birth being the final common pathway. A longitudinal cohort study, with a large sample size and multiple measures of stress, depression, and cortisol level, as well as a measure of anxiety and other stress hormone biomarkers may add new knowledge and enhance our understanding about the contribu- tion of psychosocial stress to preterm birth. Keywords: Maternal Stress; Antenatal Stress; Maternal Depression; Preterm Delivery; Preterm Birth; Gestational Age; Low Birth Weights; Cortisol Introduction Preterm birth, defined as “birth before 37 completed weeks” (Steer, 2005: p. 1), is one of the most common adverse preg- nancy outcomes. Preterm birth is a global issue, irrespective of region or the level of resources (Beck et al., 2010). All resource regions: high, middle, and low report varying degrees of pre- term birth rates (Beck et al.). The rate of preterm delivery ranges from 5% in developed countries to 25% in developing countries (Goldenberg et al., 2008; Steer, 2005). Africa (11.9%), followed by North America (10.6%) and Asia (9.1%) have the highest rates of preterm birth. The estimated global rate of pre- term birth is 9.6% which is close to the rate of preterm birth rate in Asia (Beck et al.). Studies indicate that preterm birth has an impact on the rate of infant mortality and morbidity (Ma- thew & Mac Dorman, 2007). According to the World Bank (2008), the global infant mortality rate was 46 per 1000 live births. Prematurity and its complications account for almost 30 percent of neonatal deaths (Mathews & Mac Dorman). The cost of the hospitalization of preterm birth infant is $5.8 billion rep- resenting half of infant hospitalization cost (Russell et al., 2007). Moreover, stress of hospitalization and fear of losing an infant is trauma tic and a source of grief for the family. Beside s this, the psychological distress and risk of postpartum depres- sion increases with having a preterm baby (Hill & Aldag, 2007). Preterm infants are also at a greater risk of serious health prob- lems, such as cerebral palsy, blindness, breathing problems, and cognitive learning disabilities (Green et al., 2005; Latengresse, 2009; Rafati et al., 2005). Kramer et al. (2009) stated that un- derstanding the etiology of preterm birth will facilitate early identification of mothers at risk for preterm birth. Imple- mentation of early intervention strategies for these high risk mothers will decrease preterm birth thereby reducing the burden of preterm birth (i.e., infant mortality, morbidity, postpartum depression, parental role stress, and financial *Corresponding author. 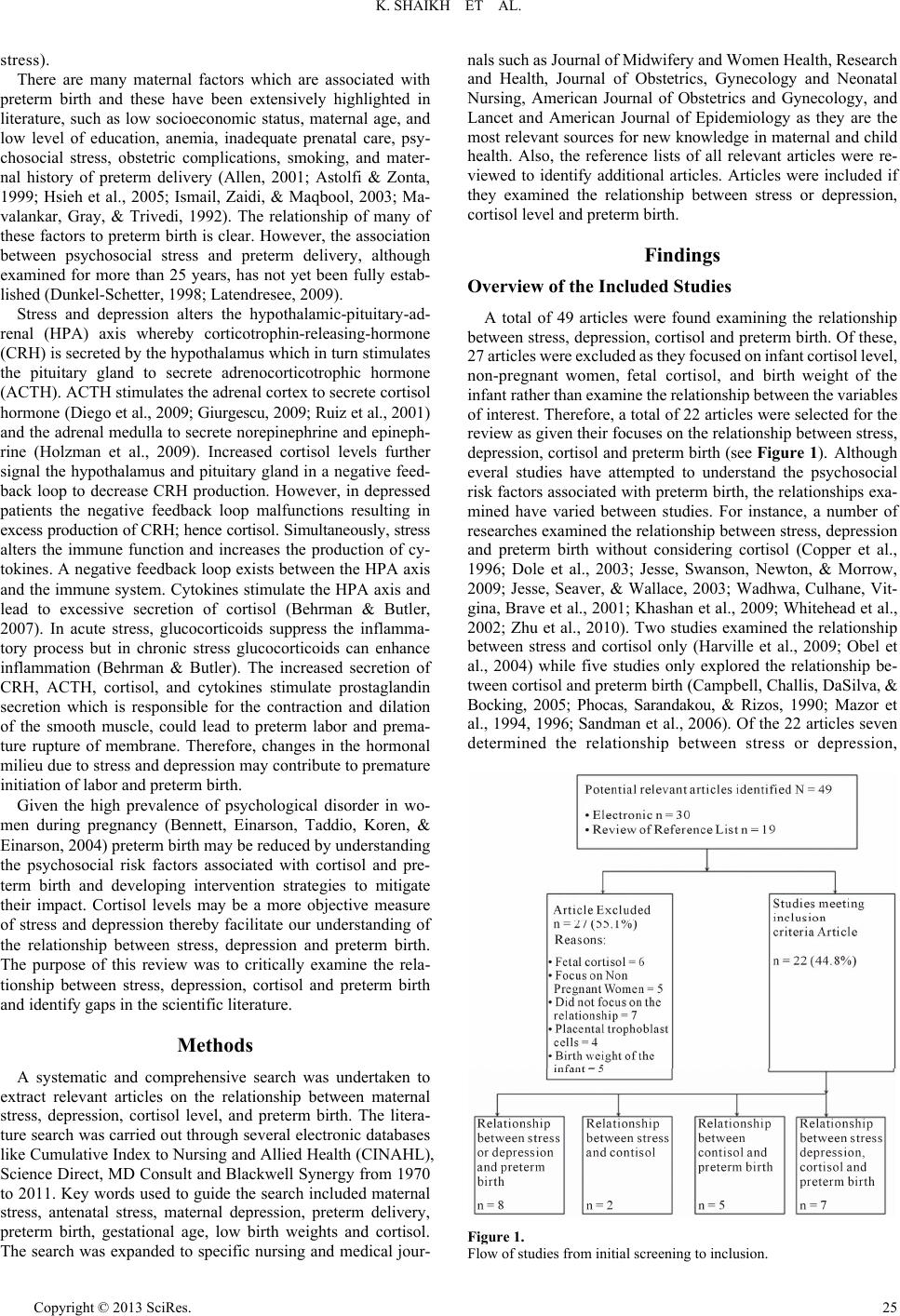 K. SHAIKH ET AL. stress). There are many maternal factors which are associated with preterm birth and these have been extensively highlighted in literature, such as low socioeconomic status, maternal age, and low level of education, anemia, inadequate prenatal care, psy- chosocial stress, obstetric complications, smoking, and mater- nal history of preterm delivery (Allen, 2001; Astolfi & Zonta, 1999; Hsieh et al., 2005; Ismail, Zaidi, & Maqbool, 2003; Ma- valankar, Gray, & Trivedi, 1992). The relationship of many of these factors to preterm birth is clear. However, the association between psychosocial stress and preterm delivery, although examined for more than 25 years, has not yet been fully estab- lished (Dunkel-Schetter, 1998; Latendresee, 2009). Stress and depression alters the hypothalamic-pituitary-ad- renal (HPA) axis whereby corticotrophin-releasing-hormone (CRH) is secreted by the hypothalamus which in turn stimulates the pituitary gland to secrete adrenocorticotrophic hormone (ACTH). ACTH stimulates the adrenal cortex to secrete cortisol hor mo ne ( Di eg o et al., 2009; Giurgescu, 2009; Ruiz et al., 2001) and the adrenal medulla to secrete norepinephrine and epineph- rine (Holzman et al., 2009). Increased cortisol levels further signal the hypothalamus and pituitary gland in a negative feed- back loop to decrease CRH production. However, in depressed patients the negative feedback loop malfunctions resulting in excess production of CRH; he nce cortisol. Simultaneously , stress alters the immune function and increases the production of cy- tokines. A negative feedback loop exists between the HPA axis and the immune system. Cytokines stimulate the HPA axis and lead to excessive secretion of cortisol (Behrman & Butler, 2007). In acute stress, glucocorticoids suppress the inflamma- tory process but in chronic stress glucocorticoids can enhance inflammation (Behrman & Butler). The increased secretion of CRH, ACTH, cortisol, and cytokines stimulate prostaglandin secretion which is responsible for the contraction and dilation of the smooth muscle, could lead to preterm labor and prema- ture rupture of membrane. Therefore, changes in the hormonal milieu due to stress and depression may contribute to premature initiation of labor and preterm birth. Given the high prevalence of psychological disorder in wo- men during pregnancy (Bennett, Einarson, Taddio, Koren, & Einarson, 2004) preterm birth may be reduced by understanding the psychosocial risk factors associated with cortisol and pre- term birth and developing intervention strategies to mitigate their impact. Cortisol levels may be a more objective measure of stress and depression thereby facilitate our understanding of the relationship between stress, depression and preterm birth. The purpose of this review was to critically examine the rela- tionship between stress, depression, cortisol and preterm birth and identify gaps in the scientific literature. Methods A systematic and comprehensive search was undertaken to extract relevant articles on the relationship between maternal stress, depression, cortisol level, and preterm birth. The litera- ture search was carried out through several electronic databases like Cumulative Index to Nursing and Allied Health (CINAHL), Science Direct, MD Consult and Blackwell Synergy from 1970 to 2011. Key words used to guide the search included maternal stress, antenatal stress, maternal depression, preterm delivery, preterm birth, gestational age, low birth weights and cortisol. The search was expanded to specific nursing and medical jour- nals such as J ourna l of M idwifery and Wom en He alth , Rese arch and Health, Journal of Obstetrics, Gynecology and Neonatal Nursing, American Journal of Obstetrics and Gynecology, and Lancet and American Journal of Epidemiology as they are the most relevant sources for new knowledge in maternal and child health. Also, the reference lists of all relevant articles were re- viewed to identify additional articles. Articles were included if they examined the relationship between stress or depression, cortisol level and preterm birth. Findings Overview of the Included Studies A total of 49 articles were found examining the relationship between stress, depression, cortisol and preterm birth. Of these, 27 articles wer e excluded as the y focused on infant cor tisol level, non-pregnant women, fetal cortisol, and birth weight of the infant rather than examine the r elationship betwee n the variables of interest. Therefore, a total of 22 articles were selected for the review as given their focuses on the relationship between stress, depression, cortisol and preterm birth (see Figure 1). Although everal studies have attempted to understand the psychosocial risk factors associated with preterm birth, the relationships exa- mined have varied between studies. For instance, a number of researches examined the relationship between stress, depression and preterm birth without considering cortisol (Copper et al., 1996; Dole et al., 2003; Jesse, Swanson, Newton, & Morrow, 2009; Jesse, Seaver, & Wallace, 2003; Wadhwa, Culhane, Vit- gina, Brave et al., 2001; Khashan et al., 2009; Whitehead et al., 2002; Zhu et al., 2010). Two studies examined the relationship between stress and cortisol only (Harville et al., 2009; Obel et al., 2004) while five studies only explored the relationship be- tween cortisol and preterm birth (Campbell, Challis, DaSilva, & Bocking, 2005; Phocas, Sarandakou, & Rizos, 1990; Mazor et al., 1994, 1996; Sandman et al., 2006). Of the 22 articles seven determined the relationship between stress or depression, Figure 1. Flow of studies from initial screening to inclusion. Copyright © 2013 SciRes. 25  K. SHAIKH ET AL. cortisol and preterm birth together at the same time (Diego et al., 2009; Erickson et al., 2001; Field et al., 2004, 2006; Hobel et al., 1999; Kramer et al., 2009; Shaikh et al., 2011). Relationsh i p be tw e en Prenatal Stress or D epres sion and Preterm Birth Many studies demonstrate an association between stress and preterm birth (Copper et al., 1996; Erickson et al., 2001; Hobel et al., 1999; Jesse et al., 2009; Ruiz et al., 2001). Copper et al., in a prospective study, enrolled 2593 pregnant women between 25 to 29 weeks of gestation and demonstrated that stress was significantly associated with sp ontaneous preterm birth and low birth weight. Similarly, Jesse et al. (2003) conducted a prospec- tive correlation research design in which 120 Appalachian pregnant women were recruited between 16 and 28 weeks of gestation and showed that symptoms of depression, level of self esteem, and perception towards pregnancy were significantly associated with preterm delivery. Women with depressive sy mp- toms were four times more likely to deliver preterm birth as compared to women without depressive symptoms. In this stu- dy the rate of preterm delivery was 27 out of 120 babies (i.e., 23% delivered preterm). Also, a population based retrospective cohort study conducted in Denmark between January 1979 and December, 2002, reported that maternal exposure to severe life events increased the risk of preterm delivery (Khashan et al., 2009). Whitehead, Hill, Brogan, and Blackmore-Prince (2002) explored that stress beyond a certain threshold affects the rela- tionship between stress and preterm birth. On the other hand, many studies have reported contradictory findings. Jesse et al. (2009) studied the relationship between bi- opsychosocial factors and preterm birth in different ethnic groups. Preterm delivery was three times higher in African American than Hispanic and Caucasian women, but there was no significant relationship between depressive symptoms and preterm birth in African American or Caucasian women. Many other studies have emphasized racial disparity as one of the causes of preterm birth and highlighted that preterm birth was more evident in African-American women compared to non- Hispanic white women (Kramer & Hogue, 2009; Pearl, Brave- man, & Abrams, 2001). Wadhwa et al. (1993) also used a prospective study and re- cruited 90 women at 22 and 28 weeks of pregnancy and showed no significant relationship between perceived stress and gesta- tional age at birth. In addition, Dole et al. (2003) reported simi- lar findings in which life events, social support and depression were not significantly associated with preterm birth. Similarly, Hedegaard, Henriksen, Secher, Hatch and Sabroe (1996) in a population based study of 5873 pregnant women reported that negatives life events during pregnancy did not increase the risk of preterm birth. Relationship between Stress and Cortisol Harville et al. (2009) analyzed data of stress and cortisol from 1587 North Carolina and collected one saliva sample for cortisol measurement and blood for CRH at 14 - 19 and 24 - 29 weeks’ gestation and found no co-relation between self-report- ed indicators of stress and hormones such as cortisol and corti- cotrophin-releasing hormone. While Obel et al. (2005) examin- ed the exposure to stressful life events and changes in levels of cortisol during pregnancy in a population of 603 pregnant wo- men and found evening cortisol to be more strongly associated with stress markers than morning cortisol. Relationship between Cortisol and Preterm Birth High cortisol level in pregnancy has been associated with adverse pregnancy outcomes like aborted fetus, delayed fetal growth, preterm delivery, and low birth weight baby (Campbell, Challis, DaSilva, & Bocking, 2005; Field, Diego, Hernandez- Reif, et al., 2008). A systematic review has been done to deter- mine the relationship between cortisol levels and preterm birth (Giurgescu, 2009). For this review, fifteen studies were selected. Out of these, some studies determine the relationship of cortisol and preterm birth and the remaining studies determine the rela- tionship of maternal stress, depression, anxiety, cortisol, and preterm delivery. The majority of these studies suggested that women with higher cortisol levels in pregnancy were at greater risk of preterm birth. Phocas et al. (1990) measured maternal cortisol levels in 204 pregnant women at different gestational ages. The blood cortisol samples were obtained between 8:00 a.m. to 9:00 a.m. Cortisol gradually increased from 6 weeks to 40 weeks of pregnancy and a sharp rise was noted two weeks before the onset of labor in normal pregnancy. Mazor et al. (1994) measured the amniotic fluid and plasma concentrations of cortisol in 38 women with preterm labor and intact membrane between 32 and 36 weeks of gestation. Ma- ternal plasma cortisol levels were significantly higher in women with preterm births than in those who delivered at term, but no significant differences were reported in amniotic fluid cortisol concentration. Similar results were found in a study where plas- ma and amniotic fluid cortisol were measured for 40 pregnant women with preterm labor and intact membrane at 28 to 30 weeks of gestation (Mazor et al., 1996). Sandman et al. (2006) studied the relationship between ma- ternal cortisol and CRH in 203 pregnant women in a longitudi- nal study. Cortisol at 15 weeks of gestation predicted elevated CRH at 31 weeks. A few studies measured the blood cortisol level in pregnant women admitted with a diagnosis of threat- ened preterm labor (Campbell et al., 2005). Cortisol was sig- nificantly higher in women who gave birth within 24 to 48 hours of hospitalization. A majority of results of these studies lend support to the premise that high blood level of cortisol in- creases the risk of preterm delivery. Relationship between Stress or Depression, Cortisol and Preterm Birth The studies that examine the relationship between maternal stress, cortisol and preterm birth together at the same time have inconsistent findings (see Table 1) (Erickson et al., 2001; Ho- bel et al., 1999; Kramer et al., 2009; Ruiz et al., 2001; Shaikh et al., 2011). Few studies (Erickson et al., 2001; Hobel et al., 1999; Kramer et al., 2009) support the hypothesis that cortisol levels increase with maternal stress. However, the Ruiz et al. (2001) study does not support the hypothesis that cortisol levels in- creases with stress, but it shows a significant relationship be- tween stress and gestational age. Moreover, Shaikh et al. (2011) did not find any relationship between stress, cortisol and pre- term birth. Erickson et al. (2001) prospectively recruited 3596 women and matched 59 women who delivered preterm with 300 wo- men who delivered at term. Hobel (1999) also conducted a pro- spective study in which 524 women of diverse ethnic and Copyright © 2013 SciRes. 26 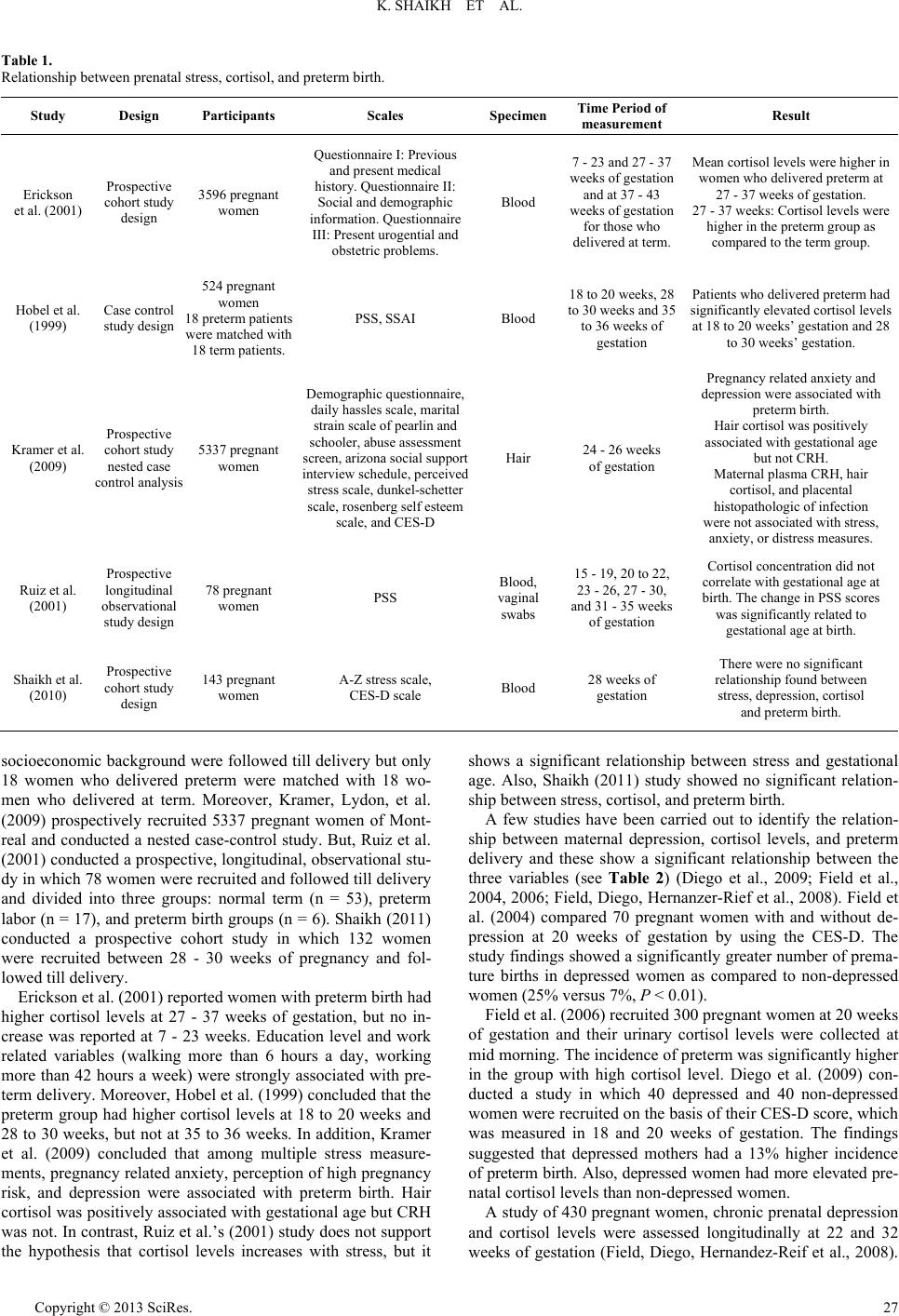 K. SHAIKH ET AL. Copyright © 2013 SciRes. 27 Table 1. Relationship between prenatal stress, cortisol, and preterm birth. Study Design Participants Scales SpecimenTime Period of measurement Result Erickson et al. (2001) Prospective cohort study design 3596 pregnant women Questionnaire I : Previous and present medical history. Que stionnaire II: Social and demographic information. Q u estionnaire III: Present u r ogential and obstetric problems. Blood 7 - 23 and 27 - 37 weeks of gestat ion and at 37 - 43 weeks of gestat ion for those who delivered at term. Mean cortisol levels were highe r in women who delivered preterm at 27 - 37 wee ks of g estation. 27 - 37 weeks: Cortisol levels were higher in the preterm group as compared to the term gro up . Hobel et al. (1999) Case control study design 524 pregnant women 18 preterm patients were matched with 18 term patie n ts. PSS, SSAI Blood 18 to 20 wee ks, 28 to 30 week s and 35 to 36 weeks of gestation Patients wh o delivered preterm had significantly elevated cortisol levels at 18 to 20 weeks’ gestation and 28 to 30 weeks’ gestation. Kramer et al. (2009) Prospective cohort study nested case control analysis 5337 pregnant women Demographic questionnaire, daily hassles scale, marital strain scale of pearlin and schooler, abu s e assessment screen, arizona social support interview s chedule, per ceived stress scale , dunkel-schetter scale, rosenberg self esteem scale, and CES-D Hair 24 - 26 weeks of gestation Pregnancy related anxiety and depression were associated with preterm b ir th . Hair cortisol was positively associated with gestational age but not CRH. Maternal plasma CRH, hair cortisol, and placental histopathologic of infection were not associated with stress, anxiety, or d istress me asures. Ruiz et al. (2001) Prospective longitudinal observational study design 78 pregnant women PSS Blood, vaginal swabs 15 - 19, 20 to 22, 23 - 26, 27 - 30, and 31 - 35 we eks of gestation Cortisol conce ntration did not correlate with gestational age at birth. The change in PSS scores was significantly related to gestational age at birth. Shaikh et al. (2010) Prospective cohort study design 143 pregnant women A-Z stress scale, CES-D scale Blood 28 weeks of gestation There were no significant relationship found between stress, depression, cortisol and preterm birth. socioeconomic background were followed till delivery but only 18 women who delivered preterm were matched with 18 wo- men who delivered at term. Moreover, Kramer, Lydon, et al. (2009) prospectively recruited 5337 pregnant women of Mont- real and conducted a nested case-control study. But, Ruiz et al. (2001) conducted a prospective, longitudinal, observational stu- dy in which 78 women were recruited and followed till delivery and divided into three groups: normal term (n = 53), preterm labor (n = 17), and preterm birth groups (n = 6). Shaikh (2011) conducted a prospective cohort study in which 132 women were recruited between 28 - 30 weeks of pregnancy and fol- lowed till delivery. Erickson et al. (2001) reported women with preterm birth had higher cortisol levels at 27 - 37 weeks of gestation, but no in- crease was reported at 7 - 23 weeks. Education level and work related variables (walking more than 6 hours a day, working more than 42 hours a week) were strongly associated with pre- term delivery. Moreover, Hobel et al. (1999) concluded that the preterm group had higher cortisol levels at 18 to 20 weeks and 28 to 30 weeks, but not at 35 to 36 weeks. In addition, Kramer et al. (2009) concluded that among multiple stress measure- ments, pregnancy related anxiety, perception of high pregnancy risk, and depression were associated with preterm birth. Hair cortisol was positively associated with gestational age but CRH was not. In contrast, Ruiz et al.’s (2001) study does not support the hypothesis that cortisol levels increases with stress, but it shows a significant relationship between stress and gestational age. Also, Shaikh (2011) study showed no significant relation- ship between stress, cortisol, and preterm birth. A few studies have been carried out to identify the relation- ship between maternal depression, cortisol levels, and preterm delivery and these show a significant relationship between the three variables (see Table 2) (Diego et al., 2009; Field et al., 2004, 2006; Field, Diego, Hernanzer-Rief et al., 2008). Field et al. (2004) compared 70 pregnant women with and without de- pression at 20 weeks of gestation by using the CES-D. The study findings showed a significantly greater number of prema- ture births in depressed women as compared to non-depressed women (25% versus 7%, P < 0.01). Field et al. (2006) recruited 300 pregnant women at 20 weeks of gestation and their urinary cortisol levels were collected at mid morning. The incidence of preterm was significantly higher in the group with high cortisol level. Diego et al. (2009) con- ducted a study in which 40 depressed and 40 non-depressed women were recruited on the basis of their CES-D score, which was measured in 18 and 20 weeks of gestation. The findings suggested that depressed mothers had a 13% higher incidence of preterm birth. Also, depressed women had more elevated pre- natal cortisol levels than non-depressed women. A study of 430 pregnant women, chronic prenatal depression and cortisol levels were assessed longitudinally at 22 and 32 weeks of gestation (Field, Diego, Hernandez-Reif et al., 2008).  K. SHAIKH ET AL. Table 2. Relationship between prenatal depression, cortisol, and preterm birth. Study Design Participants Scales Specimen Time period of measurement Results Field et al. (2004) Prospective longitudinal study design 70 pregnant women with depression and 70 without depression CES-D scale, STAI, profile mood states, anger scale, vagal tone, EEG asymmetry and neonata l behavior during sleep and during the brazelton neon atal behavior assessment sca l e Maternal and neonatal urine for cortisol, dopamine, and serotonin 20 weeks of gestation and within 24 hours of delivery The study findi ngs showed significantly greater number of prematur e births in depressed women as compared to non-depressed women (25% v ersus 7%, P < 0.01). Cortisol was a significant predictor of preterm birth. Field et al. (2006) Prospective cohort 300 pregnant women CES-D, structured clinical interview of diagnosis, STAI and STAXI, behaviour inhibition, and behaviour approach system questionnaire, neonatal assessments Urine cortisol 20 weeks of gestation The high cor ti sol group had higher CES-D scores. The fetus was more active an d had a smaller he ad circumference, abdominal circumference, biparietal diameter, less fetal we i g ht and a shorter gestational age. Diego et al. (2009) Prospective cohort study 40 depressed and 40 non-depressed pregnant w omen Schedule of recent life events, daily hassles, perceived stress scale, hopkins symptom checklist, and pregna n cy-related anxiety Urine cortisol 18 - 20 weeks of gestation ( i.e ., mid gestation) Depressed women had a 13% greater incidence of premature delivery than non-depressed women. Depressed women also had elevated prenatal cortisol levels than non-depressed women. Field, Diego, Hernandez- Reif et al. (2008) Prospective longitudinal study design 430 pregnant women SCID, CE S -D, STAI and STAXI, Daily hassles and urine cortisol 22 weeks and 32 weeks of gestation The depre ssed group had a higher cortisol levels as compared to the non-depre ss ed group on t he first prenatal visit but no difference in cortisol level wa s noted on the second visit. The depre ssed group had a higher rate of preterm birth than the non-depressed group. ACTH Adrenocorticotrophic Ho rmones, CBC Complete Blood Count , CRH Corticotrophin-releasing-hormones, ACTH Adrenocorticotrophic Hormones, PSS Perceived Stress Scale, SSAI The Spielberger State Anxiety Inventory, CES-D Centre for Epidemiology Studies Depression Scale, CRH Corticotrophin-releasing -hormon es, STAI State Anxiety Inventory , EEG Electroencephalography, STAXI State Anger Inventory, SCID Structured Clinical Interview for DSM IV Disorder. After delivery, postnatal depression was assessed and the rela- tionship with neonatal outcomes was assessed.The depressed group had higher cortisol levels as compared to the non-de- pressed group on the first prenatal visit but no difference in cortisol levels was noted on the second visit in the two groups. The depressed group had more incidences of preterm birth than the non-depressed group. Hence, all these studies highlight the significance of maternal cortisol as an important predictor for preterm delivery and an indicator of depression. Discussion The existing literature on the relationship between stress, de- pression, cortisol and preterm does not have a common, clear, and consistent definition of the concept of stress, as evident from the different measures of stress (i.e., the various scales) used. The researchers have used a variety of scales to measure stress which makes it difficult to compare the results. For in- stance, Whitehead et al. (2002) measured stress by negative life events, which included family illness, death, finances, job loss, relationships, physical injury, and legal matters, whereas Hobel et al. (1999) measured the perception of stress by using the PSS and Spielberger State Anxiety Inventory (STAI). Erickson et al. (2001) study included previous and present medical history, stressful life situations, and questions on behaviors, and present urogenital and obstetric history. Ruiz et al. (2001) used only the PSS. In addition, Wadhwa et al. (1993) assessed stress using multiple scales, such as Schedule of Recent Life Events, Daily Hassles Questionnaire, PSS, Hopkins Symptoms Checklist for measuring psychological and physical symptoms and Pregnan- cy Related Anxiety Scale. Obel et al. (2005) and Zhu et al. (2010) used Life Events Checklist. Shaikh et al. (2011) used A-Z stress scale. Moreover CES-D was use d to assess depress- ion (Diego et al., 2009; Fi el d et a l. , 2004, 2006; Shaikh et al., 2011). The varied variables for instance live events, daily hassles, social support used in different studies to assess stress during pregnancy makes it dif ficult to compar e the outco mes as varied measures are used. There has been no universal stan- dard method to measure stress in pregnant women. The lack of use of a standardized scale to measure stress contributes to the inability to confirm the association between maternal stress, cortisol level and preterm birth (Lantendresse, 2009; Paarlberg et al., 1995). The different inclusion and exclusion criteria used in studies may also explain the inconsistent findings. Erickson et al. (2001); Harville et al. (2009); Hobel et al. (1999); Kramer et al. (2009); Obel et al. (2003); Shaikh et al. (2011) and Zhu et al. (2010) enrolled primiparous and multiparous women, while Ruiz et al. (2001) enrolled only primiparous women. In addition, a few studies excluded women who received betamethasone (Eri- ckson et al.; Hobel et al.; Mazor et al., 1994, 1996; Shaikh et al.) whereas Harville et al.; Kramer et al.; Obel et al. (2003) and Copyright © 2013 SciRes. 28  K. SHAIKH ET AL. Ruiz et al. (2001) did not mention betamethasone treatment. Betamethasone affects the cortisol level and therefore may not highlight the relationship between stress, cortisol, and preterm delivery. Moreover, a few studies excluded women with diabe- tes mellitus, thyroid disorder, and chronic renal or heart disease and uterine and cervical abnormalitywhich are the risk factors for preterm birth and can impact the result (Diego et al., 2009; Kramer et al.; Ruiz et al.; Shaikh et al.; Zhu et al.). Cortisol undergoes diurnal variation. It is at its highest prior to awakening and decreases during the day and is at its lowest in the evening (Levine et al., 2007; Ruiz et al., 2001). Therefore, cortisol should be drawn in the morning or the afternoon, con- sistently, for each subject. Hobel et al. (1999) collected plasma cortisol level between 9 a.m. to 1 p.m. Harville et al. (2009) collected between 8 a.m. and 10 a.m. while Ruiz et al. (2001) collected plasma cortisol either in the morning or the afternoon, consistently, for each subject. Obel et al. (2005) collected morn- ing and evening sample. A number of studies collected first morning urine cortisol sample (Diego et al., 2009; Field, 2004, 2006). The different time period s in which stress and depressi on were measured may explain the variation in findings regarding the lin k be tw een st r ess, de p re ssi on, an d pr ete r m bir t h. Paa r lb e rg, Vingerhoets, Passchier, Dekker, and Geijn (1995) observed that an identical stressful condition led to different effects depend- ing on when during the pregnancy (i.e., which trimester) the stressful condition occurred whereas in late pregnancy the same stimuli can lead to preterm delivery. In their view stress in early pregnancy affects the developing fetus. The use of a longitudi- nal design, where multiple measurements are taken, will give a better understanding of the relationship between stress and pre- term delivery (Giurgescu, 2009). On the other hand, the Erickson et al. (2001) study collected serum cortisol but did not mention the time the sample was collected. The varied times of data collections may also explain the inconsistent findings. Some studies used blood (Erickson et al., 2001; Phocas et al., 1990; Hobel et al., 1999; Mazor et al., 1994, 1996; Ruiz et al., 2001) to measure the cortisol level whereas a few studies measured cortisol in urine (Diego et al., 2009; Field et al., 2004, 2006) and one study used hair to mea- sure cortisol (Kramer, et al., 2009) and two studies used sa- liva (Harville et al.; Obel et al.). Cortisol levels can be de- tected in blood, urine, and saliva. Urinary cortisol is a non- invasive procedure and a better way to measure cortisol than other measures for frequent and rapid sampling. Levine et al. (2007) explained the reason for preferring 24 hours urine sample for cortisol as “Urinary cortisol excretion results from glomerular filtration and is a useful index of integrated 24 hours plasma free cortisol” (p. 46). Therefore, urinary corti- sol may be a more accurate measure of maternal cortisol le- vels when a 24 hours urine collection for cortisol is taken rather than a single measure of urine for cortisol (Levine et al.). The studies examining the relationship between stress, corti- sol levels and preterm birth, shows inconsistent results. Some studies (Hobel et al., 1999; Erickson et al., 2001; Kramer et al., 2009) support the relationship between stress, cortisol, and pre- term births, whereas others (Ruiz et al., 2001; Harville et al., 2009) found cortisol to be a poor biomarker. In normal preg- nancy, the cortisol level increases throughout pregnancy and at mid pregnancy the level increases by 50% due to the production of CRH via placenta (Ruiz et al., 2001). Measuring stress once in a pregnancy may not provide an adequate appraisal of the psychosocial health of the women throughout the pregnancy. Hence, multiple measurements of stress variables are likely to provide a more in-depth understanding of the relationship be- tween stress and preterm birth. Even though there are inconsis- tencies in th e fin di ngs of th e stud ies th at ad dress t he r el ationsh ip between stress, depression, cortisol, and preterm birth, high levels of cortisol may be one of the strong biomarkers for pre- term delivery (Giurgescu, 2009). In other words, higher stress and depression scores and higher levels of cortisol when occur- ring together, may predict preterm birth. The relationship be- tween stress, depression, cortisol levels and preterm birth may be multifactorial and complex with premature birth being the final common pathway. Implications for Research Studies (Field et al., 2004, 2006; Field, Diego, Hernandez, et al., 2008) suggest that among pregnant women cortisol gets elevated with co-occurring anxiety and depression. Hence, add- ing an anxiety measure would enhance the psychological mea- sures and allow for more sophisticated data analyses, such as comparing women with elevated scores on both anxiety and de- pression. Furthermore, a recent study by Holzman et al. (2009) proposed other biomarkers, such as catecholamine level (e.g., epinephrine, norepinephrine, and dopamine) for preterm deliv- ery. Therefore, adding this biomarker in future studies may contribute to our understanding of the mechanism responsible for preterm birth. Moreover, such studies should be done using non-invasive methods to check cortisol hormone like saliva because it is easier and painless if multiple measures are going Finally, a longitudinal cohort study design should be under- taken in which stress, depression and cortisol are measured in each trimester. Implications for Practice Mental health of pregnant women is often not given priority. Medical and Nursing clinicians (e.g., community health nurses) and lady health visitors should integrate assessment of psycho- social factors as standard of care provided to pregnant women. Early identification of stress and depression will permit the medical and nursing clinicians to implement measures to reduce stress and depression caused by psychological factors and its potential negative consequences such as preterm birth (Laten- dresse, 2009). Decreasing the incidence of preterm birth may reduce infant which is an important fourth millennium devel- opment goal. In addition, nurses should be educated about the importance of the psychological aspect of care. Group prenatal care may be one of the strategies nurses can employ to reduce stress (Field & Diego, 2008). Ickovics et al. (2007) demonstrated that group prenatal care which includes physical assessment, education and skills building, and support through facilitated group discussion, reduced the incidence of preterm birth when compared to women who received individual prenatal care. Group prenatal care reduced the stress and the effects on ma- ternal and fetal endocrine stress response, minimizing the inci- dence of preterm birth. Health professionals (e.g., physicians, nurses and psycholo- gist) who have skills need to intervene in a timely way in order to lower the stress of pregnant women and to monitor the im- pact of their interventions to ensure that appropriate outcomes are attained. A number of interventions have been shown to re- duce stress, anxiety and depression or its negative consequen- Copyright © 2013 SciRes. 29 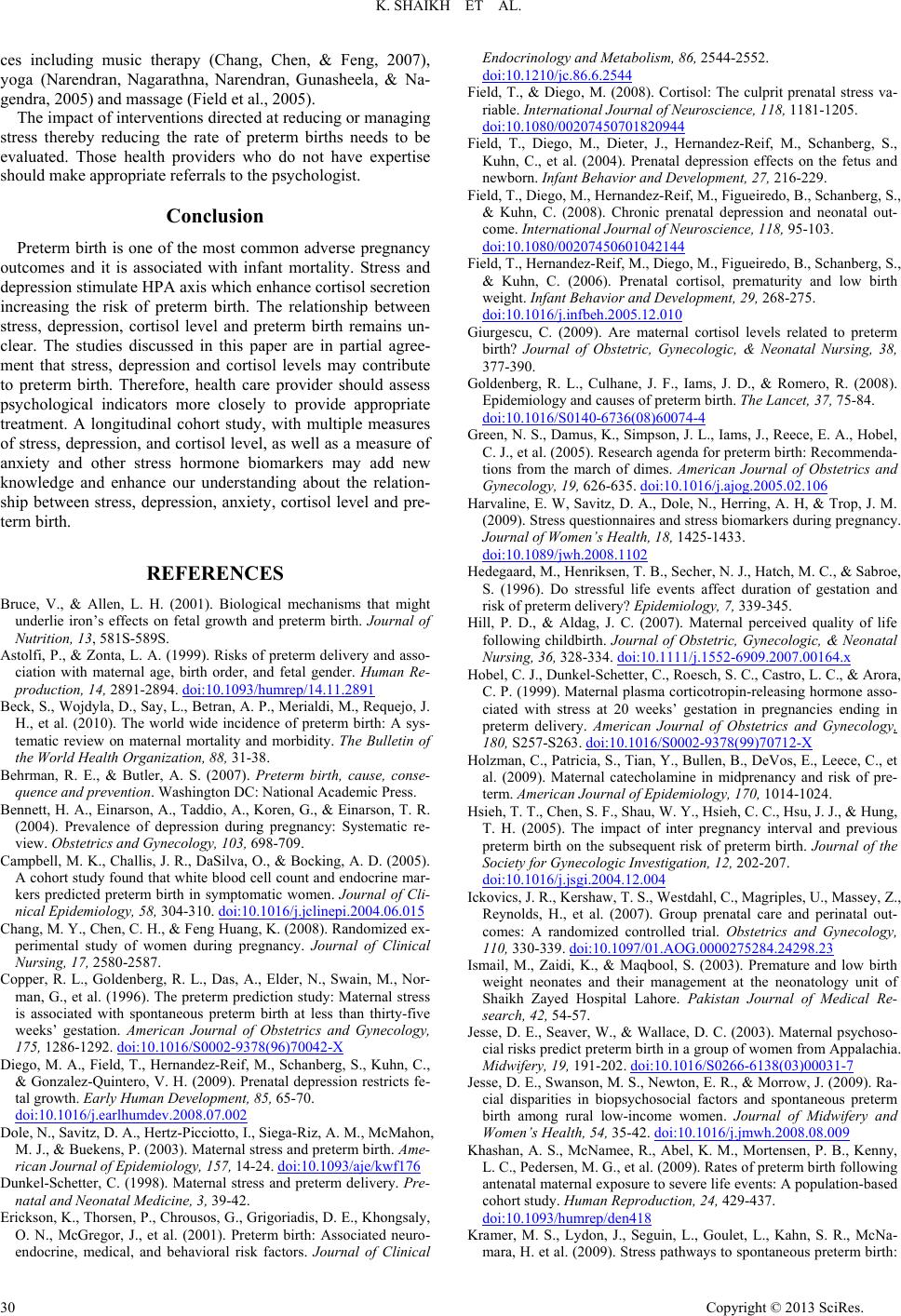 K. SHAIKH ET AL. ces including music therapy (Chang, Chen, & Feng, 2007), yoga (Narendran, Nagarathna, Narendran, Gunasheela, & Na- gendra, 2005) and massage (Field et al., 2005). The impact of interventions directed at reducing or managing stress thereby reducing the rate of preterm births needs to be evaluated. Those health providers who do not have expertise should make appropriate referrals to the psychologist. Conclusion Preterm birth is one of the most common adverse pregnancy outcomes and it is associated with infant mortality. Stress and depression stimulate HPA axis which enhance cortisol secretion increasing the risk of preterm birth. The relationship between stress, depression, cortisol level and preterm birth remains un- clear. The studies discussed in this paper are in partial agree- ment that stress, depression and cortisol levels may contribute to preterm birth. Therefore, health care provider should assess psychological indicators more closely to provide appropriate treatment. A longitudinal cohort study, with multiple measures of stress, depression, and cortisol level, as well as a measure of anxiety and other stress hormone biomarkers may add new knowledge and enhance our understanding about the relation- ship between stress, depression, anxiety, cortisol level and pre- term birth. REFERENCES Bruce, V., & Allen, L. H. (2001). Biological mechanisms that might underlie iron’s effects on fetal growth and preterm birth. Journal of Nutrition, 13, 581S-589S. Astolfi, P., & Zonta, L. A. (1999). Risks of preterm delivery and asso- ciation with maternal age, birth order, and fetal gender. Human Re- production, 14, 2891-2894. doi:10.1093/humrep/14.11.2891 Beck, S., Wojdyl a, D., Say, L., Betran, A. P ., Merialdi, M., Requejo, J. H., et al. (2010). The world wide incidence of preterm birth: A sys- tematic review on maternal mortality and morbidity. The Bulletin of the World Health Organization, 88, 31-38. Behrman, R. E., & Butler, A. S. (2007). Preterm birth, cause, conse- quence and prevention. Washington DC: Nat ional Academic Press. Bennett, H. A., Einarson, A., Taddio, A., Koren, G., & Einarson, T. R. (2004). Prevalence of depression during pregnancy: Systematic re- view. Obstetrics and Gynecology, 103, 698-709. Campbell, M. K., Challis, J. R., DaSilva, O., & Bocking, A. D. (2005). A cohort study found that white blood cell count and endocrine mar- kers predicted preterm birth in symptomatic women. Journal of Cli- nical Epidemiology, 58, 304-310. doi:10.1016/j.jclinepi.2004.06.015 Chang, M. Y., Chen, C. H., & Feng Huang, K. (2008). Randomized ex- perimental study of women during pregnancy. Journal of Clinical Nursing, 17, 2580-2587. Copper, R. L., Goldenberg, R. L., Das, A., Elder, N., Swain, M., Nor- man, G., et al. (1996). The preterm prediction study: Maternal stress is associated with spontaneous preterm birth at less than thirty-five weeks’ gestation. American Journal of Obstetrics and Gynecology, 175, 1286-1292. doi:10.1016/S0002-9378(96)70042-X Diego, M. A., Field, T., Hernandez-Reif, M., Schanberg, S., Kuhn, C., & Gonzalez-Quintero, V. H. (2009). Prenatal depression restricts fe- tal growth. Early Human Development, 85, 65-70. doi:10.1016/j.earlhumdev.2008.07.002 Dole, N., Savitz, D. A., Hertz-Picciotto, I., Siega-Riz, A. M., McMahon, M. J., & Buekens, P. (2003). Maternal stress and preterm birth. Ame- rican Journal of Epidemiology, 157, 14-24. doi:10.1093/aje/kwf176 Dunkel-Schetter, C. (1998). Maternal stress and preterm delivery. Pre- natal and Neonatal Medici ne , 3, 39-42. Erickson, K., Thorsen, P., Chrousos, G., Grigoriadis, D. E., Khongsaly, O. N., McGregor, J., et al. (2001). Preterm birth: Associated neuro- endocrine, medical, and behavioral risk factors. Journal of Clinical Endocrinology and Metabolism, 86, 2544-2552. doi:10.1210/jc.86.6.2544 Field, T., & Diego, M. (2008). Cortisol: The culprit prenatal stress va- riable. International Journal of Neuroscience, 118, 118 1-1205. doi:10.1080/00207450701820944 Field, T., Diego, M., Dieter, J., Hernandez-Reif, M., Schanberg, S., Kuhn, C., et al. (2004). Prenatal depression effects on the fetus and newborn. Infant Behavior and D ev el o pm en t, 27 , 216-229. Field, T., Diego, M., Hernandez-Reif, M., Figueiredo, B., Schanberg, S., & Kuhn, C. (2008). Chronic prenatal depression and neonatal out- come. International Journal of Neuroscience, 118, 95- 103. doi:10.1080/00207450601042144 Field, T., Hernand ez-Reif , M., Diego, M., Figueiredo, B., Schanberg, S., & Kuhn, C. (2006). Prenatal cortisol, prematurity and low birth weight. Infant Behavior and Developm e n t , 2 9 , 268-275. doi:10.1016/j.infbeh.2005.12.010 Giurgescu, C. (2009). Are maternal cortisol levels related to preterm birth? Journal of Obstetric, Gynecologic, & Neonatal Nursing, 38, 377-390. Goldenberg, R. L., Culhane, J. F., Iams, J. D., & Romero, R. (2008). Epidemiology and causes of pr eterm birth. The Lancet, 37, 75-84. doi:10.1016/S0140-6736(08)60074-4 Green, N. S., Damu s, K., Simpson, J. L., Iams, J., Reec e, E. A., Hobel, C. J., et al. (2005). Research agenda for preterm birth: Recommenda- tions from the march of dimes. American Journal of Obstetrics and Gynecology, 19, 626-635. doi:10.1016/j.ajog.2005.02.106 Harvaline, E. W, Savitz, D. A., Dole, N., Herring, A. H, & Trop, J. M. (2009). Stress questionnaires and stress biomarkers during pregnancy. Journal of Women’s Health, 18, 1425-1433. doi:10.1089/jwh.2008.1102 Hedegaard, M., Henriksen, T. B., Secher, N. J., Hatch, M. C., & Sab roe, S. (1996). Do stressful life events affect duration of gestation and risk of preterm delivery? Epidemiology, 7, 339-345. Hill, P. D., & Aldag, J. C. (2007). Maternal perceived quality of life following childbirth. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 36, 328-334. doi:10.1111/j.1552-6909.2007.00164.x Hobel, C. J., Dunkel-Schetter, C., Roesch, S. C., Castro, L. C., & Arora, C. P. (1999). Maternal plasma corticotropin-releasing hormone asso- ciated with stress at 20 weeks’ gestation in pregnancies ending in preterm delivery. American Journal of Obstetrics and Gynecology, 180, S257-S263. doi:10.1016/S0002-9378(99)70712-X Holzman, C., Patricia, S., Tian, Y., Bullen, B., DeVos, E., Leece, C., et al. (2009). Maternal catecholamine in midprenancy and risk of pre- term. American Journal of Epidemiology, 170, 1014-1024. Hsieh, T. T., Chen, S. F., Shau, W. Y., Hsieh, C. C., Hsu, J. J., & Hung, T. H. (2005). The impact of inter pregnancy interval and previous preterm birth on the subsequent risk of preterm birth. Journal of the Society for Gynecologic Investigation, 12, 202-207. doi:10.1016/j.jsgi.2004.12.004 Ickovics, J. R., Kershaw, T. S., Westdahl, C., Magriples, U., Massey, Z., Reynolds, H., et al. (2007). Group prenatal care and perinatal out- comes: A randomized controlled trial. Obstetrics and Gynecology, 110, 330-339. doi:10.1097/01.AOG.0000275284.24298.23 Ismail, M., Zaidi, K., & Maqbool, S. (2003). Premature and low birth weight neonates and their management at the neonatology unit of Shaikh Zayed Hospital Lahore. Pakistan Journal of Medical Re- search, 42, 54-57. Jesse, D. E., Seaver, W., & Wallace, D. C. (2003). Maternal psychoso- cial risks predict preterm birth in a group of women from Appalachia. Midwifery, 19, 191-202. doi:10.1016/S0266-6138(03)00031-7 Jesse, D. E., Swanson, M. S., Newton, E. R., & Morrow, J. (2009). Ra- cial disparities in biopsychosocial factors and spontaneous preterm birth among rural low-income women. Journal of Midwifery and Women’s Health, 54, 35- 42. doi:10.1016/j.jmwh.2008.08.009 Khashan, A. S., McNamee, R., Abel, K. M., Mortensen , P. B., Kenny, L. C., Pedersen, M. G., et al. (2009). Rates of preterm birth following antenatal maternal exposure to severe life events: A population-based cohort study. Human Re production, 24, 429-437. doi:10.1093/humrep/den418 Kramer, M. S., Lydon, J., Seguin, L., Goulet, L., Kahn, S. R., McNa- mara, H. et al. (2009). Stress pathways to spontaneous preterm birth: Copyright © 2013 SciRes. 30  K. SHAIKH ET AL. Copyright © 2013 SciRes. 31 The role of stressors, psychological distress, and stress hormones. American Journal of Epidemiology, 169, 1319-1326. doi:10.1093/aje/kwp061 Latendresse, G. (2009). The interaction between chronic stress and pregnancy: Preterm birth from a biobehavioral perspective. Journal of Midwifery and Women's Health, 54, 8-17. doi:10.1016/j.jmwh.2008.08.001 Levine, A., Zagoory-Sharon, O., Feldman, R., Lewis, J. G., & Weller, A. (2007). Measuring cortisol in human psychobiological studies. Physiology and Behavior, 90, 43-53. doi:10.1016/j.physbeh.2006.08.025 Mathews, T. J., & MacDorman, M. F. (2007). Infant mortality statistics from the 2004 period linked birth/infant death data set. National vital statistics reports, 55. http://www.cdc.gov/nchs/data/nvsr/nvsr57/nvsr57_02.pdf Mavalankar, D. V., Gray, R. H., & Trivedi, C. R. (1992). Risk factors for preterm and term low birthweight in Ahmedabad, India. Interna- tional Journal of Epidemiology, 21, 2 63-272. doi:10.1093/ije/21.2.263 Mazor, M., Chaim, W., Hershkowitz, R., Levy, J., Leiberman, J. R., & Glezerman, M. (1994). Association between preterm birth and in- creased maternal plasma cortisol concentrations. Obstetrics and Gy- necology, 84, 521-524. Mazor, M., Hershkowitz, R., Ghezzi, F., Cohen, J., Silber, A., Levy, J. et al. (1996). Maternal plasma and amniotic fluid 17 beta-estradiol, progesterone and cortisol concentrations in women with successfully and unsuccessfully treated preterm labor. Archives of Gynecology and Obstetrics, 258, 89-96. doi:10.1007/BF00626029 Narendran, S., Nagrathna, R., Narendran, V., Gunasheela, S., & Rao, N. H. R. (2005). Efficacy of yoga on pregnancy outcome. The Journal of Alternative and Complementary Medicine , 11, 237-244. doi:10.1089/acm.2005.11.237 Obel, C., Hedegaard, M., Henriksen, T. B., Secher. N. J., Olsen, J., & Levine, S. (2005). Stress and salivary cortisol during pregnancy. Psychoneuroendrocrinology, 30, 647-656. doi:10.1016/j.psyneuen.2004.11.006 Paarlberg, K. M., Vingerhoets, A. D., Passchier, J., Dekker, G. A., & Van Geijn, H. P. (1995). Psychosocial factors and pregnancy out- come: A review with emphasis on methodological issues. Journal of Psychosomatic Research, 39, 563-595. doi:10.1016/0022-3999(95)00018-6 Pearl, M., Braveman, P., & Abrams, B. (2001). Relationship of socio- economic characteristics to birthweight among 5 ethnic groups in California. American Journ al of P ublic Health, 91, 1808-1814. doi:10.2105/AJPH.91.11.1808 Phocas, I., Sarandakou, A., & Rizos, D. (1990). Maternal serum total cortisol levels in normal and pathologic pregnancies. International Journal of Gynecology and Obstetrics, 31, 3-8. doi:10.1016/0020-7292(90)90173-I Rafati, S., Borna, H., Akhavirad, M. B., & Fallah, N. (2005). Maternal determinants of giving birth to low-birth-weight neonates. Archives of Iranian Medicine, 8, 277-281. Russell, R. B., Green, N. S., Meikle, S., Meikle, S., Howse, S., Posch- man, K. et al. (2007). Cost of hospitalization for preterm and low birth weight infants in the United States. Pediatric, 120, e1-e9. doi:10.1542/peds.2006-2386 Ruiz, R. J., & Avant, K. C. (2005). Effects of maternal prenatal stress on infant outcomes: A synthesis of the literature. Advances in Nurs- ing Science, 28, 345-355. Ruiz, R. J., Fullerton, J., Brown, C. E. L., & Schoolfield, J. (2001). Relationships of cortisol, perceived stress, genitourinary infections, and fetal fibronectin to gestational age at birth. Biological Research for Nursing, 3, 39-47. doi:10.1177/109980040100300106 Sandman, C. A., Glynn, L., Schetter, C. D., Wadhwa, P., Garite, T., Chicz-DeMet, A. et al. (2006). Elevated maternal cortisol early in pregnancy predicts third trimester levels of placental corticotropin releasing hormone (CRH): Priming the placental clock. Peptides, 27, 1457-1463. doi:10.1016/j.peptides.2005.10.002 Shaikh, K., Premji, S. S., Rose, M. R., Kazi, A., Khowaja, S., & Tough, S. (2011). The association between parity, infant gender, high level of paternal education and preterm birth in Pakistan: A cohot study. BMC Pregnancy Childbirth, 11, 1-10. doi:10.1186/1471-2393-11-88 Steer, P. (2005). The epidemiology of preterm labor. International Journal of Obstetrics and Gynecology-Supplements, 112, 1-3. The World Bank (2008). Mor tality rate, infant (per 1,000 live births). http://data.worldbank.org/indicator/SP.DYN.IMRT.IN/countries/latest? display=default. Wadhwa, P. D., Culhane, J. F., Virginia, R., & Brave, S. (2001). Stress and preterm birth: Neuroendocrine, immune/inflamattory, and vas- cular mechanisms. Maternal and Child Health Journal, 5, 119-125. doi:10.1023/A:1011353216619 Wadhwa, P. D., Sandman, C. A., Porto, M., Dunkel-Schetter, C., & Garite, T. J. (1993). The association between prenatal stress and in- fant birth weight and gestational age at birth: A prospective investi- gation. American Journal of Obstetrics and Gynecology, 169, 858- 865. doi:10.1016/0002-9378(93)90016-C Whitehead, N., Hill, H. A., Brogan, D. J., & Blackmore-Prince, C. (2002). Exploration of threshold analysis in the relation between stressful life events and preterm delivery. American Journal of Epi- demiology, 15, 117-124. doi:10.1093/aje/155.2.117 Zhu, P., Tao, F., Hao, J. H., Sun, Y., Jiang, S., Jiang, X. (2010). Prena- tal life events stress: Implications for preterm birth and infant birth weight. American Journal o f O bs t et rics and Gynecology, 204 , e1-e8. doi:10.1016/j.ajog.2010.02.023
|