Open Journal of Obstetrics and Gynecology
Vol.4 No.10(2014), Article
ID:47831,4
pages
DOI:10.4236/ojog.2014.410085
Metastatic Carcinoma of the Uterine Cervix from Rectal Carcinoma: A Case Report and Review of the Literature
Motoki Matsuura1,2, Masato Tamate1, Masahiro Suzuki1, Tasuku Mariya1, Sakura Takada1, Yuta Tabuchi1, Mizue Teramoto1, Seiro Satohisa1, Ryoichi Tanaka1, Masahiro Iwasaki1, Kaori Fukunaka3, Noriyoshi Fukunaka3, Satoshi Tanaka3, Tsuyoshi Saito1
1Department of Obstetrics and Gynecology, Sapporo Medical University, Sapporo, Japan
2Department of Obstetrics and Gynecology, Nikko Memorial Hospital, Muroran, Japan
3Department of Obstetrics and Gynecology, Hakodate Goryoukaku Hospital, Hakodate, Japan
Email: mmatsuura@sapmed.ac.jp
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 12 May 2014; revised 10 June 2014; accepted 2 July 2014
ABSTRACT
Primary adenocarcinomas of the uterine cervix account for 5% - 15% of all cervical malignancies, but secondary adenocarcinomas from extragenital cancers are rare. Only 35 cases have been reported in the literature since 1941. We report a 52-year-old Japanese woman who had been treated for rectal adenocarcinoma (Dukes C, stage IIIb) and who was diagnosed with primary uterine cervical carcinoma (FIGO stage Ib2) two years later. A radical hysterectomy was performed and the surgical specimen showed metastatic adenocarcinoma of the uterine cervix from rectal cancer without direct extension. Immunohistochemical staining was positive for cytokeratin 20 and CDX2, and negative for cytokeratin 7. Immunohistochemical staining is important for distinguishing between primary and secondary adenocarcinomas of the cervix, but histologic findings alone are not always adequate to establish the site of the primary lesion. The distinction between primary and secondary adenocarcinomas of the cervix is important for patient management and prognosis. Therefore, the possibility of metastatic adenocarcinoma should be considered whenever a diagnosis of adenocarcinoma of the cervix is received.
Keywords:Metastatic Adenocarcinoma, Cervical Cancer, Colorectal Carcinoma

1. Introduction
The incidence of primary adenocarcinoma of the uterine cervix has recently been increasing [1] [2] , and they now account for 5% - 15% of all cervical malignancies [3] . However, secondary adenocarcinomas from extragenital cancers are rare. The most common primary sites of extragenital cancers are the breast, stomach, colon, lung, kidney, and pancreas [4] -[8] . Colorectal cancer is the third most common cancer in Japan, and 15% - 20% of patients have metastatic disease at presentation [4] . However, metastatic carcinoma of the uterine cervix from colorectal carcinoma is very rare.
Here, we present a case of metastatic carcinoma of the uterine cervix from rectal carcinoma, and a review of the relevant literature.
2. Case Report
A 52-year-old, gravida 2, para 2, woman had been diagnosed with rectal adenocarcinoma (Dukes C, stage IIIb) and was treated with laparoscopy-assisted high anterior resection. She received six courses of adjuvant chemotherapy with leucovorin (LV) 250 mg/m2 intravenous (i.v.) drip infusion and 5-fluorouracil (5-FU) 600 mg/m2 as an i.v. bolus, administered weekly for 6 weeks, followed by a 2-week rest period (Figure 1(A)). She underwent an annual gynecologic examination two years later. She had no gynecologic symptoms, but the cervix was found to be replaced by a hard fixed mass, and a Papanicolaou (Pap) smear showed atypical glandular cells and a small amount of high columnar cells, suspicious for metastatic adenocarcinoma from rectal cancer. A cervical biopsy revealed a well-differentiated adenocarcinoma, with no evident primary site. She was therefore diagnosed with primary uterine cervical carcinoma (FIGO stage Ib2). The patient was referred to Hakodate Goryoukaku Hospital, and a radical hysterectomy was performed. Operative findings demonstrated severe adhesions between the uterus and the pouch of Douglas, but there was no dissemination within the peritoneum. The surgical specimen showed metastatic adenocarcinoma of the uterine cervix from rectal cancer without direct extension (Figure 1(B)). Immunohistochemical staining was positive for cytokeratin 20 and CDX2, and negative for cytokeratin 7 (Figure 1(C), Figure 1(D)). The bilateral ovaries, tubes, and endometrium were tumor-free. Computed tomography of the lungs showed a small nodule suspicious of metastasis. After surgery, the patient received chemotherapy including oxaliplatin, 5-FU, and l-LV (FOLFOX4 regimen). She remained well over the 7-year post-chemotherapy follow-up period.
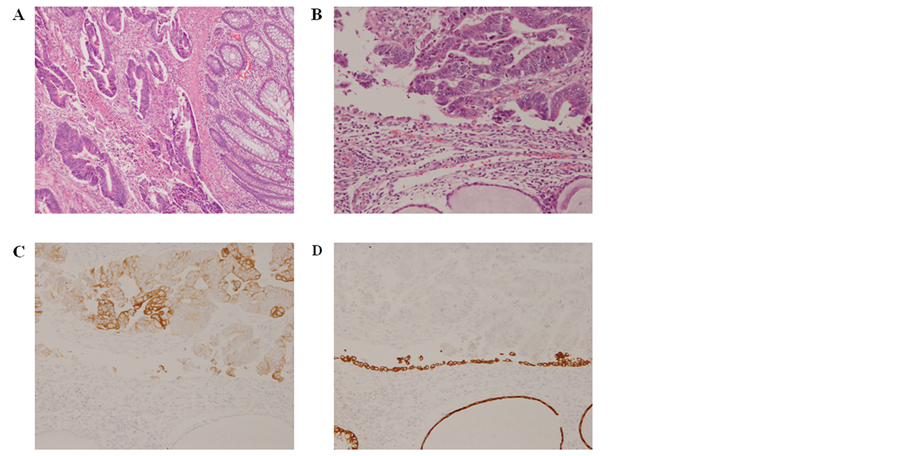
Figure 1. (A) Moderately differentiated adenocarcinoma at the primary site. Hematoxylin-eosin stain, ×10; (B) Adenocarcinoma at the metastatic site. Hematoxylin-eosin stain, ×20; (C) The malignant cells were positive for cytokeratin 20, ×20; (D) The malignant cells were negative for cytokeratin 7, ×20.
3. Discussion
Metastatic carcinoma of the uterine cervix from colorectal carcinoma is very rare, and only 35 cases have been reported in the literature since 1941 [4] -[17] . The patients’ ages ranged from 17 - 77 years [9] , with an average age of 56.5 years. Metastatic adenocarcinoma of the cervix from colorectal carcinoma has been reported to comprise only 18.5% of all secondary adenocarcinomas of the cervix [5] [8] [13] [16] [18] .
The rarity of uterine cervical metastatic adenocarcinomas has been attributed to: 1) the high fibrous tissue content of the cervix providing an unfavorable medium for metastatic growth; 2) the small size and relatively limited blood flow of the cervix as a target organ; 3) the fact that the lymphatic vessels of the pelvis all drain away from the cervix; 4) the failure to exclude possible primary sites in cases diagnosed as adenocarcinoma of the cervix; and 5) the failure to screen the cervix routinely during follow-up in women with adenocarcinomas of extragenital sites [14] . Failure to examine the cervix during autopsy may also result in an underestimation of the incidence of metastatic adenocarcinoma of the cervix [5] [6] [13] [14] [16] .
Severe adhesions in the Douglas pouch were observed in our case, but there was no direct extension and no dissemination in the peritoneum. Although both the uterine endometrium and ovaries were tumor-free, lung metastasis was observed. This suggests that the spread of the tumor to the uterine cervix in our case might have been caused by lymphatic and hematogenous spread.
Recurrence of colorectal carcinoma usually occurs within 5 years after surgery [4] . Most cases of uterine cervical metastasis from colorectal carcinoma have penetrated the wall of the bowel at the time of first surgery (Dukes stage B), or spread to the regional lymph nodes (Dukes stage C) [6] [8] . Most patients have extensive carcinoma at the time of diagnosis of the cervical metastasis.
It is difficult to determine the primary site on the basis of Pap smear results and histologic findings. However, a palisading pattern consisting of high columnar cells is a feature of Pap smears in cases of metastatic adenocarcinoma from colorectal cancer [19] . Pap smears also show clusters with anisocytosis, high N/C ratio, and prominent nucleoli [20] . Intestinal and mucinous differentiation can be detected histologically in some cases. Immunohistochemical staining is often positive for cytokeratin 20 and negative for cytokeratin 7 [16] . However, histologic findings alone are not always adequate for establishing the site of the primary lesion.
The distinction between primary and secondary adenocarcinomas of the cervix is important for patient management and prognosis [10] . Thus the possibility of metastatic adenocarcinoma should be considered whenever a diagnosis of adenocarcinoma of the cervix is received.
References
- Kim, H.S. and Underwood D. (1991) Adenocarcinomas in the Cervicovaginal Papanicolaou Smear: An Analysis of a 12-Year Experience. Diagnostic Cytopathology, 7, 119-124. http://dx.doi.org/10.1002/dc.2840070203
- Shingleton, H.M., Gore, H., Bradley, D.H. and Soong, S.J. (1981) Adenocarcinoma of the Cervix. Clinical Evaluation and Pathologic Features. American Journal of Obstetrics Gynecology, 139, 799-814.
- Buckley, C. and Fox, H. (1992) Pathology of Clinical Invasive Carcinoma of Cervix. Churchill Livingstone, Edinburgh.
- Childs, A.J., Burke, 2nd, J.J., Perry, M.Y., Check, W.E. and Gallup, D.G. (2005) Recurrent Colorectal Carcinoma Detected by Routine Cervicovaginal Papanicolaou Smear Testing. Journal of Lower Genital Tract Disease, 9, 236-238. http://dx.doi.org/10.1097/01.lgt.0000179865.98068.32
- Nakagami, K., Takahashi, T., Sugitani, K., Sasaki, T., Ohwada, S. and Morishita, Y. (1999) Uterine Cervix Metastasis from Rectal Carcinoma: A Case Report and a Review of the Literature. Japanese Journal of Clinical Oncology, 29, 640-642. http://dx.doi.org/10.1093/jjco/29.12.640
- Lemoine, N.R. and Hall, P.A. (1986) Epithelial Tumors Metastatic to the Uterine Cervix: A Study of 33 Cases and Review of Literature. Cancer, 57, 2002-2005. http://dx.doi.org/10.1002/1097-0142(19860515)57:10<2002::AID-CNCR2820571021>3.0.CO;2-L
- Korhonen, M. and Stenback, F. (1984) Adenocarcinoma Metastatic to the Uterine Cervix. Gynecologic and Obstetric Investigation, 17, 57-65. http://dx.doi.org/10.1159/000299123
- Mazur, M.T., Hsueh, S. and Gersell, D.J. (1984) Metastases to the Female Genital Tract: Analysis of 325 Cases. Cancer, 53, 1978-1984. http://dx.doi.org/10.1002/1097-0142(19840501)53:9<1978::AID-CNCR2820530929>3.0.CO;2-1
- Sozen, I., Small, L., Kowalski, M., Mayo, A.W. and Hurwitz, C.A. (2005) Adenocarcinoma of the Cervix Metastatic from a Colon Primary and Diagnosed from a Routine Pap Smear in a 17-Year-Old Woman: A Case Report. The Journal of Reproductive Medicine, 50, 793-795.
- Mulvany, N.J., Nirenberg, A. and Oster, A.G. (1996) Non-Primary Cervical Adenocarcinomas. Pathology, 28, 293-297. http://dx.doi.org/10.1080/00313029600169214
- William, P. and Abraham, M. (1962) Adenocarcinoma of the Cervix. American Journal of Obstetrics Gynecology, 84, 367-374.
- Zhang, Y.C., Zhang, P.F. and Wei, Y.H. (1983) Metastatic Carcinoma of the Cervix Uteri from the Gastrointestinal Tract. Gynecologic Oncology, 15, 287-290. http://dx.doi.org/10.1016/0090-8258(83)90084-7
- Eposito, J.M., Zarou, D.M. and Zarou, G.S. (1965) Extragenital Adenocarcinoma Metastatic to the Cervix Uteri: A Diagnostic Problem. American Journal of Obstetrics Gynecology, 92, 792-795.
- Daw, E. (1972) Extragenital Adenocarcinoma Metastatic to the Cervix Uteri. American Journal of Obstetrics Gynecology, 114, 1104-1105.
- Trastour, C., Rahili, A. and Chevallier, A. (2007) Metastasis to the Uterine Cervix from a Rectal Cancer. European Journal of Obstetrics. Gynecology and Reproductive Biology, 130, 137-138. http://dx.doi.org/10.1016/j.ejogrb.2005.12.028
- Millaire, M., Alobaid, A., Gariepy, G. and Gauthier, P. (2005) Metastatic Adenocarcinoma of the Cervix: A Case Report. Journal of Obstetrics Gynaecology, 27, 1113-1116.
- Wallach, J.B. and Edberg, S. (1959) Carcinoma Metastatic to the Uterine Cervix. American Journal of Obstetrics Gynecology, 77, 990-995.
- Kumar, N.B. and Hart, W.R. (1982) Metastases to the Uterine Corpus from Extragenital Cancers: A Clinicopathologic Study of 63 Cases. Cancer, 50, 2163-2169. http://dx.doi.org/10.1002/1097-0142(19821115)50:10<2163::AID-CNCR2820501032>3.0.CO;2-F
- Tango, M., Seto, T. and Watanabe, K. (1998) The Cellular Manifestations of Metastatic Adenocarcinoma of the Uterine Cervix. IRYO, 52, 534-538 (Japanese).
- Suzuki, T., Ito, E., Takehara, M., Koizumi, M., Takeda, T., Fukunaka, N. and Kudo, R. (1997) A Study on Cytology and Histology of Metastatic Uterine Cancer. Journal of the Japanese Society of Clinical Cytology, 36, 167-173 (Japanese). http://dx.doi.org/10.5795/jjscc.36.167