M. C. Provero et al. / Open Journal of Pediatrics 3 (2013) 133-138
136
nasal smear showed an eosinophilic infiltration allowing
us the diagnosis of NARES. This indicates that the
treatment with systemic antibiotic was not able to control
the recurrent rhinosinusitis because of these allergic cells
[11] and nasal steroids improved the situation.
This observation is in favor of the specificity of the
NARES diagnosis, which should not be considered as
due to allergy towards an unknown allergen, but a true
novel entity.
The nasal cytogram helped us in the diagnosis of AR.
In 9/59 asymptomatic children with AR to perennial
allergens we expected to see a normal exam, but we
found neutrophils and eosinophils, documenting the
presence of “minimal persistent inflammation” [7].
The nasal cytogram of 38/59 children with AR (symp-
toms and positivity to SPT and/or RAST) showed eosi-
nophilia, confirming the isolated allergic form in these
patients. In 21/59 allergic patients the nasal smear was
normal. This confirmed the effectiveness of the treatment,
in particular in those under SLIT. On the other hand, a
significant proportion of allergic children (11/59) showed
also bacteria. In the absence of this result an ineffective-
ness of the antiallergic therapy would have been sus-
pected and it would not have been added the correct
therapy with antibiotic.
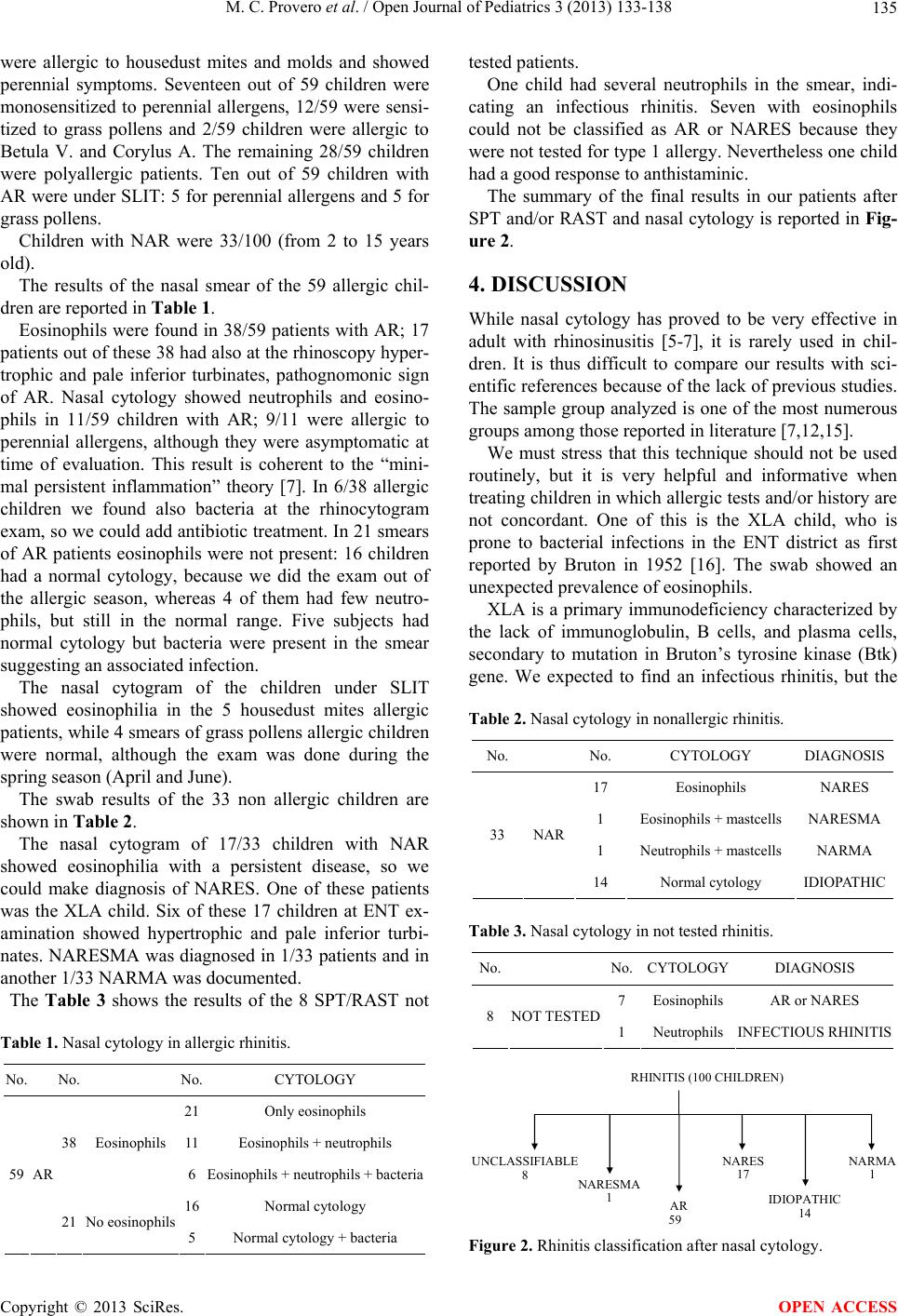
Using nasal cytology we could identify cellular rhinitis
(17 NARES, 1 NARESMA and 1 NARMA) in our group
of patients, who without this exam would have remained
with no specific diagnosis and treatment.
Despite our intent was to design nasal cytology just for
allergic patients, it allowed us a specific diagnosis even
in nonallergic ones.
5. CONCLUSIONS
Nasal cytology is useful both from the pathophysiologi-
cal and clinical point of view to better understand the
disease and to follow especially children in which aller-
gic test and/or history are not concordant.
The advantages of nasal cytology are different: the
ease of performance, the noninvasiveness allowing repe-
tition and the low cost.
It is useful to follow the disease during medical treat-
ment by periodic cytologic controls, showing, for exam-
ple, a significant reduction of inflammatory cells or the
disappearance of bacteria.
When considering an allergic child with SPT positivity,
the etiology of an existent rhinitis could not be assumed
to be certainly allergic: only the nasal cytology can di-
rectly confirm such etiology by showing the presence of
an eosinophilic infiltrate. On the other side, the allergic
child is prone to long lasting bacterial infection and even
in this case the nasal cytology can show the existence of
a secondary bacterial infection (neutrophilic infiltrate ±
bacteria).
The effectiveness of the SLIT could be documented by
this technique allowing us to show the disappearance of
the eosinophilic infiltrate. The compliance to the SLIT
could also be assessed by nasal cytology.
It has provided an important contributution to identi-
fication of new pathological entities, such as the nonal-
lergic eosinophilic rhinitis (NARES) or mast cell medi-
ated nasal inflammation (NARESMA).
Despite the proven usefulness of nasal cytology, we
suggest to use this technique not routinely, but mainly
for selected patients or for scientific survey.
6. ACKNOWLEDGEMENTS
We thank the technicians and colleagues of the ENT and pediatric
allergy clinics for the kind and effective collaboration.
REFERENCES
[1] Bogaerts, P. and Clement, P. (1981) The diagnostic value
of a cytogram in rhinopathology. Rhinology, 19, 203-208.
[2] Hu, T. and Desai, J.P. (2004) Soft-tissue material proper-
ties under large deformation: Strain rate effect. Proceed-
ings of the 26th Annual International Conference of the
IEEE EMBS, San Francisco, 1-5 September 2004, 2758-
2761.
[3] Malmberg, H. and Holopainen, E. (1979) Nasal smear as
a screening test for immediate-type nasal allergy. Allergy,
34, 331-337. doi:10.1111/j.1398-9995.1979.tb04375.x
[4] Cohen, G.A, Macpherson, G.A, Golembersky, H.E, Ja-
lowayski, A.A. and O’Connor, R.D. (1985) Normal nasal
cytology in infancy. Annals of Allergy, 54, 112-114.
[5] Glück, U., Schütz, R. and Gebbers, J.O. (2003) Cytopa-
thology of the nasal mucosa in chronic exposure to diesel
engine emission: A five-year survey of Swiss customs of-
ficers. Environmental Health Perspectives, 111, 925-929.
doi:10.1289/ehp.4401
[6] Boysen, M., Zadig, E. and Digerne, V. (1990) Nasal mu-
cosa in workers exposed to formaldehyde: A pilot study.
British Journal of Industrial Medicine, 47, 116-121.
[7] Gelardi, M., Fiorella, M.L, Leo, G. and Incorvaia C.
(2007) Cytology in the diagnosis of rhinosinusitis. Pedi-
atric Allergy and Immunology, 18, 50-52.
doi:10.1111/j.1399-3038.2007.00634.x
[8] Gelardi, M., Cassano, P., Cassano, M. and Fiorella, M.L.
(2003) Nasal cytology: Description of a hyperchromatic
supranuclear stria as a possible marker for the anatomical
and functional integrity of the ciliated cell. American
Journal of Rhinology, 17, 263-268.
[9] Gelardi, M., Incorvaia, C., Passalacqua, G., Quaranta, N.
and Frati, F. (2011) The classification of allergic rhinitis
and its cytological correlate. Allergy, 66, 1624-1625.
doi:10.1111/j.1398-9995.2011.02741.x
[10] Bickmore, J.T. and Marshall, M.L. (1976) Cytology of
nasal secretions: Further diagnostic help. Laryngoscope,
86, 516-523. doi:10.1288/00005537-197604000-00007
Copyright © 2013 SciRes. OPEN ACCESS