Chinese Medicine
Vol.4 No.3(2013), Article ID:36122,8 pages DOI:10.4236/cm.2013.43012
The Eastern Cultural Signature of Traditional Chinese Medicine: Empirical Evidence and Theoretical Perspectives
State Key Laboratory of Cognitive Neuroscience and Learning, Beijing Normal University, Beijing, China
Email: #liujia@bnu.edu.cn
Copyright © 2013 Huanhua Lu et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received June 14, 2013; revised July 19, 2013; accepted July 30, 2013
Keywords: association; Eastern holistic thinking; individual difference; Traditional Chinese Medicine (TCM); variability; Western medicine
ABSTRACT
Background: Holistic thinking, which is rooted in Eastern culture, is assumed to be the core of traditional Chinese medicine (TCM). Recently, such holistic thinking has been proposed to be applicable to Western medicine practices for alleviating serious side effects; however, the obscure and often ill-defined terms of TCM, such as qi, yin yang, and wuxing, pose considerable obstacles for further understanding TCM. In the present study, we explored whether and how TCM is actually related to the scientific construct of holistic thinking, to elucidate the particular cultural signature of TCM. Methods: A random sample of 101 college students majoring in TCM and 93 non-medical college students was recruited for the study. Two psychological scales—the Chinese Holistic Thinking Scale and the TCM Competence Scale were used respectively to measure the holistic thinking and participants’ ability to apply the TCM in practice. Results: We found that individuals who thought more holistically were better at applying TCM to modern medical problems. Interestingly, TCM was associated with holistic thinking in both TCM and non-medical students, suggesting that this association is intrinsic. Further exploration revealed that the association and variability facets of Eastern holistic thinking—which emphasize that the world is interconnected and ever-changing, respectively—significantly accounted for the individual differences in competence in utilizing TCM in practice. Conclusion: In short, our study provides the first empirical evidence linking TCM to the Eastern holistic thinking style, which not only deepens the understanding of TCM from a scientific perspective but also promotes dialogue between TCM and Western medicine for building safer and more effective health care systems.
1. Introduction
Traditional Chinese medicine (TCM) is a complete and independent medical system, which has been used to diagnose, treat, and prevent illnesses for thousands of years. Ever since the World Health Organization began exploring TCM in the 1950s, interest in it has been growing rapidly beyond China because of its particular therapeutic methods and effects. Currently, in many countries, TCM is practiced alongside Western medicine, providing patients with a wide array of therapeutic options. Thus, the integration of two medical traditions can take advantage of the strong points of both traditions to facilitate safer, faster, and more effective health care [1-4].
Because Western medicine and TCM arise in different cultural backgrounds, they show different characteristics, especially in the thinking styles for making diagnoses [1]. Western medicine primarily examines the material aspects of the body and treats illnesses by using drugs, radiation, and surgery, relying on a wide body of scientific evidence. In contrast, TCM emphasizes a more holistic approach and aims to cure and maintain balance in the body through more natural treatments [5-7]. In other words, TCM treats patients as an integrated whole, while Western medicine focuses on the specific symptoms associated with illness [3,8]. Therefore, although Western medicine is generally more effective in treating acute diseases than TCM, such treatment is usually accompanied by serious side effects, such as fatigue, nausea, or hair loss [9,10]. Therefore, Western medicine may benefit from the acquisition of a more holistic approach, which can be obtained by using the techniques and thinking style of TCM to alleviate or even eliminate the unpleasant side effects of drugs and radiation therapy [2,3].
As a discipline rooted in Eastern traditional culture, TCM is not just a medical system, but also an important branch of Eastern philosophy and the Chinese healing arts. Therefore, TCM uses symbolic concepts to emphasize the integration of the body and mind. According to TCM terminology, health is thought to result from a delicate balance between yin (negativity) and yang (positivity) in the body. The body is thought to be constituted of qi (vital energy) and blood instead of tissues and organs. Furthermore, the body is divided into five functional sub-systems—liver, heart, spleen, lungs, and kidneys, corresponding to the Taoist concept of wuxing (five elements) [1]. However, these obscure concepts are often regarded as inaccurate descriptions of the human body in the eyes of Western medical practitioners [11]; this notion greatly interferes with appropriate understanding of TCM from a Western medicine perspective. Therefore, in the present study, we explore the particular cultural characteristics of TCM by using a well-established scale assessing Eastern holistic thinking style in an empirical study.
The core of holistic thinking is the belief that every element in the world is interconnected [12-16]. In the past two decades, numerous cross-cultural studies have demonstrated that East Asians, especially Chinese, prefer to think in a holistic way, whereas Westerners tend to engage more in analytic thinking [15,17-19]. For example, East Asians often pay more attention to context and the relationships between issues, while Westerners are more attentive to distinctive features [20-27]. Furthermore, East Asians are more likely to attribute behaviors to contextual factors than to personal dispositions, while Westerners do the opposite [28-35]. Finally, East Asians show more tolerance for contradiction and are more likely to expect changes in current trends, while Westerners prefer non-contradictory arguments and often predict that current trends will continue [36-41].
Despite theories assuming that TCM is rooted in holistic thinking, to our knowledge, no empirical study has directly examined the relationship between holistic thinking and TCM. To fill this gap, we investigated whether and how TCM relates to Eastern holistic thinking style by using two psychological scales—the Chinese Holistic Thinking Scale (CHTS) [42-45] and the Traditional Chinese Medicine Competence Scale (TCMCS), which was designed for this study. We investigated whether individuals who scored higher on the CHTS possessed greater competence in TCM practice, as measured by the TCMCS. In addition, we tested both students of TCM and non-medical students to examine whether the relationship between TCM and holistic thinking, if observed, is intrinsic, and therefore independent of TCM education.
2. Method
2.1. Participants
One hundred and one college students majoring in TCM at the Beijing University of Chinese Medicine (67 women; mean age = 20.86, SD = 0.61) and 93 non-medical college students at Beijing Normal University (64 females; mean age = 20.54, SD = 0.59) participated in the study. At the time of testing, the TCM students had already taken at least one year of core courses on TCM and had been trained in clinical practices such as acupuncture and moxibustion. The non-medical students had no history of any medical training. The study was approved by the institutional review board of Beijing Normal University. All subjects were informed that they were participating in a social and behavioral survey, and that their answers would be used only for the purposes of scientific research and would be kept strictly confidential. Before testing, written informed consent was obtained from all participants.
2.2. Measures
Eastern holistic thinking style was measured with the CHTS [44], a 26-item questionnaire using a 7-point Likert-type scale from “completely disagree” (1) to “completely agree” (7). The CHTS contains three facets: association, variability, and contradiction. The association facet consists of 13 questions such as “I always think about all of the aspects of others,” which asserts that everything in the world is interconnected and nothing can be separated from the rest of the world. The contradiction facet consists of nine questions such as “I often do something which I do not really like,” which holds that the world is a contradictory entity with old and new, good and bad, strong and weak opposites, coexisting in everything. Finally, the variability facet contains four items such as “I think that a person’s habits are difficult to change,” which emphasizes that everything in the world is changeable and flexible, and nothing can stand still or remain fixed. The CHTS has excellent reliability and validity [42-45]. Both the total score and the score of each facet were used in the following analyses.
To assess participants’ ability to apply TCM theories in tackling medical problems, we created the TCMCS. To conceptualize TCM competence and generate items to assess it, we generated 60 items on the use of TCM to diagnose medical problems by reviewing the literature on TCM. An example item is “In my opinion, illness is related to one’s living environment, daily diet, and mood states.” Of these 60, 25 were selected by eleven TCM experts from the Beijing University of Chinese Medicine and the Chinese Academy of Traditional Chinese Medicine. A pilot study revealed sixteen items that had high internal consistency and test-retest reliability; these were selected as the items of the TCMCS (see Appendix for all items). All were rated on a 7-point Likert-type scale from “completely disagree” (1) to “completely agree” (7). Individuals who scored higher on the TCMCS were better at applying the TCM in practice.
Nine participants were excluded because of missing items in the questionnaire. Three additional participants (1.5% of the sample) with outlier responses—that is, scoring over three SDs from the group mean—were excluded from further analyses. Therefore, the final sample comprised 182 participants (92 TCM students; 90 nonmedical students).
3. Results
The CHTS, which was used to measure Eastern holistic thinking style, had high internal consistency reliability (Cronbach’s α = 0.73). The reliability of its three subscales was also adequate (association: α = 0.79; variability: α = 0.83; contradiction: α = 0.65). Similarly, the TCMCS, which was used to measure participants’ competence in TCM practice, also had high internal consistency reliability (Cronbach’s α = 0.75). Participants with TCM training (i.e., TCM students) scored significantly higher on the TCMCS than did the non-medical students; TCM students: mean = 92.9, SD = 9.64; nonmedical students: mean = 82.8, SD = 9.19; t(180) = 7.2, p < 0.001; these data indicate that the TCMCS had high construct validity. Next, we investigated whether participants who preferred to think holistically were better at TCM practice.
First, we examined the relationship between holistic thinking and TCM competence in TCM students. The significant positive correlation found between holistic thinking and TCM competence (r = 0.27, p = 0.009; Figure 1(a)) suggested that individuals who had an Eastern holistic thinking style exhibited greater TCM competence. To further examine whether this association was established through education on TCM, or whether it was an intrinsic property of Eastern culture, we examined the association in a group of non-medical students who had no experience with or knowledge of TCM. Interestingly, in this sample, we observed a similar association (r = 0.38, p < 0.001; Figure 1(b)); this was further confirmed by Fisher’s Z-test analysis, in that there was no significant group difference in the correlation (Z < 1). Therefore, we conclude that the association between Eastern holistic thinking and TCM competence is intrinsic, and independent of TCM education. Taken together, our findings indicate that TCM competence is the realization of Eastern holistic thinking in practice.
To further examine which specific facets of Eastern holistic thinking (as measured by the CHTS) affect TCM competence, we performed a stepwise multiple regression analysis. To increase the statistical power, both the TCM and non-medical students were included in the analysis because they showed the same pattern in the association between holistic thinking and TCM competence. In this analysis, we used TCM competence as the dependent variable, and the three facets of Eastern holistic thinking (i.e., association, variability, and contradicttion) as covariates of interest, controlling for gender and age. The regression analysis revealed that both the association and variability facets, not the contradiction facet, significantly predicted TCM competence (Table 1), together accounting for 11.8% of the variance in TCM competence. The finding was further confirmed by correlation analyses between the three facets of Eastern holistic thinking and TCM competence (association: r = 0.17, p = 0.02; variability: r = 0.27, p < 0.001; contradiction: r = −0.01, p = 0.86; Figure 2).
4. Discussion
Holistic thinking and TCM are arguably the most representative markers of Eastern culture. Many theorists believe that TCM naturally embeds holistic thinking in medical practice [5,7,19]. Our study used the individual differences approach to provide the first empirical evidence supporting this speculation. That is, individuals who preferred to think holistically were more competent in putting TCM into practice. Importantly, this link was observed even in individuals who had no knowledge of TCM, suggesting that the link is intrinsic, and independent of education on TCM.
Our study not only adds to the findings of previous cross-culture studies on thinking style but also deepens the understanding of TCM. In previous studies on the differences in thinking style between people from Eastern and Western cultures, researchers focused on cultural influences on cognitions as tested in laboratories, such as attention, categorization, and attribution, and rarely on
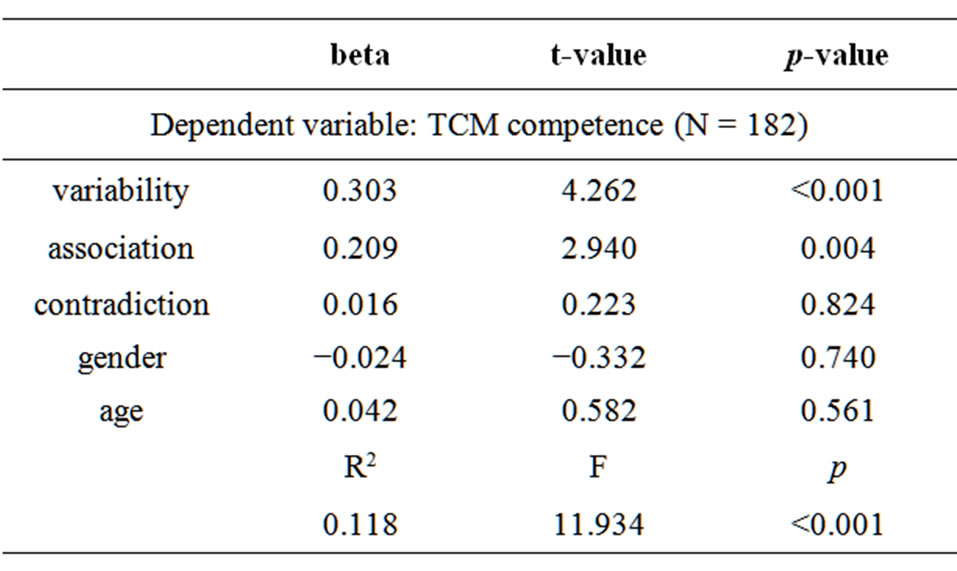
Table1. . Multiple regression analysis testing the relationship between TCM competence and the three facets of holistic thinking.
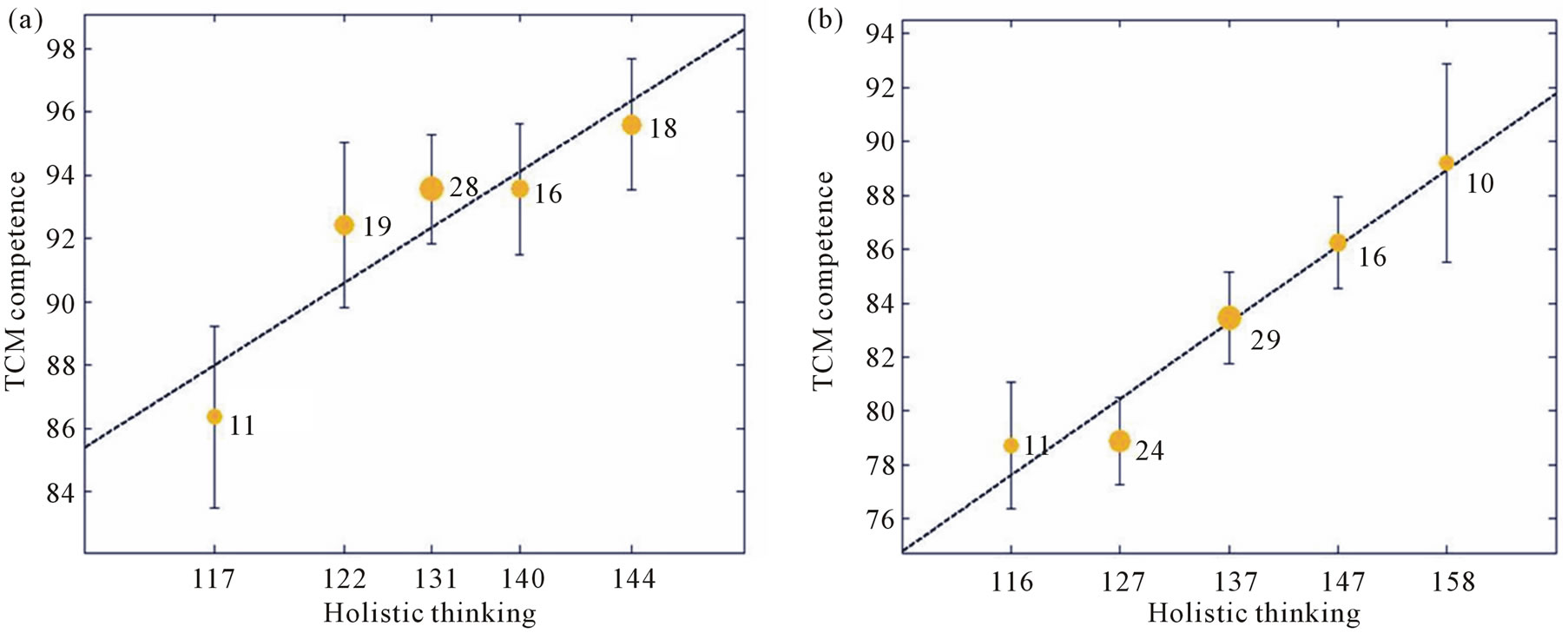
Figure 1. Binned scatter plots between TCM competence and Eastern holistic thinking in (a) TCM students, (b) non-medical students. The x-axis denotes participants’ scores on the Chinese Holistic Thinking Scale (CHTS), with higher scores indicating preference for holistic thinking. The y-axis denotes participants’ scores on the Traditional Chinese Medicine Competence Scale (TCMCS), with higher scores indicating higher competence in TCM practice. To avoid overlap between participants with similar scores, participants were binned into groups according to holistic thinking scores. Dot size is proportional to the number of observations, which are listed next to each dot. Error bars indicate standard errors of the mean.
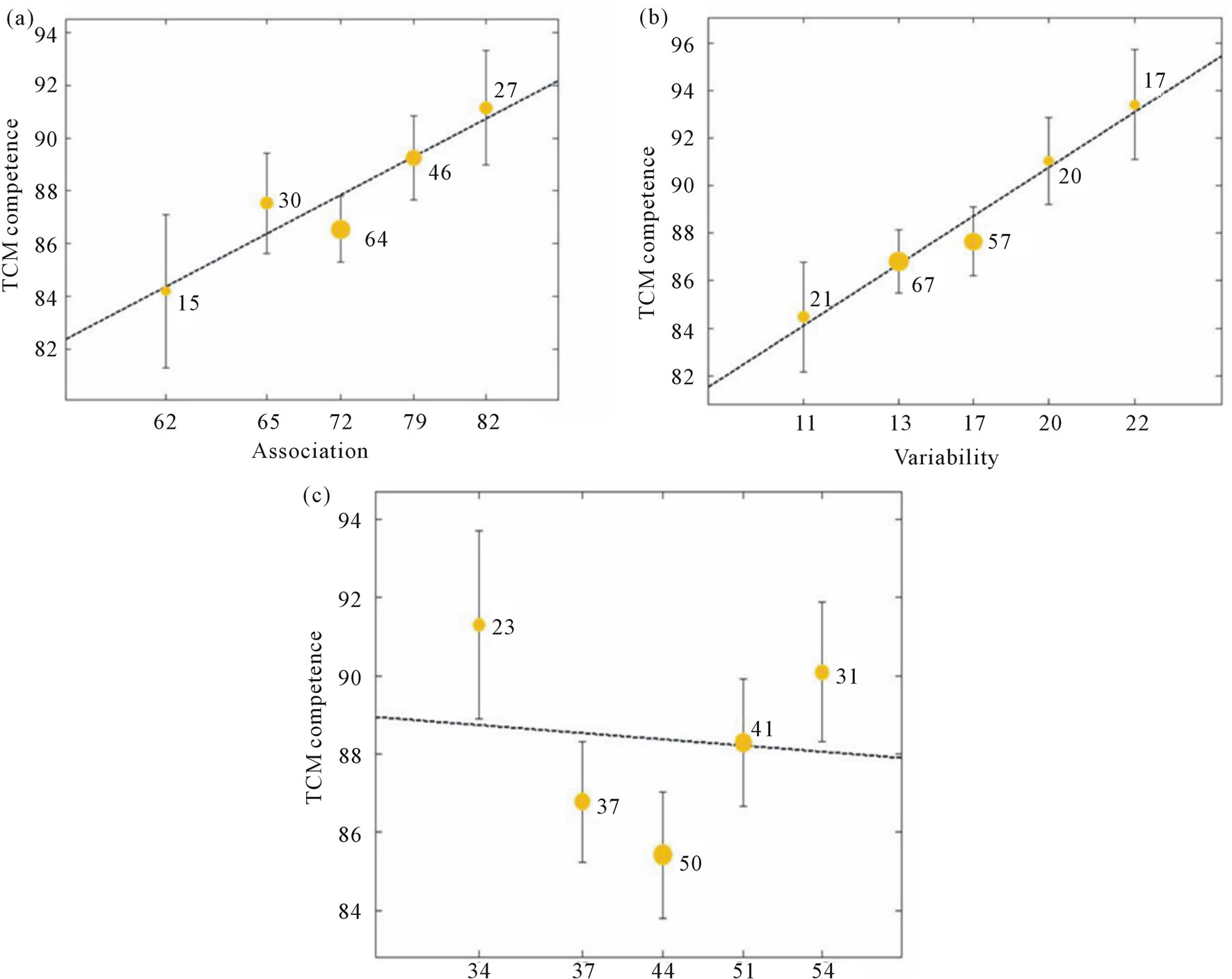
Figure 2. Binned scatter plots between TCM competence and the three facets of Eastern holistic thinking: (a) association, (b) variability, and (c) contradiction. To avoid overlap between participants with similar scores, participants were binned into groups according to scores for association, variability, and contradiction facets. Dot size is proportional to the number of observations, which are listed next to each dot. Error bars indicate standard errors of the mean.
daily activities or common practices [20,21,28,46-50]. The link between holistic thinking and TCM observed in this study thus provides a new platform for further investigation of how Eastern culture affects daily behaviors through thinking in general, and of the culture difference between TCM and Western medicine in particular. Furthermore, our study aids in understanding the obscure concepts in TCM such as yin yang, wuxing, and qi by making the thinking style through which they were formed more accessible to scientific study. In TCM, yin and yang are complementary opposites that are interdependent; wuxing emphasizes dynamic interactions and the balance of organs; and qi is regarded as the ultimate constituent of the world, the nature of the cosmic movement, and the medium that connects everything in the universe [7,51,52]. Our finding that the association and variability facets of CHTS were correlated with TCM competence confirmed the hypothesis that the yin yang, wuxing, and qi concepts in TCM derive from the associative and flexible nature of Eastern holistic thinking [7,51].
Why is there an association between holistic thinking and TCM? One possible reason is that both originate from the agrarian culture of Eastern societies and philosophy [5,7,15,19]. In Eastern societies, irrigated agriculture and changeable climatic conditions require cooperation and coordination with a substantial number of individuals for effective economic activities. Therefore, individuals living in such an interdependent social environment may have needed to attend more to interpersonal relationships and to emphasize the harmony between human and nature, which are core tenets of Eastern holistic thinking [15,19]. In parallel, TCM, which stems from practices in agricultural production, uses metaphors to understand the body (e.g., liver, heart, spleen, lungs, and kidneys) in terms of natural phenomena (e.g., metal, wood, water, fire, and earth), and thus integrates the body and nature into a unified whole. From the perspective of Eastern philosophy, the Yi Jing (the Book of Changes), the first Chinese philosophy book written during the Zhou Dynasty (1111-721 BC), offers a comprehensive view on the interconnected and everchanging nature of the universe and human societies. Therefore, the holistic thinking style suggested by Chinese philosophy likely serves as a cognitive schema in TCM practice, where TCM doctors are more likely to search for integrated patterns among seemingly fragmented elements. Taken together, because of the shared source of the agrarian culture and the common root of Chinese philosophy, it is not surprising that the link between holistic thinking and TCM competence was also found in individuals who were naïve to TCM. This observation has considerable implications in practice. In medical schools that teach TCM, education on traditional Chinese philosophy and culture could improve students’ TCM competence. Conversely, studying TCM may help people master Eastern holistic thinking styles [8,53].
Our study further demonstrated that the association and variability facets, and not the contradiction facet, of the CHTS were correlated with TCM competence, which may help enrich the thinking style of Western medicine. In terms of the association facet, diseases are not only caused by particular types of viruses, but also by lifestyles or emotion states. That is to suggest, therapy should focus more on the person with the disease, instead of the disease itself. Similarly, the variability facet suggests the benefits of individualized therapy based on a combination of treating symptoms and monitoring patients’ physical conditions, and even their psychological traits. With future studies on the relation between Western analytical thinking and Western medicine, we can deepen our understanding of the cultural signatures of both TCM and Western medicine, which may help in building a safer and more effective system to promote physical health and well-being.
5. Conclusion
Our study used the individual differences approach to provide the first empirical evidence linking TCM to the Eastern holistic thinking style. That is, individuals who preferred to think holistically were more competent in applying TCM in practice. Importantly, this link was observed even in individuals who had no knowledge of TCM, suggesting that the link is intrinsic, and independent of education on TCM, which not only deepens the understanding of TCM from a scientific perspective but also promotes dialogue between TCM and Western medicine for building safer and more effective health care systems.
6. Acknowledgements
This study was funded by the National Social Science Foundation of China (11&ZD187) and the National Basic Research Program of China (2011CB505402).
REFERENCES
- K. Chen and H. Xu, “The integration of Traditional Chinese Medicine and Western Medicine,” European Review, Vol. 11, No. 2, 2003, pp. 225-235.
- I. Holliday, “Traditional Medicines in Modern Societies: An Exploration of Integrationist Options through East Asian Experience,” Journal of Medicine and Philosophy, Vol. 28, No. 3, 2003, pp. 373-389. doi:10.1076/jmep.28.3.373.14587
- J. Lake, “The Integration of Chinese Medicine and Western Medicine: Focus on Mental Illness,” Integrative Medicine, Vol. 3, No. 4, 2004, pp. CB-CJ.
- G. J. Andrews, J. Evans and S. McAlister, “Creating the Right Therapy Vibe: Relational Performances in Holistic Medicine,” Social Science & Medicine, Vol. 83, April 2013, pp. 99-109. doi:10.1016/j.socscimed.2013.01.008
- T. J. Kaptchuk, “The Web That Has No Weaver: Understanding Chinese Medicine,” McGraw-Hill, New York, 2000.
- E. Yu, “Essential Traditional Chinese Medicine: Western Scientific Medicine Perspective,” Hong Kong Practitioner, Vol. 23, No. 1, 2001, pp. 20-27.
- D. E. Kendall, “Dao of Chinese Medicine: Understanding an Ancient Healing Art,” Oxford University Press, Oxford, 2002.
- M. Koo and I. Choi, “Becoming a Holistic Thinker: Training Effect of Oriental Medicine on Reasoning,” Personality and Social Psychology Bulletin, Vol. 31, No. 9, 2005, pp. 1264-1272. doi:10.1177/0146167205274692
- T. P. Lam, “Strengths and Weaknesses of Traditional Chinese Medicine and Western Medicine in the Eyes of Some Hong Kong Chinese,” Journal of Epidemiology and Community Health, Vol. 55, No. 10, 2001, pp. 762- 765. doi:10.1136/jech.55.10.762
- D. Normile, “The New Face of Traditional Chinese Medicine,” Science, Vol. 299, No. 5604, 2003, pp. 188-190. doi:10.1126/science.299.5604.188
- J. Qiu, “Traditional Medicine: A Culture in the Balance,” Nature, Vol. 448, No. 7150, 2007, pp. 126-128. doi:10.1038/448126a
- D. J. Munro, “Individualism and Holism: Studies in Confucian and Taoist Values,” Center for Chinese Studies, University of Michigan, Ann Arbor, 1985.
- H. Nakamura, “Ways of Thinking of Eastern Peoples,” University of Hawaii Press, Honolulu, 1964.
- J. Needham, “Science and Civilisation in China. Vol. 4: Physics and Physical Technology,” Cambridge University Press, Cambridge, 1962.
- R. E. Nisbett, K. Peng, I. Choi and A. Norenzayan, “Culture and Systems of Thought: Holistic Versus Analytic Cognition,” Psychological Review, Vol. 108, No. 2, 2001, p. 291. doi:10.1037/0033-295X.108.2.291
- D. Oyserman and S. W. Lee, “Does Culture Influence What and How We Think? Effects of Priming Individualism and Collectivism,” Psychological Bulletin, Vol. 134, No. 2, 2008, pp. 311-342. doi:10.1037/0033-2909.134.2.311
- R. E. Nisbett and T. Masuda, “Culture and Point of View,” Proceedings of the National Academy of Sciences, Vol. 100, No. 19, 2003, pp. 11163-11170. doi:10.1073/pnas.1934527100
- R. E. Nisbett and Y. Miyamoto, “The Influence of Culture: Holistic versus Analytic Perception,” Trends in Cognitive Sciences, Vol. 9, No. 10, 2005, pp. 467-473. doi:10.1016/j.tics.2005.08.004
- R. E. Nisbett, “The Geography of Thought: How Asians and Westerners Think Differently and Why,” Free Press, New York, 2003.
- H. F. Chua, J. E. Boland and R. E. Nisbett, “Cultural Variation in Eye Movements during Scene Perception,” Proceedings of the National Academy of Sciences, Vol. 102, No. 35, 2005, pp. 12629-12633. doi:10.1073/pnas.0506162102
- L.-J. Ji, K. Peng and R. E. Nisbett, “Culture, Control, and Perception of Relationships in the Environment,” Journal of Personality and Social Psychology, Vol. 78, No. 5, 2000, pp. 943-955.
- A. Boduroglu, P. Shah and R. E. Nisbett, “Cultural Differences in Allocation of Attention in Visual Information Processing,” Journal of Cross-Cultural Psychology, Vol. 40, No. 3, 2009, pp. 349-360. doi:10.1177/0022022108331005
- S. Duffy and S. Kitayama, “Mnemonic Context Effect in Two Cultures: Attention to Memory Representations?” Cognitive Science, Vol. 31, No. 6, 2007, pp. 1009-1020. doi:10.1080/03640210701703808
- M. Doherty, H. Tsuji and W. A. Phillips, “The ContextSensitivity of Visual Size Perception Varies across Cultures,” Perception, Vol. 37, No. 9, 2008, pp. 1426-1433. doi:10.1068/p5946
- T. Masuda, R. Gonzalez, L. Kwan and R. E. Nisbett, “Culture and Aesthetic Preference: Comparing the Attention to Context of East Asians and Americans,” Personality and Social Psychology Bulletin, Vol. 34, No. 9, 2008, pp. 1260-1275. doi:10.1177/0146167208320555
- K. Rayner, X. Li, C. C. Williams, K. R. Cave and A. D. Well, “Eye Movements during Information Processing Tasks: Individual Differences and Cultural Effects,” Vision Research, Vol. 47, No. 21, 2007, pp. 2714-2726. doi:10.1016/j.visres.2007.05.007
- X. Li, J. Zhang, Y. Huang, M. Xu and J. Liu, “Nurtured to Follow the Crowd: A Twin Study on Conformity,” Chinese Science Bulletin, Vol. 58, No. 10, 2013, pp. 1175- 1180. doi:10.1007/s11434-013-5701-x
- I. Choi and R. E. Nisbett, “Situational Salience and Cultural Differences in the Correspondence Bias and ActorObserver Bias,” Personality and Social Psychology Bulletin, Vol. 24, No. 9, 1998, pp. 949-960. doi:10.1177/0146167298249003
- I. Choi, R. E. Nisbett and A. Norenzayan, “Causal Attribution across Cultures: Variation and Universality,” Psychological Bulletin, Vol. 125, No. 1, 1999, pp. 47-63. doi:10.1037/0033-2909.125.1.47
- Lee F, Hallahan M, Herzog T: Explaining real-life events: How culture and domain shape attributions. Personality and Social Psychology Bulletin, Vol. 22, No. 7, 1996, pp. 732-741. doi:10.1177/0146167296227007
- M. W. Morris and K. Peng, “Culture and Cause: American and Chinese Attributions for Social and Physical Events,” Journal of Personality and Social Psychology, Vol. 67, No. 6, 1994, pp. 949-949. doi:10.1037/0022-3514.67.6.949
- T. Masuda and S. Kitayama, “Perceiver-Induced Constraint and Attitude Attribution in Japan and the US: A Case for the Cultural Dependence of the Correspondence Bias,” Journal of Experimental Social Psychology, Vol. 40, No. 3, 2004, pp. 409-416. doi:10.1016/j.jesp.2003.08.004
- Y. Miyamoto and S. Kitayama, “Cultural Variation in Correspondence Bias: The Critical Role of Attitude Diagnosticity of Socially Constrained Behavior,” Journal of Personality and Social Psychology, Vol. 83, No. 5, 2002, pp. 1239-1248. doi:10.1037/0022-3514.83.5.1239
- A. Norenzayan, I. Choi and R. E. Nisbett, “Cultural Similarities and Differences in Social Inference: Evidence from Behavioral Predictions and Lay Theories of Behavior,” Personality and Social Psychology Bulletin, Vol. 28, No. 1, 2002, pp. 109-120. doi:10.1177/0146167202281010
- M. D. Lieberman, J. M. Jarcho and J. Obayashi, “Attributional Inference across Cultures: Similar Automatic Attributions and Different Controlled Corrections,” Personality and Social Psychology Bulletin, Vol. 31, No. 7, 2005, pp. 889-901. doi:10.1177/0146167204274094
- K. Peng, “Naive Dialecticism and Its Effects on Reasoning and Judgment about Contradiction,” University of Michigan, Ann Arbor, 1997.
- K. Peng and R. E. Nisbett, “Culture, Dialectics, and Reasoning about Contradiction,” American Psychologist, Vol. 54, No. 9, 1999, pp. 741-754. doi:10.1037/0003-066X.54.9.741
- I. Choi and R. E. Nisbett, “Cultural Psychology of Surprise: Holistic Theories and Recognition of Contradiction,” Journal of Personality and Social Psychology, Vol. 79, No. 6, 2000, pp. 890-905. doi:10.1037/0022-3514.79.6.890
- L.-J. Ji, R. E. Nisbett and Y. Su, “Culture, Change, and Prediction,” Psychological Science, Vol. 12, No. 6, 2001, pp. 450-456. doi:10.1111/1467-9280.00384
- L.-J. Ji, Z. Zhang and T. Guo, “To Buy or to Sell: Cultural Differences in Stock Market Decisions Based on Price Trends,” Journal of Behavioral Decision Making, Vol. 21, No. 4, 2008, pp. 399-413. doi:10.1002/bdm.595
- J. Spencer-Rodgers, M. J. Williams and K. Peng, “Cultural Differences in Expectations of Change and Tolerance for Contradiction: A Decade of Empirical Research,” Personality and Social Psychology Review, Vol. 14, No. 3, 2010, pp. 296-312. doi:10.1177/1088868310362982
- Y. Hou, “Research Progress in Thinking Styles from the Perspective of Cultural Psychology,” Advances in Psychological Science, Vol. 15, No. 2, 2007, pp. 211-216.
- Y. Hou, M. Zhang and X. Wang, “The Relationship between Adolescents’ Thinking Style and their Coping Style,” Chinese Mental Health Journal, Vol. 21, No. 3, 2007, pp. 158-161.
- Y. B. Hou and Y. Zhu, “The Chinese Holistic Thinking Styles: Their Structure and Effect,” APA Annual Symposium, Chicago, 22-25 August 2002, pp. 22-25.
- Y. Hou, Y. Zhu and K. Peng, “How the Thinking Style Affect Managers’ Attribution,” In: D. Wang and Y. Hou, Eds., Personality and Social Psychology, Peking University Press, Beijing, 2004, pp. 115-130.
- L.-J. Ji, Z. Zhang and R. E. Nisbett, “Is It Culture or Is It Language? Examination of Language Effects in CrossCultural Research on Categorization,” Journal of Personality and Social Psychology, Vol. 87, No. 1, 2004, pp. 57- 65.
- A. Norenzayan, E. E. Smith, B. J. Kim and R. E. Nisbett, “Cultural Preferences for Formal versus Intuitive Reasoning,” Cognitive Science, Vol. 26, No. 5, 2002, pp. 653- 684. doi:10.1207/s15516709cog2605_4
- E. E. Buchtel and A. Norenzayan, “Which Should You Use, Intuition or Logic? Cultural Differences in Injunctive Norms about Reasoning,” Asian Journal of Social Psychology, Vol. 11, No. 4, 2008, pp. 264-273. doi:10.1111/j.1467-839X.2008.00266.x
- L.-J. Ji, T. Guo, Z. Zhang and D. Messervey, “Looking into the Past: Cultural Differences in Perception and Representation of Past Information,” Journal of Personality and Social Psychology, Vol. 96, No. 4, 2009, pp. 761-769. doi:10.1037/a0014498
- W. W. Maddux and M. Yuki, “The ‘Ripple Effect’: Cultural Differences in Perceptions of the Consequences of Events,” Personality and Social Psychology Bulletin, Vol. 32, No. 5, 2006, pp. 669-683. doi:10.1177/0146167205283840
- Y. H. Zhang and K. Rose, “A Brief History of Qi,” Paradigm Publications, Brookline, 2001.
- L. Lao, L. Xu and S. Xu, “Traditional Chinese Medicine,” In: A. Längler, P. J. Mansky and G. Seifert, Eds., Integrative Pediatric Oncology, Springer, Berlin, 2012, pp. 125- 135. doi:10.1007/978-3-642-04201-0_9
- C.-Y. Kim and B. Lim, “Modernized Education of Traditional Medicine in Korea: Is It Contributing to the Same Type of Professionalization Seen in Western Medicine?” Social Science & Medicine, Vol. 58, No. 10, 2004, pp. 1999-2008. doi:10.1016/S0277-9536(03)00405-2
Appendix:
Traditional Chinese Medicine Competence Scale (TCMCS)
1)* The brain is the organ of thinking; therefore, mental disorders damage the brain, not the five viscera.
2)* Health and disease are always contradictory.
3) There are multiple ways to reach the truth of a complicated issue.
4)* Using metaphors to understand the functionality of organs in terms of natural phenomena cannot lead to correct answers.
5) In my opinion, illness is related to one’s living environment, daily diet, and mood states.
6) The dysfunction of an organ can result in the change of its structure.
7)* Scientific studies show that gypsum contains no antiviral ingredient, so it is useless for patients with viral influenza.
8)* On the issue of health, I prefer to trust reports from medical instruments, rather than subjective feelings.
9) How an illness manifests itself in the body is constantly changing.
10)* The human body is similar to a delicate machine, which will operate perfectly so long as the exact problem is identified and fixed.
11)* Meridians and collaterals do not really exist in the body; they are imaginary.
12)* There is no connection between abnormal feces and dysfunctions in the lungs, liver, spleen, or kidneys.
13)* To treat coughing or shortness of breath, we must focus on the lungs, and not on the liver or kidneys.
14)* Since the body is a natural phenomenon, it must be measured with scientific standards that are the same as those used in physics and chemistry.
15) In order to understand the laws of life, we must study health and diseases from multiple angles, such as their physiological structures, psychological factors, environmental factors, and nature.
16)* I believe that killing cancer cells is the only way to cure cancer.
*: reversed-scored items.
NOTES
*Huanhua Lu and Yi’nan Wang contributed equally to this study.
#Corresponding author.