Open Journal of Psychiatry
Vol.4 No.1(2014), Article ID:41622,7 pages DOI:10.4236/ojpsych.2014.41003
Post-traumatic stress disorder among homeless adults in Poland: Prevalence and predictors
1Institute of Psychology, Opole University, Opole, Poland
2Department of Psychology, Wayne State University, Detroit, USA
3Department of Psychology, University of Windsor, Windsor, Canada
4Department of Psychology, Bowling Green State University, Ohio, USA
Email: Anna.Bokszczanin@uni.opole.pl
Copyright © 2014 Anna Bokszczanin et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In accordance of the Creative Commons Attribution License all Copyrights © 2014 are reserved for SCIRP and the owner of the intellectual property Anna Bokszczanin et al. All Copyright © 2014 are guarded by law and by SCIRP as a guardian.
Received 24 October 2013; revised 20 November 2013; accepted 28 November 2013
ABSTRACT
BACKGROUND: Symptoms of Post-Traumatic Stress Disorder (PTSD) have often been found in studies on homeless people, due to high rates of traumatic experiences. Most research on homelessness has been conducted in North America and Western Europe. However there are many social and cultural factors which can impact the prevalence and number of PTSD symptoms. AIMS: This study sought to determine the prevalence and predictors of trauma and PTSD symptoms among homeless adults in an Eastern European nation (Poland). METHOD: Randomly chosen residents of shelters were interviewed (N = 200). The respondents were asked about symptoms of PTSD, alcohol abuse/dependence, depression symptoms and perceived social support. RESULTS: The data indicated that 30% of the homeless sample were victims of traumatic events, 22% showed at least one PTSD symptom, and 7% met criteria for a lifetime diagnosis of PTSD. Symptoms of PTSD were the most common among those who had symptoms of alcohol abuse/ dependence and depression. CONCLUSION: The study’s findings support the need to attend to mental disorders such as PTSD when addressing the array of needs of homeless people.
KEYWORDS
Homelessness; PTSD; Trauma; Depression; Alcohol Use; Social Support; Poland
1. INTRODUCTION
A growing body of literature documents the high prevalence of traumatic experiences and other stressful events among homeless people [1]. For example, one study conducted in Australia demonstrated that more than 90% of homeless people reported at least one event of trauma in their life. Among the traumatic events, the most prevalent was serious physical assaults and witnessing someone being injured, raped, and/or killed [2]. A similar percentage of traumatic events, 91%, was observed in the United States by Ford and Frisman [3] in a sample of homeless women caring for children. The high rates of trauma observed among the homeless may be due to the fact that many have experienced abuse before becoming homeless as well as to the impact of living on the streets and coming from neighborhoods threatened by violence and crime [4].
The term trauma has been used to refer to a variety of symptoms commonly found among survivors of extreme stress. People who experience traumatic events but do not seek assistance are at risk of developing Post-Traumatic Stress Disorder (PTSD) [1-4]. For instance, Ford and Frisman [3] documented that, among homeless women, 30% met the criteria for a diagnosis of PTSD. Investigations on the prevalence of PTSD among samples of homeless youth in the United States have found that 24% - 38% of the respondents could be diagnosed as exhibiting PTSD [5]. These results are much higher than the PTSD prevalence in the general population in the US [6]. To our knowledge, no study has yet assessed the prevalence of trauma and PTSD among homeless persons in Poland.
Exposure to traumatic events and homelessness has also been associated with other negative mental health outcomes, including depression [5]. Studies have found that, overall, homeless individuals suffer from depression at substantially higher rates than members of the general population, with exposure to traumatic events increasing the risk for developing PTSD [7]. However, data from Poland show that only 3% of homeless adults suffer depression, but 60% are alcohol addicted [8,9].
Substance abuse, especially alcohol, is a known factor correlated with PTSD symptoms. One recent study found that substance abuse behaviors were directly and indirectly predicted by many psychosocial and situational factors observed among homeless individuals [10]. Bender and colleagues [5] identified that alcohol addiction significantly predicted PTSD symptomatology in homeless youth. Alcohol abuse may be either an antecedent or a consequence of trauma exposure and PTSD symptom development. Researchers have suggested several possible explanations for the relationship between alcohol abuse and trauma symptoms in homeless individuals. For example, alcohol abuse can be a way of coping with trauma by dampening already existing symptoms [10, 11].
While in the research literature much attention has been paid to examine the impact of victimization on mental health problems, there is very little known about factors which protect against the development of negative mental health symptoms in homeless adults [12]. Social support may be one of the most important agents protecting against the development of PTSD. A particularly important role is attributed to perceived social support, which refers to the help victims expect or hope to receive. Such a conviction is based on a subjective assessment of the resilience of networks and sources of support, which implies that support from loved ones will be available during times of need [13]. Although investigations on the protective effect of social support among minority groups, poor people, and the homeless are relatively rare, Toro, Tulloch, and Ouellette [14] found consistent main and stress-buffering effects of perceived social support on psychological symptoms in two samples of homeless adults in the United States.
Only a few systematic research studies have been conducted on the homeless in Poland [15,16]. One of the most extensive studies was conducted by sociologists who surveyed homeless people in the Pomeranian region. In the research, 2470 homeless adults were examined; the results indicated that the average Polish homeless individual is a man, aged 51 to 60. Only 60% of homeless adults used public assistance, and 90% were unemployed. Nearly half of the respondents usually stayed in a shelter for homeless people (48.3%). The homeless population is heterogeneous: thus, we have homeless mothers with children fleeing domestic violence and we have some with a university degree with a history working in powerful management companies who have become homeless as a result of personal, economic, and/or family problems [15].
Toro and colleagues [17] interviewed random samples of adults in Poland, United Kingdom, Germany, the United States, Italy, and other developed nations by telephone. The interview consisted of 128 items assessing experience with homelessness as well as attitudes and beliefs. Two indices of homelessness were used: 1) literal homelessness (i.e., having spent at least one night on the streets, in a shelter, or public place) and 2) total homelessness (which also includes staying with friends or family or being precariously housed). The results indicated that the United States and the United Kingdom had the highest rates of total lifetime homelessness, with somewhat lower rates in Italy, Belgium, and Poland; and the lowest rate in Germany. A similar pattern emerged among lifetime literal homelessness. The rate of homelessness in Poland was surprisingly low, despite it being the poorest of the nations studied. This may be a result of the strong sense of family and community among Poles. Many who might otherwise be homeless live with relatives. Poles scored low on compassion and trust and high on limiting the public rights of the homeless. Although Poles believed the government was responsible for homelessness, they also attributed homelessness to individuals’ personal failings. The tendency for Poles to blame the state and the individual for homelessness may be a residual attitude from the communist era, where the state provided for everyone [18].
The present research attempted to 1) estimate the prevalence of trauma, PTSD symptoms, and the diagnosis of PTSD among homeless adults in Poland, 2) identify differences between homeless individuals who have experienced trauma and those who have not, and 3) determine predictors of PTSD symptoms among homeless individuals. We hypothesized that the rate of PTSD among the homeless would be high based on data from other countries [2] and a variety of factors, including negative public attitudes toward homeless people in Poland [18,19]. We also expected more alcohol abuse, more depression symptoms, and less perceived social support in those with more PTSD symptoms.
2. METHOD
2.1. Procedure
The interviews took place in 34 different sites. These 34 sites comprised virtually all of the known places where significant numbers of homeless adults could be found in the region. A group of trained graduate students in psychology interviewed the participants. Interviews lasted 1.5 to 3 hours each and were conducted at the service setting in a private area. Participation in the research was completely voluntary and each respondent received 10 zloties (about $4.00 US) for the interview. Written consent was obtained from each respondent before the interview began. The interviews took place over an 18-month period (January 2005 through June 2006).
2.2. Participants
Participants were randomly chosen from lists of residents in shelters in the Opole and Wroclaw regions of southern Poland (with general populations of 1.0 and 2.9 million people), respectively [18]. The mean age of the respondents was 47, with a range from 18 to 75 years. The sample consisted mostly of males (72.5%; see Table 1). All but two of the participants were of Polish ethnicity (there was one Ukrainian and one Romanian). Most (61.0%) had been homeless (current episode) for more than 36 months, with many others (32.5%) homeless for 6 - 36 months, and few (6.5%) homeless for less than 6 months. Across all these basic characteristics, the present sample appeared similar to samples of homeless people from a few other existing studies done elsewhere in Poland [15].
2.3. Measures
Background characteristics. Various questions assessed the respondent’s age, educational attainment, and how many children the respondent had.
Symptoms of post-traumatic stress. The Polish adaptation of The PTSD Interview [20], as developed by Koniarek, Dudek, and Szymaczak [21] was used. This scale has been used in a variety of populations including medical trauma victims, auto accident trauma victims, fireman, policemen, and sexually and physically assaulted women [22]. In the review of PTSD scales Norris and Hamblen [23] characterized this scale as flexible in scoring, reliable, and valid. This scale includes 2 questions about traumatic event(s) (Criterion A), 17 questions about PTSD Criterion symptoms (5 on Criterion B, 7 on Criterion C, and 5 on Criterion D), and 2 questions about the current/lifetime course of the PTSD symptoms (Criteria E and F). Respondents were asked how often they experienced traumatic reactions related to the event, where: 1 = never; 2 = very rarely, 3 = sometimes, 4 = somewhat often, 5 = very often, 6 = always. The following is an example item (symptom B2): “Have you had recurring unpleasant dreams about (the trauma)?” A continuous symptom count of post-traumatic stress were created by summing the number of affirmative responses to all symptoms (B, C, and D, range = 0 - 17) with a cutoff = 3 for each symptom to produce an optimal sensitivity/specificity balance (alpha = 0.89).
Alcohol abuse/dependence. This measure was a part of a structured diagnostic interview (DIS) that yields current and lifetime estimates of various psychiatric disorders based on DSM-III-R criteria. The DIS has been used in a variety of earlier studies on homeless adults [24]. The total number of symptoms of alcohol abuse and de-
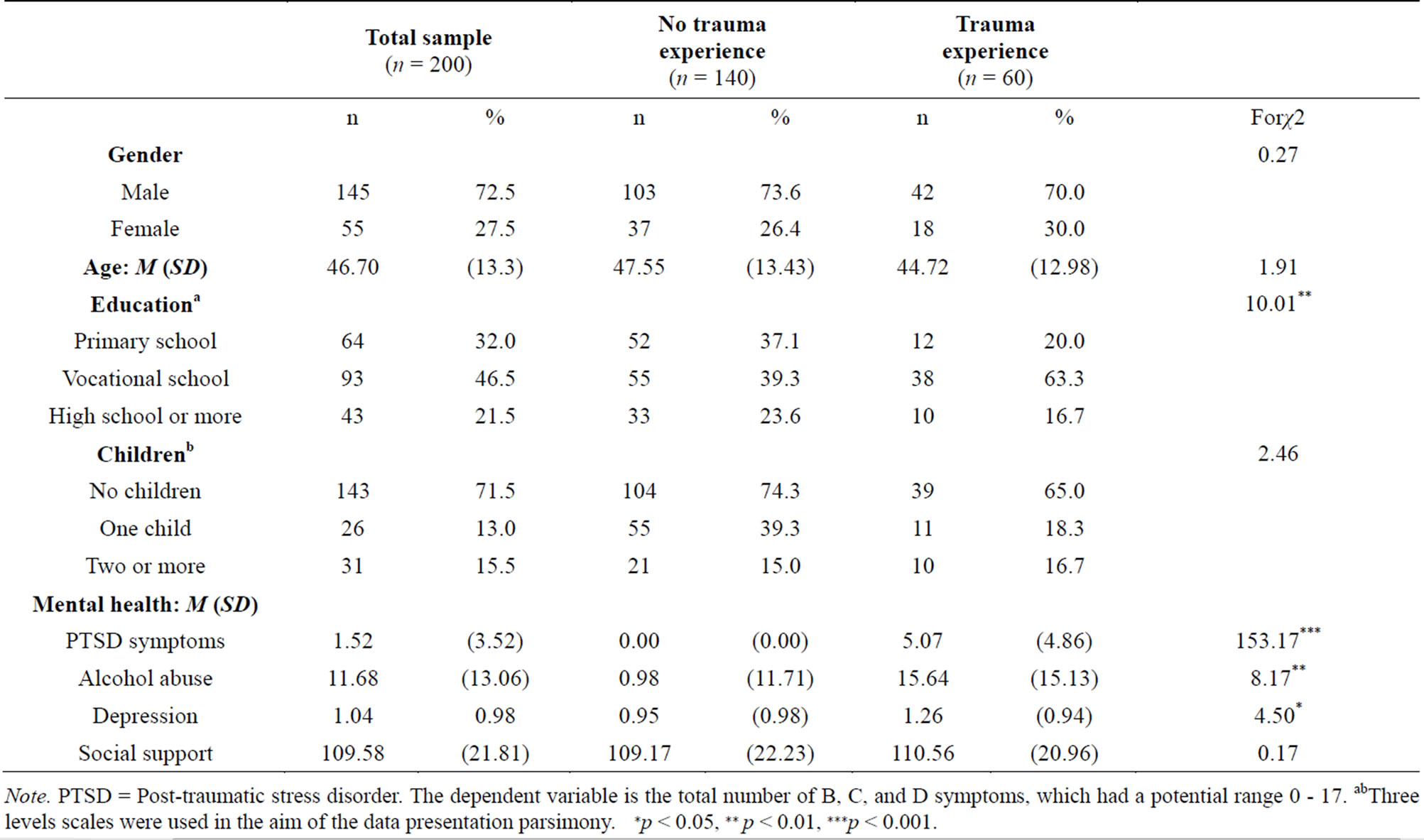
Table 1. Sample characteristics and differences between no trauma, and trauma groups.
Note. PTSD = Post-traumatic stress disorder. The dependent variable is the total number of B, C, and D symptoms, which had a potential range 0 - 17. abThree levels scales were used in the aim of the data presentation parsimony. ∗p < 0.05, ∗∗ p < 0.01, ∗∗∗p < 0.001.
pendence was used here.
Depression. The Brief Symptom Inventory (BSI) [25] subscale measuring depression symptoms was used. Each of the 6 raw depression items was rated on a 5-point scale to indicate the degree to which the symptom has been experienced during the preceding two weeks. The mean across the relevant items was used here (alpha = 0.76). This measure has been used in several earlier studies and has satisfactory validity and reliability [14,26].
Perceived social support. The Interpersonal Support Evaluation List (ISEL) is a 40-item questionnaire in which people are asked to rate the perceived availability of different types of social support. As in recent studies on homeless and poor people [14,27], a 4-point rating scale was used on each item, rather than the original dichotomous format. The ISEL consists of four subscales tapping different types of support (i.e., tangible, self-esteem, belonging, and appraisal) as well as a total score. The Polish version was abridged to 38 items, due to cultural differences making translation difficult for 2 items. The four ISEL subscales have demonstrated testretest reliabilities of 0.71 - 0.87 in various community samples [26] and 0.62 to 0.85 in a sample of homeless and poor adults [25]. Bates and Toro [27] also found that the ISEL subscales were associated with various outcomes (e.g., symptoms of physical and psychological symptoms). Because of the substantial correlations among the four ISEL subscales (ranging from 0.46 to 0.62 in our sample) and the wish to reduce the number of predictors in the main analyses, the total ISEL score was used.
3. RESULTS
Thirty percent of respondents (42 men, 18 women) in the total sample of 200 reported experiencing one or more traumatic event (both unusual and severe) in their life, with 14% (16 men, 11 women) experiencing such events more than once (Criterion A). Reported traumatic events primarily included being a victim of or witnessing beatings, physical assault, and fires. Twenty-two percent (29 men, 15 women) reported PTSD symptoms, which means that they had at least one Criterion symptom (B, C, or D) that met the cut-off score of 3. Only 7% (8 men, 6 women) met all criteria for a PTSD diagnosis (Criterion A, at least one Criterion B symptom, at least three Criterion C symptoms, and at least two Criterion D symptoms). Three percent of persons (3 men, 2 women) received a current diagnosis of PTSD.
Several significant differences were found between the group of 60 that had one or more traumatic events and the 140 that had none. The group that had ever experienced a traumatic event had different educational outcomes: among those with trauma, there were fewer with a primary school education only, more who had achieved only a vocational level of education, and fewer who had completed high school. The group who experienced trauma also reported higher levels of symptoms of depression, alcohol abuse/dependence, and PTSD (Table 1).
Hierarchical regression analysis was used to predict the number of PTSD symptoms among the study participants. The results of this analysis are presented in Table 2. Four individual characteristics (i.e., gender, age, level of education, and number of dependent children) were entered in the first step of the regression analysis. None of these characteristics significantly explained the variance in PTSD symptoms. Perceived social support was entered in the second step did not predict additional variance in PTSD symptoms (after controlling for the other variables already in the regression equation). Factors related to alcohol abuse and depression symptoms were introduced simultaneously in the third step and they together explained a significant part of the variance in the symptoms. The levels of statistical significance for beta coefficients indicated that each of the variables had an independent main effect on the number of PTSD symptoms.
4. DISCUSSION
This study’s primary aim was to estimate the prevalence of trauma and symptoms relevant for the diagnosis of PTSD. One third of respondents reported having experienced at least one traumatic event in their lifetime but only 7% of them had developed a full-blown diagnosis of PTSD. The observed proportion of traumatic events and PTSD diagnosis experienced by homeless people in Poland seems lower, as compared to what has been observed
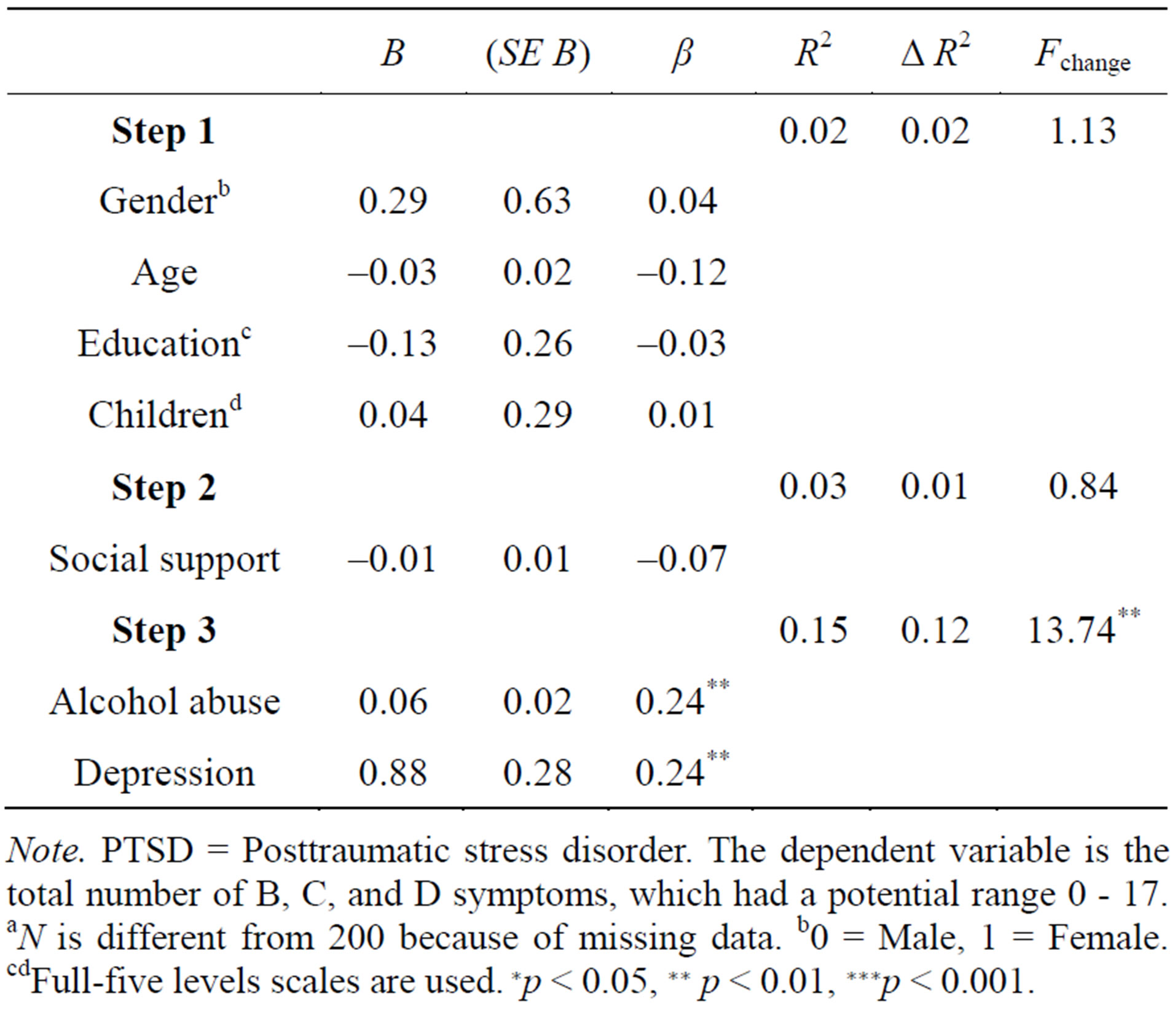
Table 2. PTSD criterion symptoms: results of hierarchical regression analyses (N = 195)a.
Note. PTSD = Posttraumatic stress disorder. The dependent variable is the total number of B, C, and D symptoms, which had a potential range 0 - 17. aN is different from 200 because of missing data. b0 = Male, 1 = Female. cdFull-five levels scales are used. ∗p < 0.05, ∗∗ p < 0.01, ∗∗∗p < 0.001.
in several studies on homeless people in other countries [2,3]. The low rates of traumatic events and PTSD diagnosis among homeless people found in this study, as compared to studies in other nations, may be related to certain differences in the basic characteristics of homeless adults in Poland as compared to other nations. Our Polish homeless group was composed mostly of men who had lived in shelters for relatively long time periods of time. Most of our sample (61%) had been homeless for over 3 years, as compared with much smaller numbers found in studies in other nations. For example, Toro et al. [14] found, in two different US cities, that only 10% and 26% were homeless for over 3 years. We can speculate, then, that homeless shelters in Poland may represent a relatively “stable” place in which people after a variety of stressful experiences find not only a place to stay, but also a psychological sense of security. Some support for this speculation comes from the research among homeless persons in shelters conducted by Perron and colleagues [12]. The study examined the influence of victimization on depressive symptoms in over 9600 homeless and mentally ill adults in the United States. They found that the relationship between violent events experienced by the homeless and depression was mediated by an individual’s perceived safety: a greater feeling of safety was related to lower levels of depression symptoms in homeless individuals. Further study carried out among Polish homeless persons living in shelters, with the measurement of sense of security, could show whether this sort of mediation might also occur in Poland in relation to symptoms of PTSD.
Nonetheless, the rate of PTSD diagnosis in our sample was comparable to what was found in studies conducted by Dudek [21] in Poland using the same PTSD questionnaire in samples of persons at high risk for developing PTSD: i.e., policemen, firefighters, and paramedics. The highest rate of PTSD found by Dudek was 4.8% among paramedics [22]. Perhaps, low levels of PTSD in our study may be partly due to underestimation of PTSD associated with the measurement tool used. Watson and colleagues [20] noted that in clinical settings the PTSDDIS functioned well, however, Kulka et al. [28] indicated that when used in a community sample, the obtained base rate of PTSD was low.
The second aim was to identify differences between homeless individuals who have experienced trauma and those who have not. Consistent with our expectations, we found several mental health characteristics were associated with having experienced trauma. Those with a history of trauma experience were more likely to develop PTSD symptomatology, and had more depression and alcohol abuse symptoms. Exposure to traumatic events can often result in mental health problems. Intense fear, shock, and losses associated with trauma could have a long-term psychological impact on a person’s mental health and behaviors, even though he/she may not develop PTSD symptomatology [7]. Over-represented among those with traumatic events were people with PTSD symptoms. In fact, PTSD diagnose require that the respondent have experienced at least one traumatic event and response involving intense fear, helplessness, or horror. The reasons why some people develop PTSD symptomatology after traumatic events and others has not also been considered in previous studies. Various factors can determine developing PTSD: threat experienced during the event, personal traits, family mental health history, received social support, and many others [29]. The higher levels of depression and alcohol abuse symptoms found in the trauma group is not surprising and is consistent with other studies involving homeless samples [5]. In summary, the results of our comparisons of homeless with and without traumatic experiences have shown much worse functioning of the previous group, i.e. they consume more alcohol, are more depressed, and exhibit detrimental symptoms of intrusion, avoidance, and arousal.
The last goal of our study was to determine predictors of PTSD symptoms among homeless individuals. The hierarchical regression equation included four sociodemographic predictors (gender, age, education level, and number of dependent children) and three mental health predictors (social support, alcohol abuse/dependence, and depression symptoms. None of the sociodemographic variables was not statistically significant, and our expectation that perceived social support would be a protective factor against PTSD development was also not confirmed. We only assessed the overall level of perceived support. Further studies may wish to consider not only perceived but also other types of social support, such as support actually received or the support provided. Future research could also include social support from a variety of sources—from friends, family, and other people living at the shelter, and the staff from care centers for the homeless [30]. However, available descriptions of the situation of persons living in homeless shelters in Poland leave no illusions—they are people with low social support. Analysis of the family situations of homeless women showed that most had no family contact because of conflicts within the family [16]. Furthermore, families of homeless people themselves often lack material resources and have little to offer to their homeless relatives [31].
It should be pointed out that two factors, i.e., alcohol abuse/dependence and depression symptoms, explained separately significant portions of the variation in PTSD symptoms above and beyond the influence of the socio-demographic variables and perceived social support. While the findings concerning alcohol abuse/dependence symptoms are consistent with other studies, our crosssectional data do not indicate the direction of the relationship between such symptoms and PTSD symptoms. As noted earlier, it could be that having problems with alcohol abuse and/or dependence could put one at risk for the development of PTSD symptoms; it is also possible that persons with PTSD symptoms attempt to “selfmedicate” to escape the pain of their symptoms. Of course, this is not an effective strategy in the long run, as it often leads to more serious substance abuse problems that may ultimately exacerbate the PTSD symptoms rather than alleviate them.
A relatively consistent finding across several studies is that the number of depression symptoms is correlated with a higher level of PTSD symptoms. Trauma survivors can develop only depression, PTSD, or both disorders. In our study, depression symptoms explained the greatest part of the variance in PTSD symptoms, even after controlling for prior variables in the regression equation. These findings suggest a high degree of shared psychopathology between the two disorders of PTSD and depression.
5. CONCLUSIONS
The study’s findings have a number of implications for intervention. First, the results suggest the need for complex interventions to address PTSD symptoms. Depression symptoms, alcohol addiction, and problems with social relations that often co-occur with PTSD may complicate treatment efforts. An integrative approach in the treatment of PTSD is already present in some community-based programs [11] and should be considered in other programs. Our results suggest that interventions aimed at helping homeless trauma survivors should, aside from attending to basic clinical concerns, also take into account psycho-educational activities. Actions aimed at raising the level of education among the homeless could be a useful contributor to protecting against chronic symptoms of distress and to strengthening resilience [26].
The present research has its limitations, including a relatively small number of participants (N = 200) from a specific region in Poland. The study’s correlational nature does not allow for inferences about causality. This study also had some strengths. First, the random sample of homeless individuals allows us to make reasonable guesses about the characteristics of the homeless population, at least in the region studied. The present study was largely exploratory in nature and is but a first step in the study of trauma and PTSD among homeless people in Poland.
FUNDING
This Funding for this research came from the University of Opole (in Poland) and Wayne State University (in the US).
REFERENCES
- Kushel, M.B., Evans, J.L., Perry S., Robertson, M.J. and Moss, A.R. (2003) No door to lock: Victimisation among homeless and marginally housed persons. Archives of International Medicine, 163, 2492-2499. http://dx.doi.org/10.1001/archinte.163.20.2492
- Buhrich, N., Hodder, T. and Teesson, M. (2000) Lifetime prevalence of trauma among homeless people in Sydney. Australian and New Zealand Journal of Psychiatry, 34, 963-966. http://dx.doi.org/10.1080/000486700270
- Ford, J.D. and Frisman, L. (2002) Traditional and complex PTSD in homeless parents and adults with chronic addictions. Proceedings of the Annual Meeting of the International Society for Traumatic Stress Studies, 18, 57.
- Clarke, P.N., Williams, C.A., Percy, M.A. and Kim, Y.S. (1995) Health and life problems of homeless men and women in the Southeast. Journal of Community Health Nursing, 12, 101-110. http://dx.doi.org/10.1207/s15327655jchn1202_4
- Bender, K., Ferguson, K., Thompson, S., Komlo, Ch. and Pollio, D. (2010) Factors associated with trauma and Posttraumatic Stress Disorder among homeless youth in three US cities: The importance of transience. Journal of Traumatic Stress, 23, 161-168.
- Kim, M.M. and Ford, J.D. (2006) Trauma and posttraumatic stress among homeless men: A review of current research. Journal of Aggression, Maltreatment & Trauma, 13, 1-22. http://dx.doi.org/10.1300/J146v13n02_01
- Wenzel, S.L., Koegel, P. and Gelberg, L. (2000) Antecedents of physical and sexual victimization among homeless women: A comparison to homeless men. American Journal of Community Psychology, 28, 367-390. http://dx.doi.org/10.1023/A:1005157405618
- Sidorowicz, S., Sanecka, B., Ślepecka, J. and Ruciński, K. (1986). Czy bezdomność jest problemem dla opieki psychiatrycznej? [Is homelessness a problem for mental health care?]. Psychiatria Polska, 4.
- Sidorowicz, S., Sanecka, B., Ślepecka, J. and Ruciński, K. (1989) Alkoholizm wśród osób bezdomnych [Alcoholism among homeless]. In: Z. Bizoń and W. Szyszkowski, Eds., Zagadnienia Alkoholizmu i Innych Uzależnień, Państwowe Wydawnictwo Naukowe, Warszawa.
- Stein, J.A., Dixon, E.L. and Nyamathi, A.M. (2008) Effects of psychosocial and situational variables on substance abuse among homeless adults. Psychology of Addictive Behavior, 22, 343-356. http://dx.doi.org/10.1037/0893-164X.22.3.410
- Yeater, E.A., Austin, J.L., Green, M.J. and Smith, J.E. (2010) Coping mediates the relationship between posttraumatic stress disorder (PTSD) symptoms and alcohol use in homeless, ethnically diverse women: A preliminary study. Psychological Trauma: Theory, Research, Practice and Policy, 2, 307-310. http://dx.doi.org/10.1037/a0021779
- Perron, B., Alexander-Eitzman, B., Gillespie, D.F. and Pollio, D. (2008) Modeling victimization among homeless persons with serious mental illnesses. Social Science and Medicine, 67, 1475-1479. http://dx.doi.org/10.1016/j.socscimed.2008.07.012
- Barrera, M. (1986) Distinctions between social support concepts, measures, and models. American Journal of Community Psychology, 14, 413-445. http://dx.doi.org/10.1007/BF00922627
- Toro, P., Tulloch, E. and Ouellette, N. (2008) Stress, social support, and outcomes in two probability samples of homeless adults. Journal of Community Psychology, 36, 483-498. http://dx.doi.org/10.1002/jcop.20190
- Dębski, M. and Olech, P. (2005) Socjodemograficzny portret zbiorowości ludzi bezdomnych Województwa Pomorskiego (raport z badań). [Socio-demographic portrait of the homeless population from the Pomeranian province (Research Report)]. Gdańsk, Pomost.
- Szajerska, A. (2007) Reintegracja społeczno zawodowa bezdomnych kobiet na przykładzie mieszkanek schronisk w województwie kujawsko-pomorskim w latach 2004- 2006 [Professional and social reintegration of homeless women on the example of women living in shelters in Kujawsko-Pomorskie, in the years 2004-2006]. In: M. Dębski and K. Stachura, Eds., Oblicza Bezdomności, 246- 247. http://www.pfwb.org.pl/wp-content/uploads/2009/11/1.1.-Raport-BadanieSocjodemograficzne-2005-Samodzielnie.pdf
- Toro, P.A., Tompsett, C.J., Lombardo, S., Philippot, P., Nachtergael, H., Galand, B., Schlienz, N., Stammel, N., Yabar, Y., Blume, M., MacKay, L. and Harvey, K. (2007) Homelessness in Europe and North America: A comparison of prevalence and public opinion. Journal of Social Issues, 63, 505-524. http://dx.doi.org/10.1111/j.1540-4560.2007.00521.x
- Bokszczanin, A., Hobden, K.L. and Toro, P.A. (2006) Homelessness and public opinion: A comparison across four nations. Society for Community Research & Action 10th Biennial Conference 2005, Urbana, Poster Presentation.
- GUS, Departament Statystyki Społecznej [Department of Social Statistics] (2007) Wyniki badań GUS. Podstawowe dane dotyczące rozwoju demograficznego Polski do 2006 roku [GUS Survey Results: Basic data on Polish demographic trends through 2006]. GUS, Warszawa.
- Watson, Ch., Tuba, M.P., Manifold, V., Kucala, T. and Anderson, P.E.D. (1991) The PTSD interview: Rationale, description, reliability, and concurrent validity of a DSMIII-based technique, Journal of Clinical Psychology, 47, 179-188. http://dx.doi.org/10.1002/1097-4679(199103)47:2<179::AID-JCLP2270470202>3.0.CO;2-P
- Koniarek, J., Dudek, B. and Szymczak (2000) Kwestionariusz do pomiaru zaburzeń po stresie urazowym (H-PTSD) —Zastosowanie PTSD—Interview Ch. Watsona i jego współpracowników w badaniach grupowych. [Questionnaire to measure traumatic stress disorder after (H-PTSD), the use of PTSD-Interview Ch. Watson and his colleagues in the study group]. Przegląd Psychologiczny, 43, 205-216.
- Dudek, B. (2003) Zaburzenie po stresie traumatycznym. [Posttraumatic stress disorder]. Gdańskie Wydawnictwo Psychologiczne, Gdańsk.
- Norris, F.H. and Hamblen, J. (2004) Standardized selfreport measures of civilian trauma and PTSD. In: J. P. Wilson, T. M. Keane and T. Martin, Eds., Assessing Psychological Trauma and PTSD, Guilford Press, New York.
- Toro, P.A. (1998) Homelessness. In: A. Bellack and M. Hersen, Eds., Comprehensive Clinical Psychology: Applications in Diverse Populations, Pergamon, New York, 119-135. http://dx.doi.org/10.1016/B0080-4270(73)00165-6
- Derogatis, L.R. (1977) SCL-90-R (revised version) manual I. Johns Hopkins University School of Medicine, Baltimore.
- DeRoon-Cassini, T.A., Mancini, A.D., Rusch, M.D. and Bonanno, G.A. (2010) Psychopathology and resilience following traumatic injury: A latent growth mixture model analysis. Rehabilitation Psychology, 55, 1-11. http://dx.doi.org/10.1037/a0018601
- Bates, D. and Toro, P. (1999) Developing measures to assess social support among homeless and poor people. Journal of Community Psychology, 27, 137-156. http://dx.doi.org/10.1002/(SICI)1520-6629(199903)27:2<137::AID-JCOP3>3.0.CO;2-B
- Kulka, R.A., Schlenger, W.E., Fairbank, J.A., Jordan, B.K., Hough, R.L., Marmar, C.R. and Weiss, D.S. (1991) Assessment of posttraumatic stress disorder in the community: Prospects and pitfalls from recent studies of Vietnam veterans. Psychological assessment. Journal of Consulting and Clinical Psychology, 3, 547-560.
- Ozer, E.J., Best, S.R., Lipsey, T.L. and Weiss, D.S. (2003) Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychological Bulletin, 129, 52-73. http://dx.doi.org/10.1037/0033-2909.129.1.52
- Marra, J., McCarthy E., Lin, H., Ford, J.D., Rodis, E. and Frisman, L.K. (2009) Effects of social support and conflict on parenting among homeless mothers. American Journal of Orthopsychiatry, 79, 348-356. http://dx.doi.org/10.1037/a0017241
- Shinn, M., Weitzman, B.C., Stojanovic, D., Knickman, J. R., Jimenez, L., Duchon, L., James, S. and Krantz, D.H. (1998) Predictors of homelessness among families in New York City: From shelter request to housing stability. American Journal of Public Health, 88, 1651-1657. http://dx.doi.org/10.2105/AJPH.88.11.1651