Paper Menu >>
Journal Menu >>
 S ur g ical Scie n doi:10.4236/ss. 2 Copyright © 2 0 Per c 1 D e 2 D Abstract Hydatid cys t most freque n case of the r e with the op a with a thin p ultrasonogra p later during was observe d ment for the protection n e comparing t o Keywords: H 1. Introdu c Hydatid cysts b y a parasite common in t h such as Asia , and South E u high and they are common quent for the c The most f and lungs [3, 4 b one [6], ki d located cysts tients. Although t treated with t medically, th e ment for the generally sur g though the m cially used fo p referred for n ce, 2010, 1, 5 2 010.12012 Pu b 0 10 SciRes. c utane o Seze n e partment of P D epartment of R Rece i t s are slowly n t locations o e nal hydatid a que tomogra p p eriphery an d p hy we perf o the ultrason o d that the cy s kidney loca t e eded renal p o the previou H ydatid Cyst, c tion are slowly e n named Echin o h e areas that , Australia, S o u rope [1]. Th e are seen in th e at every age, c hildren that a d f requent locati 4 ]. They can b d ney [1,7] an d are with a fr e t he liver and t he usage of a e re is not any kidney locat e g ical and in m ethod of per c r liver locate d the renal hy d 5 6-59 b lished Online O o us Asp i Ultr a n Ozkisacik 1 , P ediatric Surg e R adiodiagnos t i ved August 9, enlarging c y o f the cysts a r cys t that we p hy a cystic d a size of 1 2 o rmed (Punc t o graphic exa m s t was comp l t ed hydatid c p arenchyma i s cases. Echinococc u n larging cysti c o coccus gran u deal with an i o uth America , e incidence in e 4.4 of 100.0 0 however the y d ults [2]. i ons of the cy s b e rarely loca t d pancreas [8, e quency of 2 - lung locate d a lbendazole a n data about th e e d cysts and t selective cas e c utaneous asp d hydatid cyst s d atid cysts un d O ctobe r 2010 ( h i ration a sonog r , Mesut Yaz i e ry, Adnan Me t ic, Adnan Me n E-mail: s o z 2010; revise d y stic masses c r e liver and l u used the per c mass was d e 2 × 8 plain c t ure, aspirati o m ination the r l etely collap s c ysts which a n order not t o u s Granulos u c masses caus e u losus. They a r i mal husband r , the Near E a Turkey is ve r 0 0 people. Th e y are more f r e s ts are liver [ 3 t ed in brain [ 5 9]. The kidn e - 3 % of all p a d cysts can b n d mebendazo l e medical tre a t he treatment e s [10,11]. A iration is esp e s , it can also b d er the proph y h ttp://www.Sci R of a R e r aphic G i ci 1 , Harun G e nderes Unive r n deres Univer s z kisacik@adu. e d August 9, 20 1 c aused by a p u ngs. They c a c utaneous as p e tected in the c ontour obse r o n, injection , r e was no fl u s ed. We thin k a re not relate o have a los s u s, Percutane o e d r e r y a st r y e y e - 3 ] 5 ], e y a - b e le a t- is A l- e - b e y - laxis [ 1 that w e 1.1. C a The 9 domin a in the l size o f referre d The and no datid c y functi o treatm e three m sonogr a right k i cyst a n tem. W mass w egzoti f a thin p R P.org/journal/s s e nal H y G uida n G ursoy 1 , Ku t r sity Faculty o f s ity Faculty o f e du.t r 1 0; accepted A p arasite nam e a n be rarely l p iration met h right kidne y r ving septati o , reaspiratio n u id collectio n k that this ca n d to the coll e s of tissue an d o us Aspirati o 1 2]. We prese n e used the per c a se years old ma l a l fullness and l iver was diag n f 12 × 8 cm. U d to our clinic . abdominal ex a mass was pa l y st was Ig G o ns, urinary m e nt was start e m onths the p a a phy (US) (F i i dney had a c o n d there was g W ith the opaq u w as detected i f ic located, pr e p eriphery and a s ) y datid C n ce t si Koseoglu f Medicine, A y f Medicine, Ay d A ugust 9, 2010 e d Echinoco c l ocated in ki d h od. The 9 y e y that was pa r o ns in it. Wi t n ) (PAIR) pr o n in the cyst n be an alter n e ctive syste m d not to hav e n n t our case o f c utaneous aspi r l e patient ha d with ultrason o n osed that wa s U pon the dia g . a mination of t l pated there. T 1/2500, the te s m icroscopy ar e e d lasting fo r a tient was ex a ig ure 1) and i t o mpressed app g rade I ectasi a u e tomograph y i n the right k e ssuring the r e a size of 12 × 8 C yst wi t 2 y din, Turkey d in, Turkey c cus granulo s d ney. We pre s e ars old male r tly egzotific t h the accor d o cedure. Six or echogenit y n ative medic m and for the e a complica t f the renal hyd r ation method . d the complai n o graphy a hy d s a plain cont o g nosis the pat t he patient wa s T he serology o f s ts of liver an d e normal. Alb e r three mont h a mined with t h t was detecte d earance beca u a in the collec t y (Figure 2) k idney that w a e nal parenchy m 8 plain contou r SS t h s us. The s ent our patient, located d ance of months y and it al treat- case of t ion risk atid cyst . n t of ab- d atid cyst o ur at the ient was s normal f the hy- d kidney e ndazole h s. After h e ult r a- d that the u se of the t ive sys- a cystic a s partly m a, with r observ- 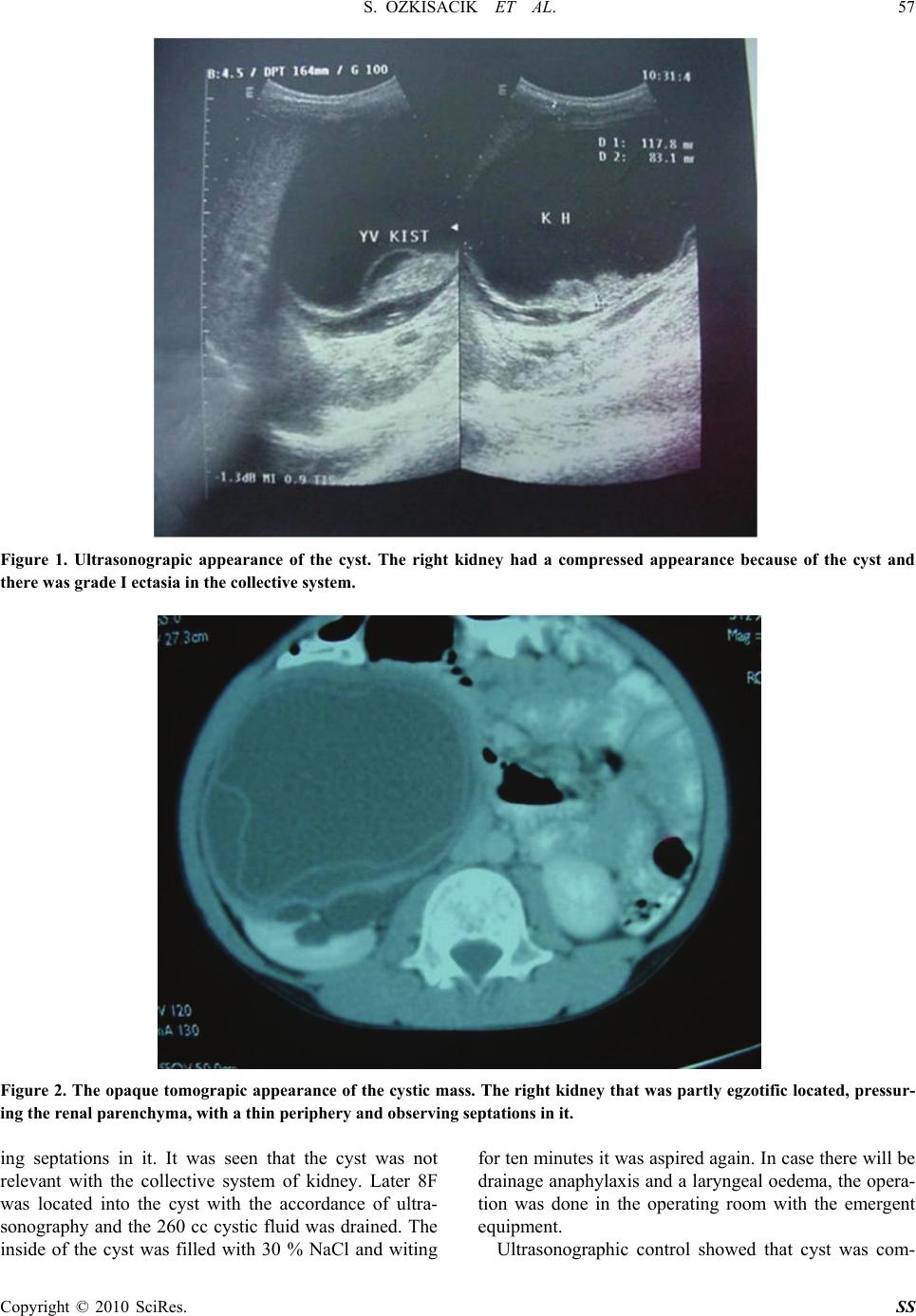 S. OZKISACIK ET AL. 57 Copyright © 2010 SciRes. SS Figure 1. Ultrasonograpic appearance of the cyst. The right kidney had a compressed appearance because of the cyst and there was grade I ectasia in the collective system. Figure 2. The opaque tomograpic appearance of the cystic mass. The right kidney that was partly egzotific located, pressur- ing the renal parenchyma, with a thin periphery and observing septations in it. ing septations in it. It was seen that the cyst was not relevant with the collective system of kidney. Later 8F was located into the cyst with the accordance of ultra- sonography and the 260 cc cystic fluid was drained. The inside of the cyst was filled with 30 % NaCl and witing for ten minutes it was aspired again. In case there will be drainage anaphylaxis and a laryngeal oedema, the opera- tion was done in the operating room with the emergent equipment. Ultrasonographic control showed that cyst was com-  S. OZKISACIK ET AL. Copyright © 2010 SciRes. SS 58 pletely drained and cystic cavity was totally collapsed. Albendazole treatment was continued for three months following intervention. Six months postintervention con- trol revealed no complication. The conventional treatment of hydatid disease is sur- gical. For hydatid cyst of the kidney, enucleation of the cyst, cystectomy, partial or total nephrectomy can be performed related to its localization. As in our case, in selected cases with hydatic cyst, percutaneous drainage may be utilized with the major aim of preservation of renal parenchyma. Postoperative with the ultrasona- graphic examination on the first day, the drained was stopped and the patient was discharged from the hospital after it was seen that the cyst was drained completely and the periphery of the cyst was shrivelled. Postoperative the prophylaxis was done for a month. Six months later during the ultrasonographic examination there was no fluid collection in the cyst or echogenity and it was ob- served that the cyst was completely collapsed. 2. Discussion EG is a parasite that lives in the intestinal system of the adult infected dogs [13]. The eggs of this parasite are ejected by the small intestine feces and they are swal- lowed by lambs, cattle, goats or humans. The humans can also be swallowed them by means of drinking water and food or by toughing the dogs directly. The capsules of these eggs are opened after they come to the human intestines and the come out larva penetrates to the jeju- num, venous and lymphatic system can be located in any organ [1]. Cysts that are the rarely in kidneys are unique and lo- cate at the cortex kidney [1]. For the renal hydatid cysts the only pathognomonic diagnosis is hydatidore, but they can only be seen if the cyst is related to the collective system and they can be seen in the 5-28% of the patients [10]. The diagnosis for these patients are nonspecific and they are usually the mass in the flank area and the symp- toms depends on its pressure [7,14]. Acute retention of urine and anuria can be rarely seen [1,15]. The treatment for the hydatid cysts on every organ is usually surgical operation [10]. Related to the location and the size of the cyst, the operations can be encuclea- tion, cystectomy [9,10]. Especially for the renal hydatid cysts on the surface, the surgical operation is recom- mended and for the cysts in the parenchyma is recom- mended [9]. However, the loss of parenchyma at differ- ent rates is possible for these patients and this situation make the surgeons to search for an alternative treatment. It is believed to be contraindicated for the hydatid cysts because of the cyst high percutaneous drainage cyst rupture and also anaphylaxic shock progress risk [3]. Prophylaxis cyst material’s being nonantigenic and its having less anaphylaxis risk are very important [12]. Moreover, it is declared that the prophylaxis decreases the tension on the cyst periphery and the risk of its spread. Percutaneous nephrostomy was tried in 1973 by Roylance and his friends, but it could not be used for a long time because of the complications such as acute anaphylaxis, laryngeal oedema, respirator arrest and the spread of hydatid cyst. However, McCorkell examined the injection aspiration for diagnosis of the lungs masses that were hard to diagnosed radiologically declared that three of these masses were hydatid cysts and after the aspiration there would be no problem [16]. Later Mueller used this method for the treatment of a liver located hy- datid cyst and he succeeded [17]. By this method, accor- dance with the ultrasonography and BT a hypertonic saline solution (15% saline solution) was aspired with an injection or a thin catheter and the ingredient was aspired again (Puncture, aspiration, injection, reaspiration) (PAIR). This was repeated until the endocyst was separated. Many authors justify that this method is very effective and safe [3]. Goel and his friends said that the need for nephrectomy was increased for the laparotomy, only one of the four patients needed nephrectomy because of the severe inflection and bleeding. They declared that the four of them would need nephrectomy if these operations were laparotomy [12]. We think that this can be an alternative medical treat- ment for the kidney located hydatid cysts which are not related to the collective system and for the case of pro- tection needed renal parenchyma in order not to have a loss of tissue and not to have a complication risk com- paring to the previous cases. By this method, the posto- parative time of staying in hospital is shorter than before. For laparotomy, the retroperitoneal spread can occur. That’s why; (especially for the prophylaxis) we think that retroperitoneal spread can be neglected con- sidering the possibilities for the percutaneous drainage. 3. References [1] D. A. Kiresi, A. Karabacakoglu, K. Odev and S. Karakose, “Uncommon Locations of Hydatid Cysts,” Acta Radio- logica, Vol. 44, No. 6, 2003, pp. 622-636. [2] D. Doğru, N. Kiper, U. Özçelik, E. Yalçın and A. Göçmen, “Medical Treatment of Pulmonary Hydatid Disease: For Which Child?” Parasitology International, Vol. 54, No. 2, 2005, pp. 135-138. [3] O. Akhan, M. N. Ozmen, A. Dinçer, I. Sayek and A. Göçmen, “Liver Hydatid Disease: Long-Term Results of Percutaneous Treatment,” Radiology, Vol. 198, No. 1, 1996, pp. 259-264. [4] O. Mutaf, A. Arikan, M. Yazici, A. Erdener and G. Ozok, 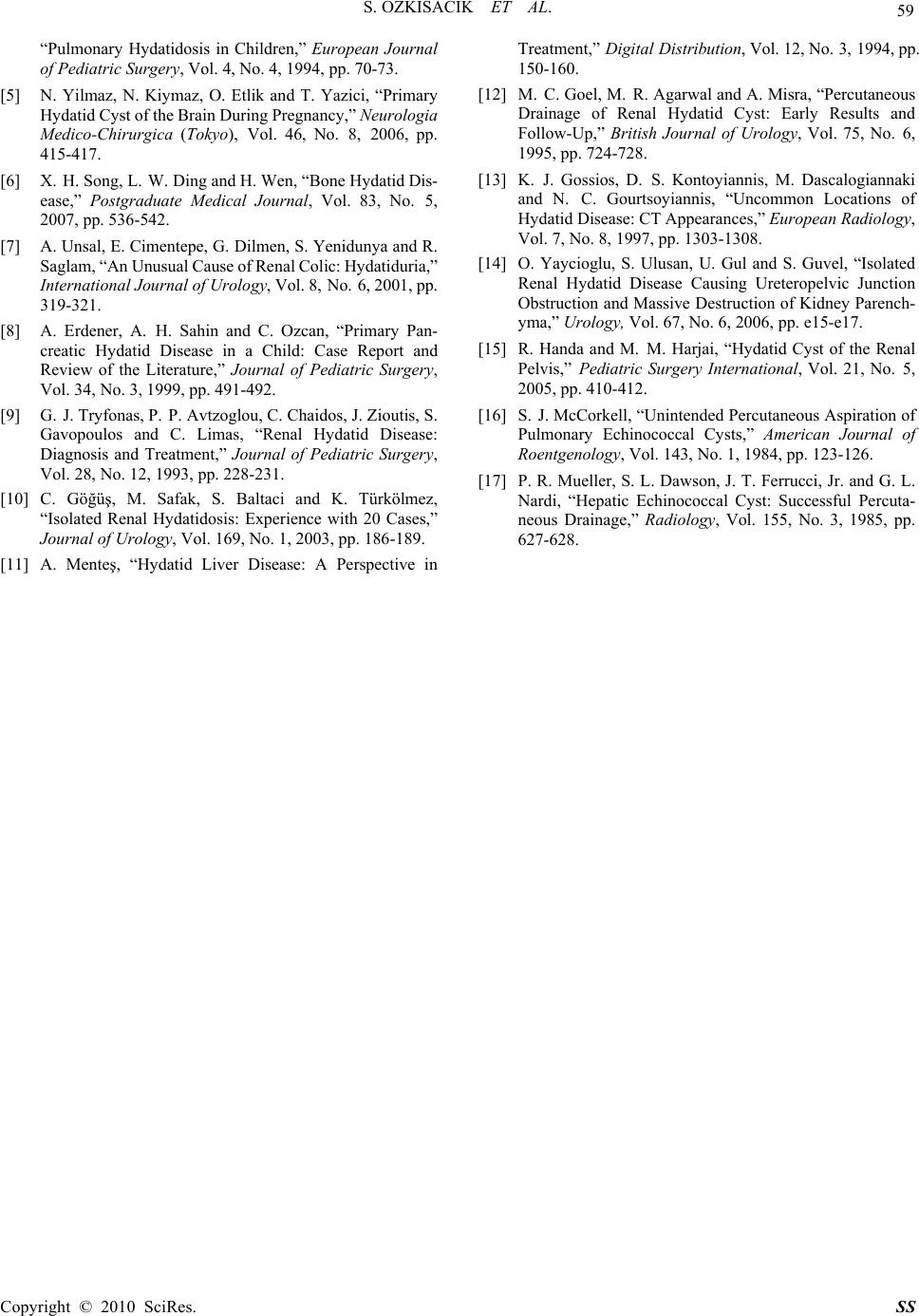 S. OZKISACIK ET AL. Copyright © 2010 SciRes. SS 59 “Pulmonary Hydatidosis in Children,” European Journal of Pediatric Surgery, Vol. 4, No. 4, 1994, pp. 70-73. [5] N. Yilmaz, N. Kiymaz, O. Etlik and T. Yazici, “Primary Hydatid Cyst of the Brain During Pregnancy,” Neurologia Medico-Chirurgica (Tokyo ), Vol. 46, No. 8, 2006, pp. 415-417. [6] X. H. Song, L. W. Ding and H. Wen, “Bone Hydatid Dis- ease,” Postgraduate Medical Journal, Vol. 83, No. 5, 2007, pp. 536-542. [7] A. Unsal, E. Cimentepe, G. Dilmen, S. Yenidunya and R. Saglam, “An Unusual Cause of Renal Colic: Hydatiduria,” International Journal of Urology, Vol. 8, No. 6, 2001, pp. 319-321. [8] A. Erdener, A. H. Sahin and C. Ozcan, “Primary Pan- creatic Hydatid Disease in a Child: Case Report and Review of the Literature,” Journal of Pediatric Surgery, Vol. 34, No. 3, 1999, pp. 491-492. [9] G. J. Tryfonas, P. P. Avtzoglou, C. Chaidos, J. Zioutis, S. Gavopoulos and C. Limas, “Renal Hydatid Disease: Diagnosis and Treatment,” Journal of Pediatric Surgery, Vol. 28, No. 12, 1993, pp. 228-231. [10] C. Göğüş, M. Safak, S. Baltaci and K. Türkölmez, “Isolated Renal Hydatidosis: Experience with 20 Cases,” Journal of Urology, Vol. 169, No. 1, 2003, pp. 186-189. [11] A. Menteş, “Hydatid Liver Disease: A Perspective in Treatment,” Digital Distribution, Vol. 12, No. 3, 1994, pp. 150-160. [12] M. C. Goel, M. R. Agarwal and A. Misra, “Percutaneous Drainage of Renal Hydatid Cyst: Early Results and Follow-Up,” British Journal of Urology, Vol. 75, No. 6, 1995, pp. 724-728. [13] K. J. Gossios, D. S. Kontoyiannis, M. Dascalogiannaki and N. C. Gourtsoyiannis, “Uncommon Locations of Hydatid Disease: CT Appearances,” European Radiology, Vol. 7, No. 8, 1997, pp. 1303-1308. [14] O. Yaycioglu, S. Ulusan, U. Gul and S. Guvel, “Isolated Renal Hydatid Disease Causing Ureteropelvic Junction Obstruction and Massive Destruction of Kidney Parench- yma,” Urology, Vol. 67, No. 6, 2006, pp. e15-e17. [15] R. Handa and M. M. Harjai, “Hydatid Cyst of the Renal Pelvis,” Pediatric Surgery International, Vol. 21, No. 5, 2005, pp. 410-412. [16] S. J. McCorkell, “Unintended Percutaneous Aspiration of Pulmonary Echinococcal Cysts,” American Journal of Roentgenology, Vol. 143, No. 1, 1984, pp. 123-126. [17] P. R. Mueller, S. L. Dawson, J. T. Ferrucci, Jr. and G. L. Nardi, “Hepatic Echinococcal Cyst: Successful Percuta- neous Drainage,” Radiology, Vol. 155, No. 3, 1985, pp. 627-628. |