 Psychology 2013. Vol.4, No.6A1, 39-44 Published Online June 2013 in SciRes (http://www.scirp.org/journal/psych) http://dx.doi.org/10.4236/psych.2013.46A1006 Copyright © 2013 SciRes. 39 Coping Strategies and Self-Efficacy for Diabetes Management in Older Mexican Adults Mónica Hattori-Hara, Ana Luisa González-Celis Division of Research and Graduate, Faculty of Higher Education Iztacala, National Autonomous University of Mexico, Mexico City, Mexico Email: saku678@yahoo.com.mx, algcr10@hotmail.com Received March 27th, 2013; revised April 28th, 2013; accepted May 27th, 2013 Copyright © 2013 Mónica Hattori-Hara, Ana Luisa González-Celis. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Diabetes Mellitus 2 (DM2) affects 20% of the elderly population in Mexico, causes disability and death, and demands many life-style changes. Since DM2 control is largely responsibility of the patient, man- agement itself is source of stress. Coping is a process by which persons face stressful situations, and ac- tive coping have proved being effective in disease control. Social-cognitive perspective suggests that self- efficacy believes can regulate human functioning, therefore they could promote specific coping if rela- tions between them are found. The study aim was to examine the association between coping strategies and self-efficacy in DM2 management in a group of 126 Mexican adults over 54 years old (X= 68.57, SD = 7.19), which answered an interview about sociodemographics data, self-efficacy in diabetes and coping strategies. The most common kind of coping used by the sample was self-recreation (X= 50.41, SD = 19.50) and religious faith (X= 50.04, SD = 17.65), and in self-efficacy the domain of taking the medicines had the greater score (X= 90.25, SD = 16.08). Total score in self-efficacy had significant cor- relations with active coping (r = .402, p ≤ .01) and self-recreation (r = .291, p ≤ .01). We concluded that there are relationships between self-efficacy beliefs in diabetes management and active coping. The cor- relation found can be used to guide future interventions with these patients, but the relation should be studied deeper for directional search, if is proved that DM self-efficacy beliefs enhance active coping; self-efficacy based interventions should be promote. Keywords: Elderly; Diabetes Mellitus; Problem Focus Coping; Self-Efficacy Introduction Currently proportion of old adults is increasing in the world population (United Nations, 2002), specifically in Mexico in 2005 a total of 7.8 million people representing 7.5% of the total habitants were over 60 years old, by 2010 this number in- creased to 9.3 million people (8.6%) and it is projected that the elderly population in Mexico will reach 33.5 million (27.5%) in 2050 (National Population Council [CONAPO], 2010). In the seniors diseases developed by the habits of a lifetime are often present, so as age increases the number of people with chronic diseases increases too (Bazo, Garcia, Maiztegui, & Martinez, 1999; Romero-Martínez et al., 2012). Among chronic diseases, diabetes mellitus type 2 (DM2) is a major cause of disability and death (Gutierrez, 2004; Interna- tional Diabetes Federation, 2012; National System of Health Information, 2005; Zuñiga, Garcia, & Partida, 2004), affects more than 20% of people over 60’s (American Diabetes Asso- ciation, 2001; Latin American Diabetes Association, 2008) and is rapidly expanding in Mexico (Olaiz et al., 2003; Villalpando et al., 2010). Due to fast expansion and negative impact of DM2 on old people’s lives, is crucial to address its control and management. To control DM2, glycemic regulation is needed, and to reach it, medical therapy alone is not enough; it must be combined with healthy lifestyle habits (Cornell & Briggs, 2004; Horton, Cefalu, Haines, & Siminerio, 2008) also known as DM2 man- agement behaviors as, inter alia, healthy eating, physical activ- ity, taking medication and risk reduction (American Association of Diabetes Educator, 2011a). In the third age replace patient’s lifetime habits with DM2 management behaviors is stressful. So disease management combined with changes and peculiarities in the elderly, con- tinuously face patients to external and internal demands often assessed as overwhelming and exceeding individual resources; forcing the person to perform cognitive and behavior efforts in order to handle the situations, this process is known as coping (Lazarus & Folkman, 1991). Coping is defined isolated from the results it have, the term is used whether the process is adaptative or nonadaptative (Lazarus & Folkman, 2000), however one of the aims of the researchers in this area is studying the effects of coping on adaptative outcomes (Lazarus, 1993), it means to find which strategies of coping are the ones that seeking to handle the situation help the patient promote and maintain overall health, ensure good quality of life and reduce sources of physical and emotional distress. There are many coping classifications (Ephrem, 1986; Katz,  M. HATTORI-HARA, A. L. GONZÁLEZ-CELIS Ritvo, Irvine, & Jackson, 1996; Monfort & Tréhel, 2012; Schwarzer & Schwarzer, 1996), but at least, coping as a process emphasizes that there are two broad functions: problem-focused which aims managing the stressor and emotion-focused which tackle the person’s affective responses to the stressor (Carver, Scheier, & Weintraub, 1989; Lazaruz & Folkman, 1984). In DM2 as the patients themselves are the most determining factor of treatment success (American Association of Diabetes Educator, 2011b; Pérez, 2003), strategies that guide persons to perform self-management behaviors in their lifestyle (problem focused coping) as search of solutions, use of social support and stress management skills (Fisher, Thorpe, McEvoy, & DeVellis, 2007) have proved effective for adaptation. Mean- while emotion-focused coping have not been significant related to overall adjustment in DM (Duangdao & Roesch, 2008) but has been significantly associated with greater perceived stress, problem areas in diabetes, and negative appraisals of diabetes control (Samuel-Hodge, Watkins, Rowell, & Hooten, 2008). Moreover, among psychological factors related to DM2 man- agement in addition to coping, self-efficacy have been positive correlated with disease management behaviors (Annesi, 2011; Ellis et al., 2004; Riveros, Cortazar-Palapa, Alcazar, & Sán- chez-Sosa, 2005; Steed et al., 2005; Wagner & Tennen, 2007) and reduced stress response in DM (Kanbara et al., 2008; Schokker et al., 2011). From a social-cognitive framework it is proposed that self- efficacy regulates human functioning through; selection, cogni- tive, motivational and emotional processes (Bandura, 1997). In this sense, human behavior guided by the beliefs about our ability to act, influence health directly through cognitive and emotional processes by activate biological system that mediates health and disease. On the other hand self-efficacy beliefs through motivational and selection processes, influence health indirectly by promoting or decrementing health habits (Bandura, 2004), from considering a change of habits and choice of tar- gets, to carry them out and keep changes reached (Bandura, 1999). In summary problem focus coping and greater self-efficacy in DM2 management are related to better self-management be- haviors, but the relation between self-efficacy and coping stra- tegies has been less explored and remains unclear. Coping used will be crucial to achieve control over the disease (Thoolen et al., 2008) and self-efficacy in DM management relate in how the individual copy with stressful situations (Gillibrand & Ste- venson, 2006; Wagner & Tennen, 2007), so the aim of this study was to analyze the association between disease coping type and levels of self-efficacy for managing DM2 in general and its factors (eating, exercising, glycemic monitoring risk reduction) a group of elderly Mexicans citizens use. According to the review we hypothesize that self-efficacy for managing DM2 in general and its factors, have positive asso- ciation with problem focus coping or related to any task to manage the disease (active and self-recreation coping) and not with emotion focus coping (depressive and religious faith copy- ing). Method Participants We interviewed 126 patients older than 54 years (mean = 68.57, SD = 7.19), with at least one year of DM2 diagnosis (1 to 53 years), who attended an outpatient public health clinic in Mexico City in any of its shifts (morning and afternoon), twenty were excluded for having missing values by more than 20% in any of the instruments. Of the respondents 44.3% reported having developed com- plications from DM2, which in 68.1% of cases were chronic and 31.9% were acute. People cognitive and audition impaired were excluded. In total 52.8% were females and 47.2% were males. The majority were dedicated to housework (38.7%) or were retired (36.8%) and only 22.6% were employed or worked outside home, of all the sample 11.3% lived alone, 42.5% lived only with their partner, 22.6% with their partner and others, while 23.5% were living without a partner but with others. Procedure Data collection was done in interview format, in an office or the waiting room of the health clinic, in a single session of 20 - 30 minutes. With support of the receptionists potential participants were detected, researchers approached them to introduce themselves, gave a brief explanation of the study and invited to participate; those who accepted were asked to accompany the interviewer in a more private space. Then the interviewer read the informed consent based on the ethical principles of the Helsinki code, clarifying the confidentiality of the information provided and its use only for research purposes. Signed the informed consent, the interview was conducted. Data were analyzed using the statistical package SPSS Statistics 19. Measures Socio-demographic data were collected from the patient through a structured interview and the following instruments were applied. The Friburgo Coping Questionnaire (FKS-LIS) Spanish ver- sion (Oviedo-Gomez, 2007). Developed by Muthny in 1989 in Germany, and designed for people over 16 years of age with sequels of chronic or acute disease, this instrument consists of five scales, with an Alpha of .68 that covers a wide range of coping strategies on cognitive, emotional and behavioral levels (Muthny, n.d.). Rose, Hildebrandt, Fliege, Klapp and Schirop (2002) vali- dated this scale in English with a sample of 350 chronic or acute patients, obtaining an Alpha of .734. Furthermore Ovi- edo-Gomez (2007) translated and applied this scale in Mexico, obtaining an Alpha of .75 for the total scale of 35 items. To increase the Alpha coefficient of each subscale, six items (11, 12, 20, 29, 32 and 33) and the subscale of “reduce importance to the disease” (2, 3, 4 and 31) were removed, thereby resulting in a questionnaire with 25 items with an Alpha of .723. The four subscales remaining in this instrument are the depressive (8 items, α = .67), active (7 items, α = .64), self-recreation (4 items, α = .63) and religious faith coping (6 items, α = .55). Some examples of its items are for depressive coping “I feel pity of myself”, “I isolate from others”; for active coping “I seek information of the disease and its treatment”, “I show my feelings to others”; for self-recreation coping “I try to distract myself”, “I give more permits to myself”; and for religious faith coping “I accept illness as destiny”, “I seek solace in religious faith”. Each item was assessed on a Likert scale of five points, in which the higher the score the greater the use of the strategy. Copyright © 2013 SciRes. 40 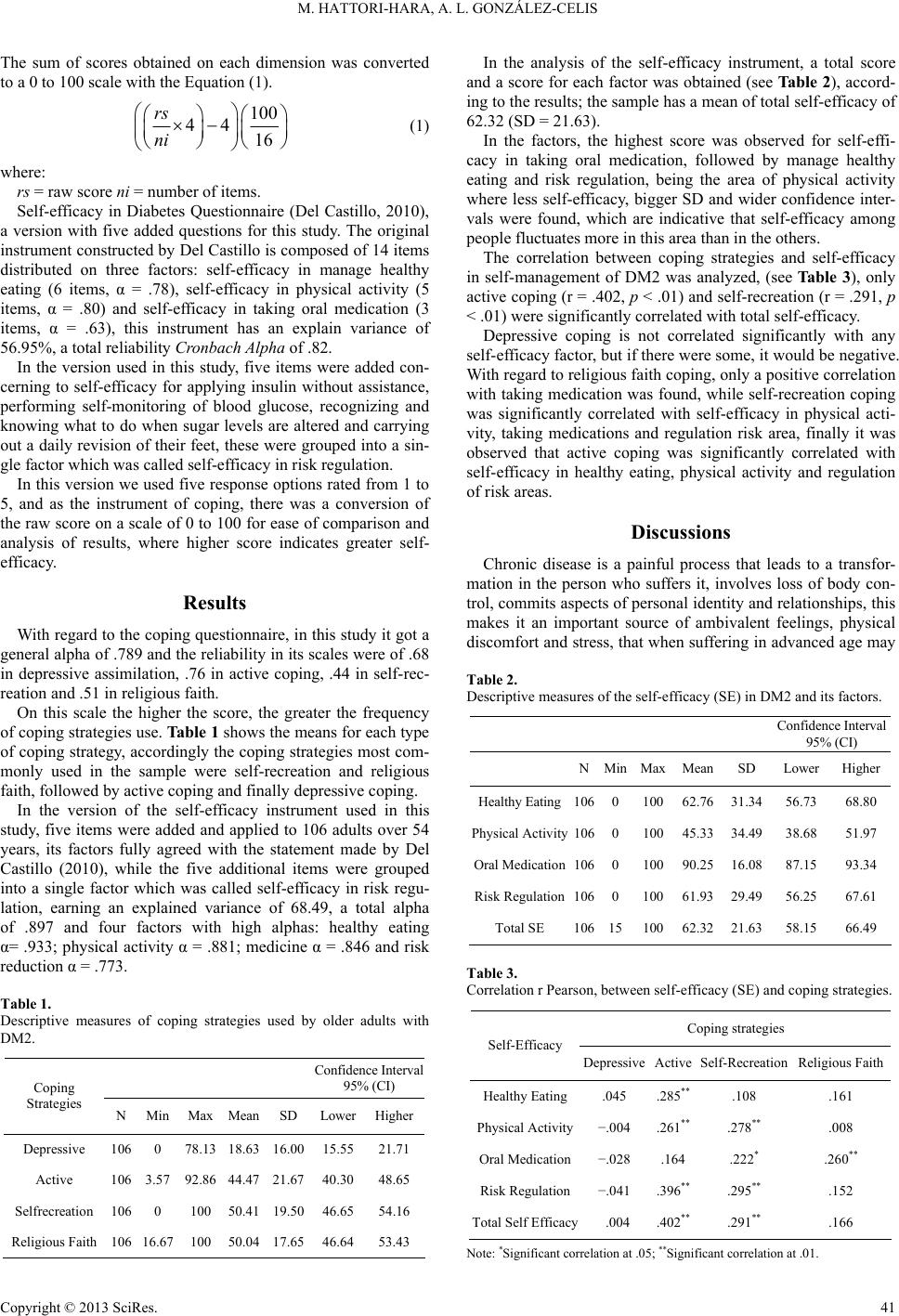 M. HATTORI-HARA, A. L. GONZÁLEZ-CELIS The sum of scores obtained on each dimension was converted to a 0 to 100 scale with the Equation (1). 100 4416 rs ni (1) where: rs = raw score ni = number of items. Self-efficacy in Diabetes Questionnaire (Del Castillo, 2010), a version with five added questions for this study. The original instrument constructed by Del Castillo is composed of 14 items distributed on three factors: self-efficacy in manage healthy eating (6 items, α = .78), self-efficacy in physical activity (5 items, α = .80) and self-efficacy in taking oral medication (3 items, α = .63), this instrument has an explain variance of 56.95%, a total reliability Cro nbach Al pha of .82. In the version used in this study, five items were added con- cerning to self-efficacy for applying insulin without assistance, performing self-monitoring of blood glucose, recognizing and knowing what to do when sugar levels are altered and carrying out a daily revision of their feet, these were grouped into a sin- gle factor which was called self-efficacy in risk regulation. In this version we used five response options rated from 1 to 5, and as the instrument of coping, there was a conversion of the raw score on a scale of 0 to 100 for ease of comparison and analysis of results, where higher score indicates greater self- efficacy. Results With regard to the coping questionnaire, in this study it got a general alpha of .789 and the reliability in its scales were of .68 in depressive assimilation, .76 in active coping, .44 in self-rec- reation and .51 in religious faith. On this scale the higher the score, the greater the frequency of coping strategies use. Table 1 shows the means for each type of coping strategy, accordingly the coping strategies most com- monly used in the sample were self-recreation and religious faith, followed by active coping and finally depressive coping. In the version of the self-efficacy instrument used in this study, five items were added and applied to 106 adults over 54 years, its factors fully agreed with the statement made by Del Castillo (2010), while the five additional items were grouped into a single factor which was called self-efficacy in risk regu- lation, earning an explained variance of 68.49, a total alpha of .897 and four factors with high alphas: healthy eating α= .933; physical activity α = .881; medicine α = .846 and risk reduction α = .773. Table 1. Descriptive measures of coping strategies used by older adults with DM2. Confidence Interval 95% (CI) Coping Strategies N Min Max Mean SD LowerHigher Depressive 106 0 78.13 18.63 16.00 15.5521.71 Active 106 3.57 92.86 44.47 21.67 40.3048.65 Selfrecreation 106 0 100 50.41 19.50 46.6554.16 Religious Faith 106 16.67 100 50.04 17.65 46.6453.43 In the analysis of the self-efficacy instrument, a total score and a score for each factor was obtained (see Ta ble 2), accord- ing to the results; the sample has a mean of total self-efficacy of 62.32 (SD = 21.63). In the factors, the highest score was observed for self-effi- cacy in taking oral medication, followed by manage healthy eating and risk regulation, being the area of physical activity where less self-efficacy, bigger SD and wider confidence inter- vals were found, which are indicative that self-efficacy among people fluctuates more in this area than in the others. The correlation between coping strategies and self-efficacy in self-management of DM2 was analyzed, (see Ta b le 3), only active coping (r = .402, p ˂ .01) and self-recreation (r = .291, p ˂ .01) were significantly correlated with total self-efficacy. Depressive coping is not correlated significantly with any self-efficacy factor, but if there were some, it would be negative. With regard to religious faith coping, only a positive correlation with taking medication was found, while self-recreation coping was significantly correlated with self-efficacy in physical acti- vity, taking medications and regulation risk area, finally it was observed that active coping was significantly correlated with self-efficacy in healthy eating, physical activity and regulation of risk areas. Discussions Chronic disease is a painful process that leads to a transfor- mation in the person who suffers it, involves loss of body con- trol, commits aspects of personal identity and relationships, this makes it an important source of ambivalent feelings, physical discomfort and stress, that when suffering in advanced age may Table 2. Descriptive measures of the self-efficacy (SE) in DM2 and its factors. Confidence Interval 95% (CI) NMinMaxMean SD LowerHigher Healthy Eating106010062.76 31.34 56.7368.80 Physical Activity106010045.33 34.49 38.6851.97 Oral Medication106010090.25 16.08 87.1593.34 Risk Regulation106010061.93 29.49 56.2567.61 Total SE 1061510062.32 21.63 58.1566.49 Table 3. Correlation r Pearson, between self-efficacy (SE) and coping strategies. Coping strategies Self-Efficacy Depressive Active Self-Recreation Religious Faith Healthy Eating.045 .285** .108 .161 Physical Activity−.004 .261** .278** .008 Oral Medication−.028 .164 .222* .260** Risk Regulation−.041 .396** .295** .152 Total Self Efficacy .004 .402** .291** .166 Note: *Significant correlation at .05; **Significant correlation at .01. Copyright © 2013 SciRes. 41  M. HATTORI-HARA, A. L. GONZÁLEZ-CELIS be of greater magnitude, impacting the quality of life and func- tioning of the elderly (Gonzalez-Celis, 2002, 2005), so in old age and disease, the development of coping skills are key for optimum fit to both processes. In DM2 to achieve good glycemic control is necessary to carry out self-management behaviors (Haire, 1996; Pérez, 2003) but self-management itself represents a stressful situation which need continue adaptation. Frojan and Rubio (2004) found that taking oral medicine is considered by the patients as the most important and simple behavior to make, as opposed to changes in lifestyles (diet, exercise, risk reduction and stress manage- ment) that seemed complicated and secondary to the treatment. Results in the present study agree with that, here the dimension referred to taking medication was the one with higher self-effi- cacy, so presumably patients tend to perceive a lower self-effi- cacy to change the other health habits, and that is why they assess them as more threatening and difficult to adopt. Thinking that SE beliefs and outcomes expectations could guide people choose challenges and goals, quantity of effort to invest, time of perseverance facing difficulties and way of in- terpret failures as motivational or disheartening (Del Castillo, 2010), help us to understand why commitment to incorporate medical treatment in daily life is easiest than other changes of lifestyles. Taking oral medicine in DM2 is simpler because its effect is almost immediate and do not require much time or effort to take place, on the other hand, learn to know your body, change eating habits and especially change exercise habits, requires more time, effort and volitional control, while reinforcing ef- fects that could motivate these behaviors are usually perceived at long-term and in some cases, they do not become tangible because they are preventive, this makes that the immediate cost-benefit assessment, do not encourage change in that kind of behavior. According to the processes by which self-efficacy beliefs regulate human behavior (cognitive, motivational, emotional and choice) this study was interested in the possible relation- ship between self-efficacy and person’s coping strategies to face with his disease situation, in this regard we see that the total SE in DM2 correlated with active and self-recreating cop- ing. The active coping refers to search information about the dis- ease and its treatment, follow the doctor’s instructions, express feelings, set goals and implement strategies to achieve them. This type of coping as seen in the sample, is not the most widely used, but is important to encourage it in the population since is directly related with higher frequency of self-care be- haviors and improved health indicators which represent per- son’s behavioral activation (Fisher et al., 2007). To increase the use of active coping, the results suggest study deeper the rela- tions found between active coping and self-efficacy areas where significant correlations were identified (healthy eating, physical activity and risk regulation). Among coping strategies, self-recreation was one of the most used, it refers to allow themselves make more things, self-en- courage, seek personal success and acclaim and try to distract themselves. This type of coping and its relationship with be- haviors that facilitate self-management in DM2 should be fur- ther analyzed, because if used properly, self-recreation focused in behaviors with which is significant correlated, such as phy- sical activity, risk monitoring signals and even personal well- being and self-esteem, may help DM2 management. Moreover, support for religious faith, is a type of coping ex- pected in a sample from a population in which at least 88% reported being Catholic (National Institute of Statistics, Geog- raphy and Informatic, 2005). This type of coping, only corre- lated with SE in oral medication, this could suggest that people put the responsibility of their well-being outside them (external locus of control), like in the medicine or in god, and do not feel able to change lifestyle habits and get big improvement by themselves, so they may seek solace in religion, accept illness as a destination and even seek in it some sense. This kind of coping could be fine for terminal illnesses, but for DM2 other strategies of coping should be expected and promoted. Finally depressive coping was the less frequent in the sample, but even it had no significant correlation with SE in any of its domains, it is important to note that if there were some, it would have negative tendency, this affirmation is based on other studies in which this correlations were found being sig- nificant (González-Celis, 2002; Ortiz, Ortiz, Gatica, & Gomez, 2011), an alternative explanation is that normally high presence of depression in the elderlies (Barua, Ghosh, Karl, & Basilio, 2011) could be darkening a possible relation between depres- sion coping strategies and self-efficacy in DM2 management, that possible could be found if replicate this study with different group ages. Conclusion As the type of coping that a person adopts to manage their DM, relate to the control over their illness, coping type selec- tion process is important to understand. Self-efficacy in the management of the disease have sense if improves the per- formance of behaviors that potentiate health and minimize risks. As expected, findings of this study showed correlation be- tween self-efficacy beliefs and problem focus coping (active, self-recreation) and almost no correlation was found between self-efficacy with emotion focus coping (depressive and reli- gious faith). This results and the underlying framework, suggest that the beliefs seniors have on their ability to perform certain behaviors, relate to the strategies of coping they select. Since the conducts would be held as long as the person believes hav- ing the necessary for carry them out successfully, the coping strategies that optimize these behaviors are recommended to be strengthened through self-efficacy beliefs (Krein, Heisler, Piette, Butchart, & Kerr, 2007). Even evidence seems to indicate that self-efficacy could im- prove coping choice, this relation has to be deeper studied, in one hand it is probable that the relation is bidirectional, on the other hand coping strategies selections could be influenced by many others factors, one example is that Mexican culture could have an external locus of control that could explain why self- efficacy in oral medication is related with religious faith coping but not with active coping. This study had some limitations, such as, cross-sectional de- sign, the heterogeneity of the sample related to time of diagno- sis, education level and particularities which could not be as- sessed as religion believes, spirituality, and locus of control, nevertheless, considering that diabetes is a disease which man- agement largely depends on patients involvement, it is neces- sary to make studies starting from the results found here as a point of departure for the subject. Limitations invite researchers to replicate this study with samples of different ages, religions, Copyright © 2013 SciRes. 42  M. HATTORI-HARA, A. L. GONZÁLEZ-CELIS cultures, countries, more measures and with longitudinal de- signs. Acknowledgements This paper is product of an investigation sponsored by CONACYT, through a grant scholarship (223214) for the Psy- chology PhD studies of the first author under the guidance of the second. REFERENCES American Association of Diabetes Educator (2011a). AADE 7™ self- care behaviors American Association of Diabetes Educators (AADE) position statement. http://www.diabeteseducator.org/export/sites/aade/_resources/pdf/res earch/AADE7_Position_Statement_version_2011_update.pdf American Association of Diabetes Educator (2011b). Guidelines for the practice of diabetes education. http://www.diabeteseducator.org/ American Diabetes Association (2001). Diabetes and the elderly. Cli- nical Diabetes, 19, 176. doi:10.2337/diaclin.19.4.176 Annesi, J. J. (2011). Moderation of fatigue and stress in the carry-over of self-regulation and self-efficacy for exercise to self-regulation and self-efficacy for managed eating. Psyc ho l o gy , 2, 694-699. doi:10.4236/psych.2011.27106 Bandura, A. (1997). Self-efficacy: The exercise of eontrol. Freeman and Company. Bandura, A. (Ed.) (1999). Auto-eficacia: Cómo afrontamos los cambios de la sociedad actual? España: Desclée De Brouwer. Bandura, A. (2004). The growing primacy of perceive efficacy in hu- man self-development, adaptation and change. In M. Salanova, R. Graw, I. Martinez, E. Cifre, S. Llorens, & M. Garcia-Renedo (Eds.), Nuevos horizontes en la investigación sobre la auto-eficacia. Cas- telló de la Plana: Universitat Jaume. Barua, A., Gosh, M. K., Karl, N., & Basilio, M. A. (2011). Prevalence of depressive disorders in the elderly. Annals of Saudi Medicine, 31, 640-624. doi:10.4103/0256-4947.87100 Bazo, M., Garcia, S., Maiztegui, O., & Martinez, P. (1999). Envejeci- miento y sociedad: Una perspectiva internacional. Madrid: Médica Panamericana. Carver, C. S, Scheier, M. F., & Weintraub, J. K. (1989). Assessing cop- ing strategies: A theoretically based approach. Journal of Personality and Social Psychology, 56, 267-283. doi:10.1037/0022-3514.56.2.267 Cornell, S., & Briggs, S. (2004). Newer treatment strategies for the management of type 2 diabetes mellitus. Journal of Pharmacy Prac- tice, 17, 49-54. doi:10.1177/0897190003261308 Del Castillo, A. (2010). Apoyo social, síntomas depresivos, auto-efica- cia y bienestar psicológico en pacientes con diabetes tipo 2. Ph.D. Thesis, México DF: Facultad de Psicología, UNAM. Duangdao, K. M., & Roesch, S. C. (2008). Coping with diabetes in adulthood: A meta-analysis. Journal of Behavior Medicine, 31, 291- 300. doi:10.1007/s10865-008-9155-6 Ellis, D., Naar-King, S., Frey, M., Templin, T., Rowland, M., & Greger, N. (2004). Use of multisystemic therapy to improve regimen adher- ence among adolescents with type1 diabetes in poor metabolic con- trol: A pilot investigation. Journal of Clinical Psychology in Medical Settings, 11, 1746-1747. doi:10.1023/B:JOCS.0000045351.98563.4d Ephrem, F. (1986). A classification system of cognitive coping strate- gies for pain. Pain, 26, 141-151. doi:10.1016/0304-3959(86)90070-9 Fisher, E., Thorpe, C., McEvoy, B., & DeVellis, R. (2007). Healthy coping, negative emotions, and diabetes management: A systematic review and appraisal. The Diabetes Educator, 33, 1080-1103. doi:10.1177/0145721707309808 Froján M., & Rubio, R. (2004). Análisis discriminante de la adhesión al tratamiento en la diabetes mellitus insulinodependiente. Psicothema, 16, 548-554. Gillibrand, R., & Stevenson, J. (2006). The extended health belief model applied to the experience of diabetes in young people. British Journal of Health Psychology, 11, 155-169. doi:10.1348/135910705X39485 González-Celis, A. L. (2002). Efectos de intervención de un programa de promoción a la salud sobre la calidad de vida en ancianos. Tesis de Doctorado en Psicología, México DF: Facultad de Psicología, UNAM. González-Celis, A. L. (2005). Cómo mejorarla calidad de vida y el bie- nestar subjetivo de los ancianos? In: L. Garduño, B. Salinas, & M. Rojas, (Eds.), Calidad de Vida y bienestar subjetivo en México (pp. 259-294). México: Plaza y Valdéz. Gutiérrez, L. (2004). La salud del anciano en México y la nueva epidemiología del envejecimiento. http://www.conapo.gob.mx/publicaciones/2004/sdm26.pdf Haire, D. (1996). Management of diabetes mellitus. Maryland Heights: Mosby. Horton, E., Cefalu, W., Haines, S., & Siminerio, L. (2008). Multidisci- plinary interventions: Mapping new horizonts in diabetes care. The Diabetes Educator, 34, 78S-89S. doi:10.1177/0145721708321148 International Diabetes Federation (2012). IDF diabetes atlas. http://www.idf.org/diabetesatlas/5e/the-global-burden Kanbara, S., Taniguchi, H., Sakaue, M., Wang, D. H., Takaki, J., Ya- jima, Y. et al. (2008). Social support, self-efficacy and psychological stress responses among outpatients with diabetes in Yogyakarta, In- donesia. Diabetes Res e a r c h a nd C l i nical Practice, 80, 56-62. doi:10.1016/j.diabres.2007.12.015 Katz, J., Ritvo, P., Irvine, M. J., & Jackson, M. (1996). Coping with cronic pain. In M. Zeidner, & N. Endler (Eds.), Handbook of coping. Hoboken: John Wiley & Sons. Krein, S., Heisler, M., Piette, J., Butchart, A., & Kerr, E. (2007). Over- coming the influence of chronic pain on older patients’ difficulty with recommended self-management activities. The Gerontologist, 47, 61-68. doi:10.1093/geront/47.1.61 Latin American Diabetes Association (2008). Guía de diagnóstico, control y tratamiento de la Diabetes Mellitus tipo 2. Washington: Organización Panamericana de la Salud. Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal and coping. New York: Springer Lazarus, R. S., & Folkman, S. (1991). Estrés y procesos cognitivos. México: Martínez Roca. Lazarus, R. S. (1993). Coping theory and research: Past, present and future. Psychoso m a t i c M e dicine, 55, 234-247. Lazarus, R. S. (2000). Estrés y emoción. Manejo e implicaciones en nuestra salud. Bilbao: Desclée de Brouwer. Monfort, E., & Tréhel, G. (2012). Classification of coping styles in a population of aging veterans. Annales Médico-Psychologiques, Re- vue Psychiatrique, 9, 636-641. doi:10.1016/j.amp.2012.05.017 Muthny, V. (n.d.). Freiburger frageboben zur krankheitsverarbeitung. http://www.testzentrale.del/?mod=detail&id=550 National Institute of Statistics, Geography and Informatic [INEGI] (2005). La diversidad religiosa en México. INEGI: Aguascalientes. National Population Council (2010). De la población en México 2005- 2050. Datos nacionales. http://www.conapo.gob.mx/index.php?option=com_content&view=a rticle&id=36&Itemid=234 National System of Health Information (2005). Defunciones y tasa de mortalidad general por año de registro 2000-2005. http://www.sinais.salud.gob.mx/mortalidad/index.html Olaiz, G., Rojas, R., Barquera, S., Shamah, T., Aguilar, C., Cravioto, P. et al. (2003). Encuesta nacional de salud 2000. Tomo 2. La salud de los adultos. México: Instituto Nacional de Salud Pública. Ortiz, M., Ortiz, E., Gatica, A., & Gómez, D. (2011). Factores psico- sociales asociados a la adherencia al tratamiento de la diabetes mel- litus tipo 2. Terapia Psicológica, Sociedad Chilena de Psicología Clínica, 29, 5-11. doi:10.4067/S0718-48082011000100001 Oviedo-Gómez, M. (2007). Modelo multidimensional del automanejo conductual de la diabetes tipo 2 basado en la participación familiar. Ph.D. Thesis, Universidad Nacional Autónoma de México, Facultad de Psicología, Ciudad Universitaria. Pérez, P. (2003). Guía para el paciente y el educador en diabetes. Copyright © 2013 SciRes. 43  M. HATTORI-HARA, A. L. GONZÁLEZ-CELIS Copyright © 2013 SciRes. 44 México: FES Iztacala. Riveros, A., Cortazar-Palapa, J., Alcazar, F., & Sánchez-Sosa, J. (2005). Efectos de una intervención cognitivo-conductual en la calidad de vida, ansiedad, depresión y condición médica de pacientes diabéticos e hipertensos esenciales. International Journal of Clinical and Health Psychology, 5, 445-462. http://www.aepc.es/ijchp/articulos_pdf/ijchp-153.pdf Romero-Martínez, M., Shamah-Levy, T., Franco-Núñez, A., Villal- pando, S., Cuevas-Nasu, Rivera-Dommarco, J., & Gutiérrez, J. P. (2012). Encuesta nacional de salud y nutrición 2012. Base de datos del cuestionario individual: Adultos de 20 o más años de edad SPSS. http://ensanut.insp.mx/basesdoctos.php#.UQndDmf-ibE Rose, M., Hildebrandt, M., Fliege, H., Klapp, B. F., & Schirop, T. (2002). The network of psychological variables in patients with dia- betes and their importance for quality of life and metabolic control. Diabetes Care, 25, 35-42. doi:10.2337/diacare.25.1.35 Samuel-Hodge, C. D., Watkins, D. C., Rowell, K. L., & Hooten E. G. (2008). Coping styles, well-being, and self-care behaviors among Af- rican Americans with type 2 diabetes. Diabetes Educator, 34, 501- 510. doi:10.1177/0145721708316946 Schokker, M. C., Links, T. P., Bouma, J., Keers, J. C., Sanderman, R. et al. (2011). The role of overprotection by partner in coping with dia- betes: A moderate mediation model. Psychology Health, 26 , 95-111. doi:10.1080/08870440903342325 Schwarzer, R., & Schwarzer, C. (1996). A critical survey of coping instruments. In M. Zeidner, & N. Endler (Eds.), Handbook of coping. Hoboken: John Wiley & Sons. Steed, L., Lankester, J., Barnard, M., Earle, K., Hurel, S., & Newman, S. (2005). Evaluation of the UCL Diabetes self-management pro- gramme (UCL-DSMP): A randomized control trial. Journal of He alth Psychology, 10, 261-276. doi:10.1177/1359105305049775 Thoolen, B., Ridder, D., Bensing, J., Gorter, K., & Rutten, G. (2008). Beyond good intentions: The development and evaluation of a proac- tive self-management course for patients recently diagnosed with type 2 diabetes. Health Education Research, 23, 53-61. doi:10.1093/her/cyl160 United Nations (2002). World population aging: 1950-2050. http://www.un.org/esa/population/publications/worldageing1950205 0 Villalpando, S., Cruz, V., Rojas, R., Shamah-Levy, T., Ávila, M. A., Gaona, B. et al. (2010). Prevalence and distribution of type 2 diabe- tes mellitus in Mexican adult population. A probabilistic survey. Salud Pública de México, 52, 19-26. doi:10.1590/S0036-36342010000700005 Wagner, J., & Tennen, H. (2007). Coping with diabetes: Psychological determinants of diabetes outcomes. In E. Martz, & H. Livneh (Eds). Coping with chronic illness and disability. Theoretical, empirical, and clinical aspects. New York: Springer. doi:10.1007/978-0-387-48670-3_11 Zúñiga, E., García, J., & Partida V. (2004). Mortalidad de la población de 60 años o más. http://www.conapo.gob.mx/publicaciones/2004/sdm27.pdf
|