T. HAQUE ET AL.
Copyright © 2013 SciRes. OJRD
67
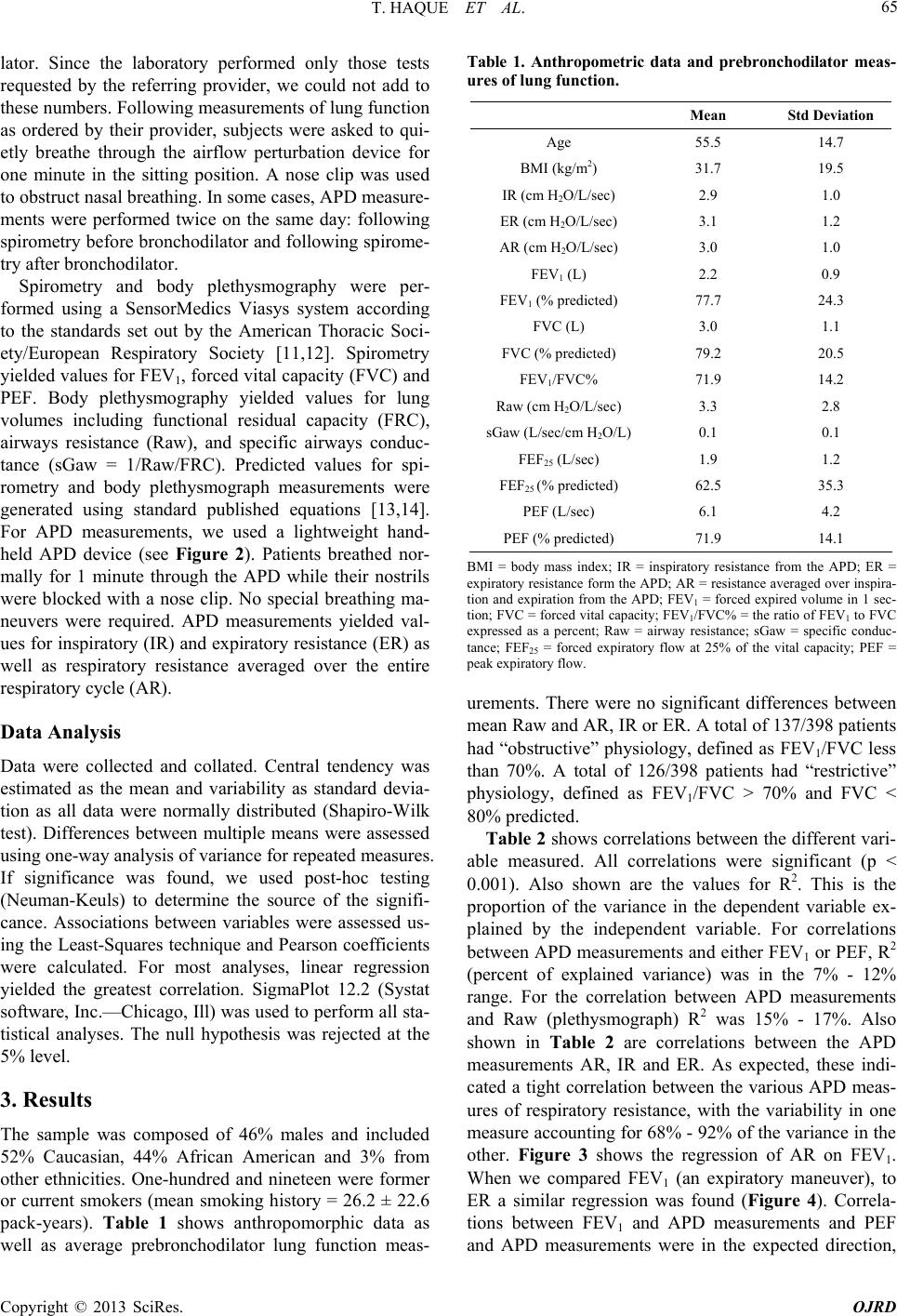
tween FEV1 and PEF, that are forced expiratory maneu-
vers, was excellent, with some 2/3 of the variance in one
explained by the other.
It is important to bear in mind that the various meas-
ures of pulmonary function actually measure different
aspects of respiratory mechanics. FEV1 and PEF are cer-
tainly responsive to changes in airways resistance; how-
ever, they are also very dependent on patient effort. Raw,
measured in the body plethysmograph, is sensitive to
changes in flow-resistance of the airways, but excludes
lung and chest wall tissue resistance. The APD measures
total respiratory resistance, and includes a large compo-
nent of upper airways resistance (see [8]). The most
practical use for the APD would likely be to follow pa-
tients with lung disease serially at home given the ease of
use and low cost of this device. We had hoped that the
measurement of serial function before and after bron-
chodilator would simulate serial measurements for stan-
dard spirometry compared with APD. Unfortunately, few
patients had bronchodilator studies ordered, and the
overall change in FEV1 with bronchodilator was small
(approximately 100 cc). Finally, in a recent study [15],
the intrasubject variability of APD measurements was
assessed. It was found that the largest portion of the
variability of measurements was in fact due to changes
within the subject and not to changes within the APD,
strengthening our argument that the device would be
most useful for serial measurements in patients with lung
disease.
In sum, there are significant correlations between APD
derived measures of respiratory resistance and measures
derived from standard pulmonary function testing. The
variance explained was less than that between commonly
used measures of pulmonary function. Studies should be
directed at the evaluation of efficacy of serial measure-
ments over time in patients with respiratory disease.
REFERENCES
[1] A. M. Dubois, S. Y. Botelho and J. H. Comroe Jr., “A
New Method for Measuring Airway Resistance in Man
Using a Body Plethysmograph: Values in Normal Sub-
jects and in Patients with Respiratory Disease,” Journal
of Clinical Investigation, Vol. 35, No. 3, 1956, pp. 327-
335. doi:10.1172/JCI103282
[2] K. Von Neergard and K. Wirz, “Die Messimg. Der
Stromungwiderstande in den Atemwegen des Menschen
Insbespondere bie Asthma und Emphysema,” Zeitschrift
fur Klinische Medizine, Vol. 105, 1927, pp. 51-82.
[3] A. M. DuBois, A. W. Brody, D. H. Lewis and B. F. Bur-
gess, “Oscillation Mechanics of Lungs and Chest in Man,”
Journal of Applied Physiology, Vol. 8, No. 6, 1956, pp.
587-594.
[4] H. J. Smith, P. Reinhold and M. D. Goldman, “Forced
Oscillation Technique and Impulse Oscillometry,” Euro-
pean Respiratory Journal, Vol. 31, 2005, pp. 72-105.
[5] A. T. Johnson, C.-S. Lin and J. N. Hochheimer, “Airflow
Perturbation Device for Measuring Airway Resistance of
Humans and Animals,” IEEE Transactions on Biomedical
Engineering, Vol. 31, No. 9, 1984, pp. 622-626.
doi:10.1109/TBME.1984.325306
[6] C. G. Lausted and A. T. Johnson, “Airflow Perturbation
Device for Measureing Human Respiratory Resistance,”
Proceedings of the IEEE 24th Annual Northeast Confer-
ence, 9-10 April 1998, pp. 97-99.
[7] A. T. Johnson and M. S. Sahota, “Validation of Airflow
Perturbation Device Resistance Measurements in Excised
Sheep Lungs,” Physiological Measurement, Vol. 25, No.
5, 2004, pp. 679-690. doi:10.1088/0967-3334/25/3/008
[8] D. C. Coursey, S. M. Scharf and A. T. Johnson, “Com-
paring Pulmonary Resistance Measured with an Eso-
phageal Balloon to Resistance and Measurements with an
Airflow Perturbation Device,” Physiological Measure-
ment, Vol. 31, No. 7, 2010, pp. 921-934.
doi:10.1088/0967-3334/31/7/004
[9] D. C. Coursey, S. M. Scharf and A. T. Johnson, “Com-
parison of the Expiratory Isovolume Pressure Flow Rela-
tionship Generated with Stop-Flow and Esophageal Bal-
loon Methods,” Respiratory Care, Vol. 56, No. 7, 2011,
pp. 969-975. doi:10.4187/respcare.01037
[10] N. K. Silverman, A. T. Johnson, W. H. Scott and F. C.
Koh, “Exercise-Induced Respiratory Resistance Changes
as Measured with the Airflow Perturbation Device,”
Physiological Measurement, Vol. 26, No. 1, 2005, pp. 29-
38. doi:10.1088/0967-3334/26/1/003
[11] M. R. Miller, J. Hankinson, V. Brusasco, F. Burgos, R.
Casaburi, A. Coates, R. Crapo, P. Enright, C. P. M. van
der Grinten, P. Gustafsson, R. Jensen, D. C. Johnson, N.
MacIntyre, R. McKay, D. Navajas, O. F. Pedersen, R.
Pellegrino, G. Viegi and J. Wanger, “Standardisation of
Lung Function Testing: Standardisation of Spirometry,”
European Respiratory Journal, Vol. 26, No. 2, 2005, pp.
319-338. doi:10.1183/09031936.05.00034805
[12] J. Wanger, J. L. Clausen, A. Coates, O. F. Pedersen, V.
Brusasco, F. Burgos, R. Casaburi, R. Crapo, P. Enright, C.
P. M. van der Grinten, P. Gustafsson, J. Hankinson, R.
Jensen, D. Johnson, N. MacIntyre, R. McKay, M. R.
Miller, D. Navajas, R. Pellegrino and G. Viegi, “Stan-
dardisation of the Measurement of Lung Volumes,”
European Respiratory Journal, Vol. 26, No. 3, 2005, pp.
511-522. doi:10.1183/09031936.05.00035005
[13] J. F. Morris, A. Koski and L. C. Johnson, “Spirometric
Standards for Healthy Non-Smoking Adults,” American
Review of Respiratory Disease, Vol. 103, 1971, pp. 57-
67.
[14] R. O. Crapo, A. H. Morris, P. D. Clayton and C. R. Nixon,
“Lung Volumes in Healthy Nonsmoking Adults,” Bulletin
Européen de Physiopathologie Respiratoire, Vol. 18, No.
3, 1982, pp. 419-425.
[15] A. T. Johnson, S. C. Jones, J. J. Pan and J. Vosoughi,
“Variation of Respiratory Resistance Suggests Optimiza-
tion of Airway Caliber,” IEEE Transactions on Biomedi-
cal Engineering, Vol. 59, No. 8, 2012, pp. 2355-2361.
doi:10.1109/TBME.2012.2204055