Open Journal of Pathology
Vol. 2 No. 2 (2012) , Article ID: 18563 , 2 pages DOI:10.4236/ojpathology.2012.22005
Tonsillar Lipoma: Report of 2 Cases
![]()
Department of Pathology, Habib Bourguiba University Hospital, Sfax, Tunisia.
Email: *samehktari@yahoo.fr
Received December 15th, 2011; revised January 16th, 2012; accepted February 27th, 2012
Keywords: Lipoma; Tonsil; Histology
ABSTRACT
Lipomas are benign slow-growing neoplasms composed of mature fat cells. Their occurrence in the oral cavity is rare representing only 1% - 4% of all benign neoplasms of this location. Tonsillar lipomas are extremely rare. Only 15 cases have been reported in the world literature so far. We present two new cases of lipoma affecting the palatine tonsils with a review of the related literature.
1. Introduction
Lipomas are benign mesenchymal neoplasms composed of mature adipocytes. Although they represent one of the most common neoplasms of soft tissue, only 1% - 4% of cases occur in the oral cavity [1]. In fact, lipomatous tumors represent an infrequent cause for upper aerodigestive neoplasms especially concerning the tonsils [2]. We report two new cases of tonsillar lipoma in purpose to highlight the presence of this rare entity.
2. Case 1
A 62-year-old woman complained of a throat discomfort evolving for several months not associated with fever or any other otolaryngological symptoms. She was obese and did not report history of intraoral trauma. Examination revealed a polypoid, pedunculated tumor measuring 1 × 0.5 cm on the upper pole of the right tonsil. A right tonsillectomy was performed. The tumor was lobulated, thinly encapsulated with a smooth yellowish cut surface. Histological examination revealed sheets of mature adipocytes containing large clear cytoplasm and eccentric nuclei with no evidence of cellular atypia leading for the diagnosis of lipoma. The patient has remained free of any symptoms for over 24 months of follow-up.
3. Case 2
A 19-year-old young man presented with angina. Otolaryngological examination revealed a right tonsillar polyp. It was 1.7 × 0.9 cm and did not cause any discomfort or pain. Elective excision of the tonsillar polyp was performed. It was polypoid (Figure 1), composed of mature fat and was covered by a nonkeratinizing squamous epithelium with an underlying rim of lymphoid tissue (Figure 2). The diagnosis of lipoma was made. The patient reported no prior personal histories related to this problem. After 1 year follow-up, the patient is asymptomatic with no residua or recurrence.
4. Discussion
Palatine tonsils are accumulations of lymphoid tissue located in the lateral wall of the oropharynx and covered by a stratified squamous epithelium. The normal tonsillar histology is devoid of adipocytes [3] and lipomatous tumors of the tonsils are extremely rare [4]. To our knowledge, there are about fifteen previously reported cases of

Figure 1. A polypoid, thinly encapsulated tumor composed of mature adipose tissue (scanning of the slide) (Case 2).
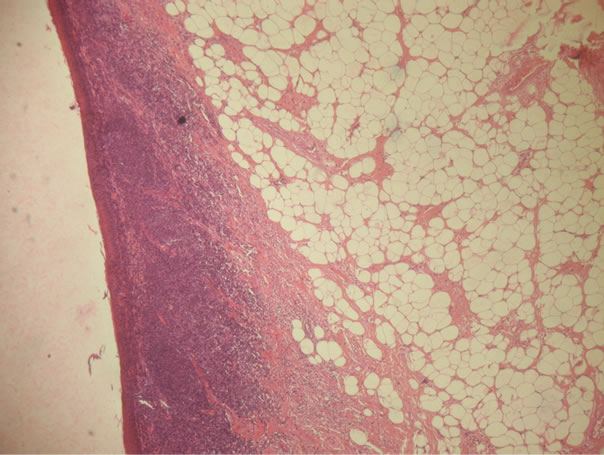
Figure 2. Proliferation of mature adipocytes covered by a nonkeratinizing squamous epithelium with an underlying rim of lymphoid tissue (×100) (Case 2).
tonsillar lipoma in the world literature review [5]. Generally, their prevalence does not differ with gender, although a male predilection has been recorded [6] and they occur most often in patients older than 40 years [1]. The cases we described illustrate that both genders can be affected and that tonsillar lipoma can be seen also in young patients.
The etiology is unknown. However, it is thought that trauma may trigger proliferation of fatty tissue and cause lipomas [7], besides lipomas seem to be more common in obese people [1]. Begin and Frenkiel state that the occurrence of lipomas in the tonsil is plausible owing to the delicate mesenchymal framework present in the normal tonsil [3].
Clinically, tonsillar lipomas are slow growing painless masses and patients commonly present with a well-circumscribed mass that have been developing for several years [1], but they may manifest symptoms such as voice change, dysphagia, soreness, excessive salivation or foreign body sensation as in our first reported case. Furthermore, when they reach an important size, these tumors may cause respiratory obstruction [3]. Dereköy et al. decribed one case of tonsillar lipoma measuring 3.6 cm of lengh and causing dyspnea, hypoxemia and respiratory acidosis. The tonsillar lipomas of our two patients did not exceed 2 cm of length and symptoms were either minimal or absent.
Although magnetic resonance imaging and computerized tomographic scans are very useful in the clinical diagnosis, the histopathology remains the gold standard in the diagnosis of lipomas [1].
Grossly, lipomas present as yellowish rounded multilobutated masses enclosed in a delicate capsule. Microscopically, they consist in sheets of mature adipocytes, containing large clear cytoplasm and eccentric nuclei, arranged in lobules with intervening fibrovascular connective tissue septa.
Differential diagnosis includes other benign tumors of the tonsils such as papilloma, which represent the most common neoplasm of the tonsils [6]. Although extremely rare, malignant change in lipoma was described. Saddik et al. reported one case of an underdiagnosed liposarcoma of the tonsillar fossa [4]. Therefore, histopathological evaluation of this kind of tumor is very important.
Surgical excision is the usual mode of treatment in symptomatic cases [3]. Recurrence is unusual and the prognosis is excellent, although Masson et al reported a case of hypopharyngeal lipoma with local recurrence or association with new lipoma elsewhere in the hypopharynx following resection [8].
REFERENCES
- R. Kaur, S. Kler and A. Bhullar, “Intraoral Lipoma: Report of 3 Cases,” Dental Research Journal, Vol. 8, No. 1, 2011, pp. 48-51.
- T. R. Kapur, “Recurrent Lipomata of the Larynx and the Pharynx with Late Malignant Change,” Journal of Laryngology and Otology, Vol. 82, No. 8, 1968, pp. 761-768. doi:10.1017/S0022215100069425
- R. Nandakumar, Y. K. Inchara, O. D’ Souza, V. Sreenivas and S. Mohanty, “Fibrolipoma of the Tonsil,” Indian Journal of Pathology and Microbiology, Vol. 53, No. 3, 2010, pp. 562-563.
- F. S. Derekoy, F. Huseyin, F. Fidan, F. Aktepe and O. Kahveci, “Tonsillar Lipoma Causing Difficult Intubation: A Case Report,” Kulak Burun Bogaz Ihtisas Dergisi, Vol. 17, No. 6, 2007, pp. 329-332.
- S. K. Ahn, S. Y. Jeon, J. P. Kim and S. M. Baek, “A Case of Lipoma of the Tonsil,” Korean Journal of Otolaryngol-Head Neck Surgery, Vol. 45, No. 8, 2002, pp. 831-833.
- A. A. Adoga, T. Nimkur, A. Manasshe and G. Echejoh, “Buccal Soft Tissue Lipoma in an Adult Nigerian: A Case Report and Literature Review,” Journal of Medical Case Reports, Vol. 2, No. 382, 2008. doi:10.1186/1752-1947-2-382
- J. G. Visscher, “Lipomas and Fibrolipomas of the Oral Cavity,” Journal of Maxillofacial Surgery, Vol. 10, No. 3, 1982, pp. 177-181. doi:10.1016/S0301-0503(82)80036-2
- C.-P. Wang, P.-C. Kwan and C.-Y. Ho, “Lipoma of the Palatine Tonsil,” Journal of Formosan Medical Association, Vol. 106, No. 8, 2007, pp. 673-675. doi:10.1016/S0929-6646(08)60026-1
NOTES
*Corresponding author.