A. Z. KALEEM ET AL.
Copyright © 2013 SciRes. SS
353
common disorders of the colon and regarded as pre-ma-
lignant conditions. The majority of colonic polyps are
amenable to endoscopic snare excision. Large flat or in-
accessible right sided polyps pose a problem to safe en-
doscopic excision. The danger of incomplete excision or
perforation of the colon is significant, particularly in thin
walled caecum and ascending colon, and varies amongst
reports to as much as 3% [2]. Laparoscopic assisted colono-
scopic polypectomies are now well established for the
removal of such polyps and provide the extra security of
an intra-abdominal, serosal view of the colon whilst the
endoscopist is removing the polyp via snare [5]. Thus in
the case of perforation, it may be identified and treated
immediately. In addition, the use of the colonoscope al-
lows for accurate location of the polyp and thus mini-
mizing the need for colonic mobilization, with the excep-
tion of posterior/lateral wall located polyp. In this ap-
proach, the polyp is removed piecemeal and without sur-
rounding margins and thus histological comments on the
complete excision are difficult. There is also the consid-
eration of a late perforation due to diathermy injury
which may not be evident at the time of laparoscopy/
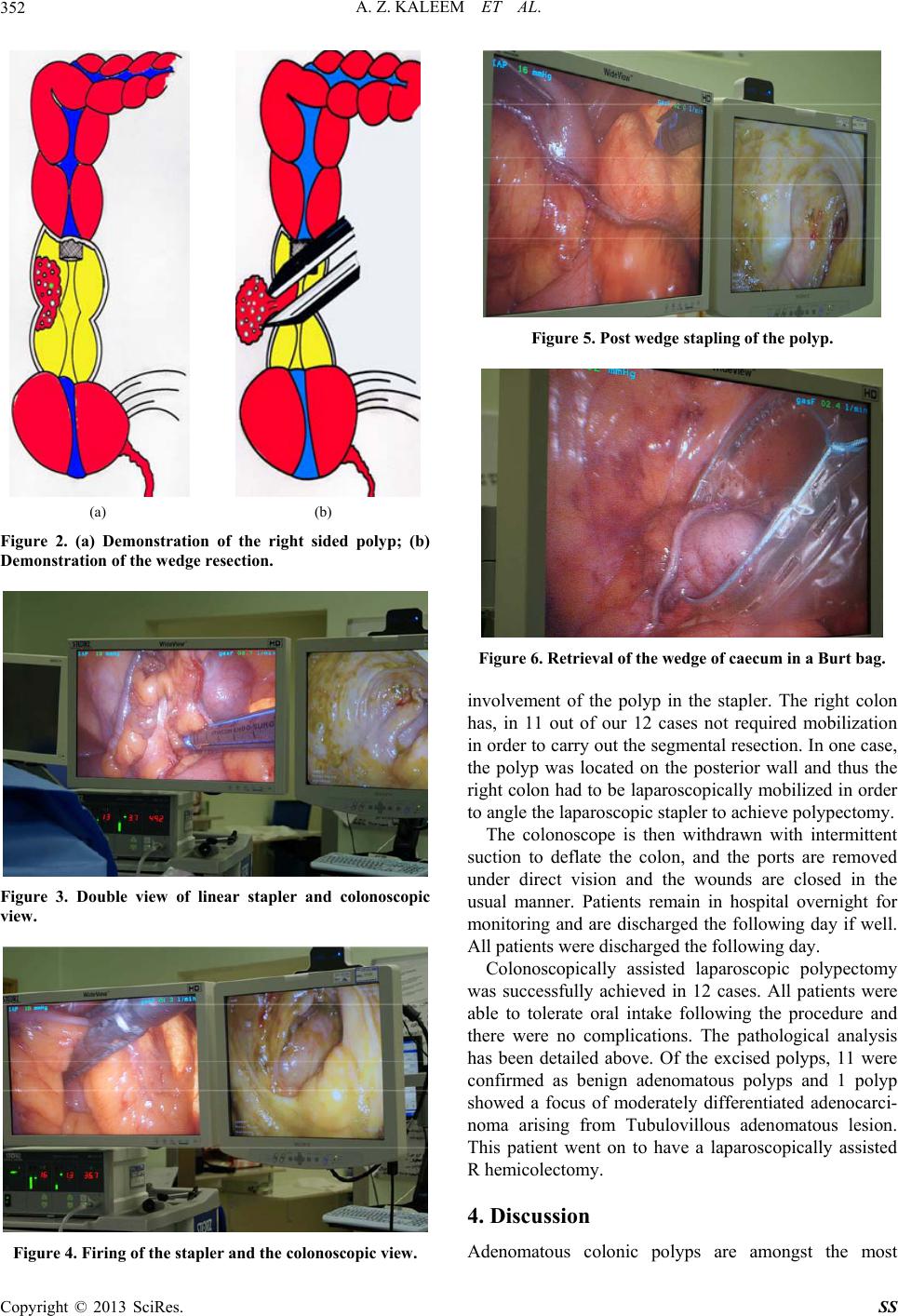
colonoscopy. We describe an alternative technique to
ensure complete polyp and margin removal, as a simple
wedge resection with the combination of laparoscopy and
colonoscopy. This technique has previously been de-
scribed, in association with the laparoscopic assisted
EMR, but not as a definitive procedure in its own right
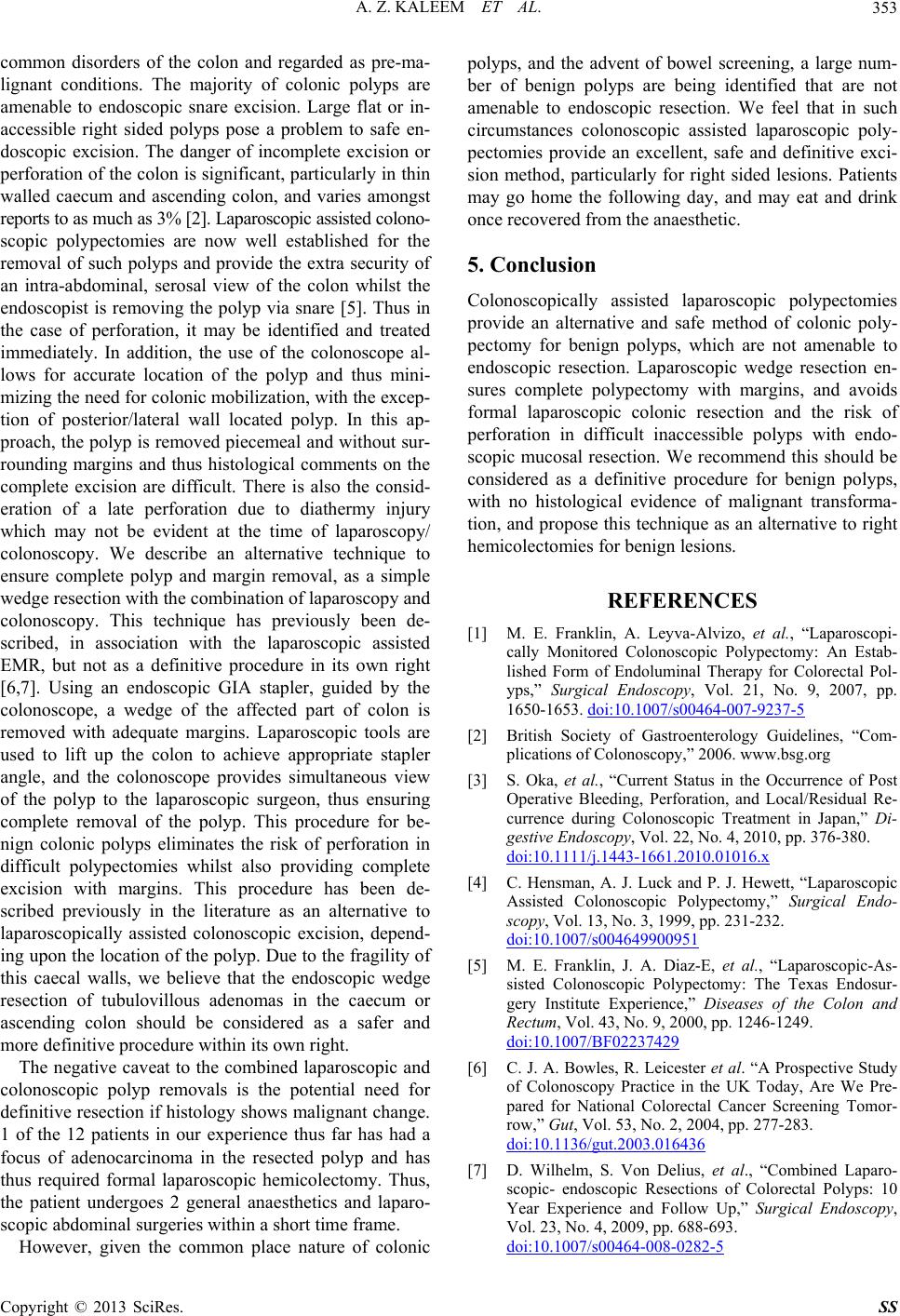
[6,7]. Using an endoscopic GIA stapler, guided by the
colonoscope, a wedge of the affected part of colon is
removed with adequate margins. Laparoscopic tools are
used to lift up the colon to achieve appropriate stapler
angle, and the colonoscope provides simultaneous view
of the polyp to the laparoscopic surgeon, thus ensuring
complete removal of the polyp. This procedure for be-
nign colonic polyps eliminates the risk of perforation in
difficult polypectomies whilst also providing complete
excision with margins. This procedure has been de-
scribed previously in the literature as an alternative to
laparoscopically assisted colonoscopic excision, depend-
ing upon the location of the polyp. Due to the fragility of
this caecal walls, we believe that the endoscopic wedge
resection of tubulovillous adenomas in the caecum or
ascending colon should be considered as a safer and
more definitive procedure within its own right.
The negative caveat to the combined laparoscopic and
colonoscopic polyp removals is the potential need for
definitive resection if histology shows malignant change.
1 of the 12 patients in our experience thus far has had a
focus of adenocarcinoma in the resected polyp and has
thus required formal laparoscopic hemicolectomy. Thus,
the patient undergoes 2 general anaesthetics and laparo-
scopic abdominal surgeries within a short time frame.
However, given the common place nature of colonic
polyps, and the advent of bowel screening, a large num-
ber of benign polyps are being identified that are not
amenable to endoscopic resection. We feel that in such
circumstances colonoscopic assisted laparoscopic poly-
pectomies provide an excellent, safe and definitive exci-
sion method, particularly for right sided lesions. Patients
may go home the following day, and may eat and drink
once recovered from the anaesthetic.
5. Conclusion
Colonoscopically assisted laparoscopic polypectomies
provide an alternative and safe method of colonic poly-
pectomy for benign polyps, which are not amenable to
endoscopic resection. Laparoscopic wedge resection en-
sures complete polypectomy with margins, and avoids
formal laparoscopic colonic resection and the risk of
perforation in difficult inaccessible polyps with endo-
scopic mucosal resection. We recommend this should be
considered as a definitive procedure for benign polyps,
with no histological evidence of malignant transforma-
tion, and propose this technique as an alternative to right
hemicolectomies for benign lesions.
REFERENCES
[1] M. E. Franklin, A. Leyva-Alvizo, et al., “Laparoscopi-
cally Monitored Colonoscopic Polypectomy: An Estab-
lished Form of Endoluminal Therapy for Colorectal Pol-
yps,” Surgical Endoscopy, Vol. 21, No. 9, 2007, pp.
1650-1653. doi:10.1007/s00464-007-9237-5
[2] British Society of Gastroenterology Guidelines, “Com-
plications of Colonoscopy,” 2006. www.bsg.org
[3] S. Oka, et al., “Current Status in the Occurrence of Post
Operative Bleeding, Perforation, and Local/Residual Re-
currence during Colonoscopic Treatment in Japan,” Di-
gestive Endoscopy, Vol. 22, No. 4, 2010, pp. 376-380.
doi:10.1111/j.1443-1661.2010.01016.x
[4] C. Hensman, A. J. Luck and P. J. Hewett, “Laparoscopic
Assisted Colonoscopic Polypectomy,” Surgical Endo-
scopy, Vol. 13, No. 3, 1999, pp. 231-232.
doi:10.1007/s004649900951
[5] M. E. Franklin, J. A. Diaz-E, et al., “Laparoscopic-As-
sisted Colonoscopic Polypectomy: The Texas Endosur-
gery Institute Experience,” Diseases of the Colon and
Rectum, Vol. 43, No. 9, 2000, pp. 1246-1249.
doi:10.1007/BF02237429
[6] C. J. A. Bowles, R. Leicester et al. “A Prospective Study
of Colonoscopy Practice in the UK Today, Are We Pre-
pared for National Colorectal Cancer Screening Tomor-
row,” Gut, Vol. 53, No. 2, 2004, pp. 277-283.
doi:10.1136/gut.2003.016436
[7] D. Wilhelm, S. Von Delius, et al., “Combined Laparo-
scopic- endoscopic Resections of Colorectal Polyps: 10
Year Experience and Follow Up,” Surgical Endoscopy,
Vol. 23, No. 4, 2009, pp. 688-693.
doi:10.1007/s00464-008-0282-5