Congenital Unilateral Hypoplasia of the Orbicularis Oris Muscle:
A Rare Cause of Congenital Unilateral Upper Lip Palsy
66
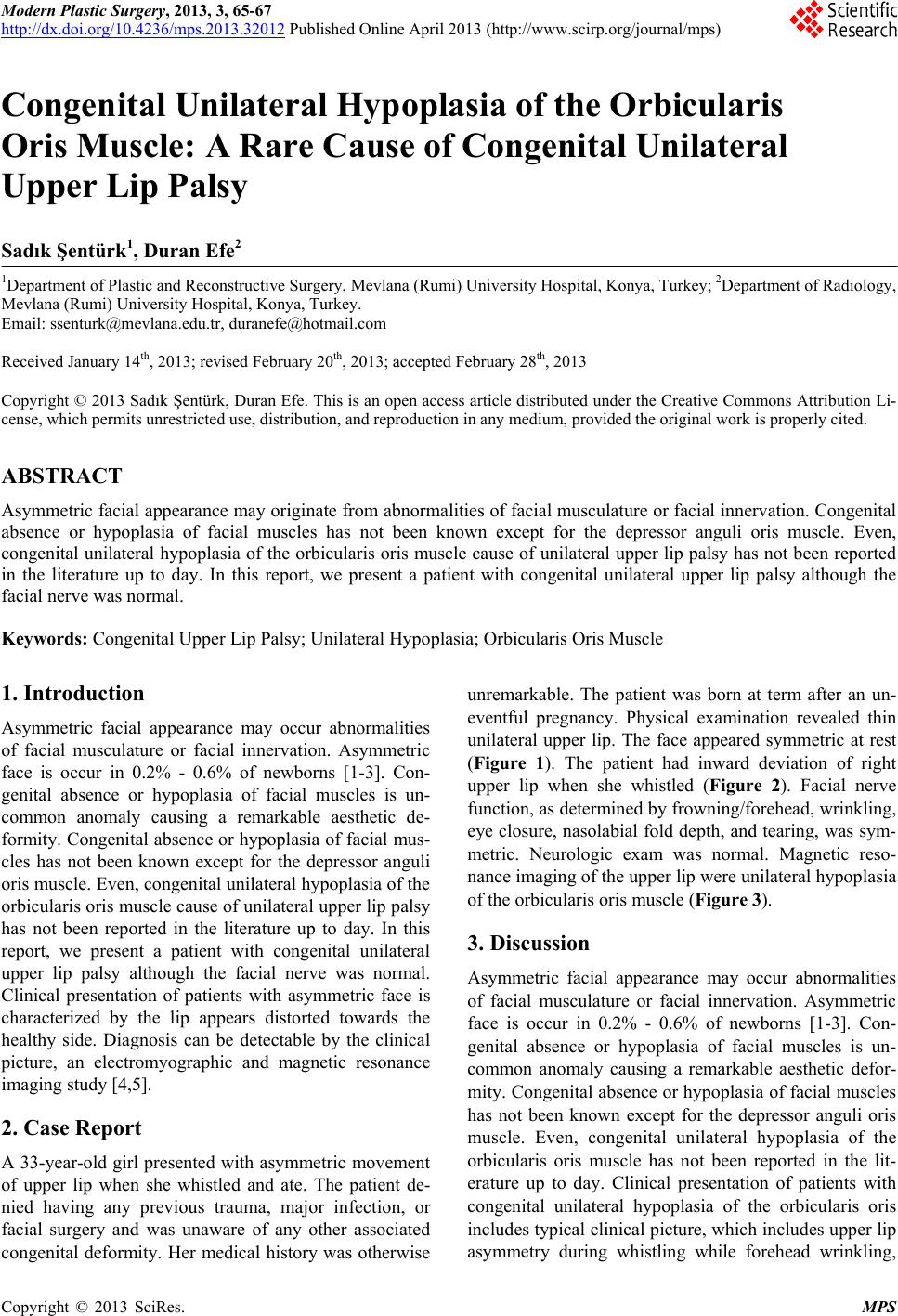
Figure 1. Patient with right-sided asymmetric upper lip at
rest.
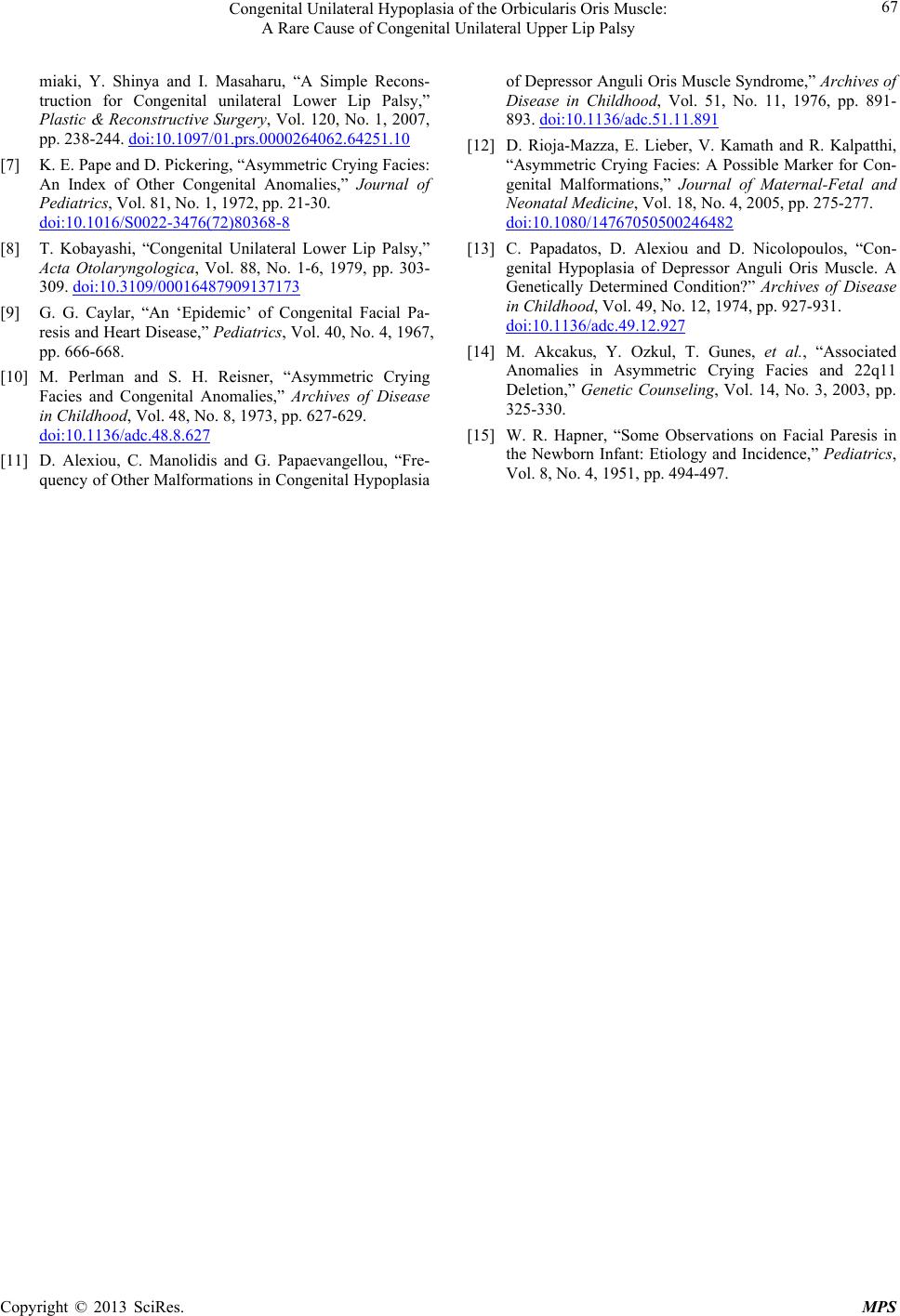
Figure 2. The upper lip is pulled toward the intact left side.
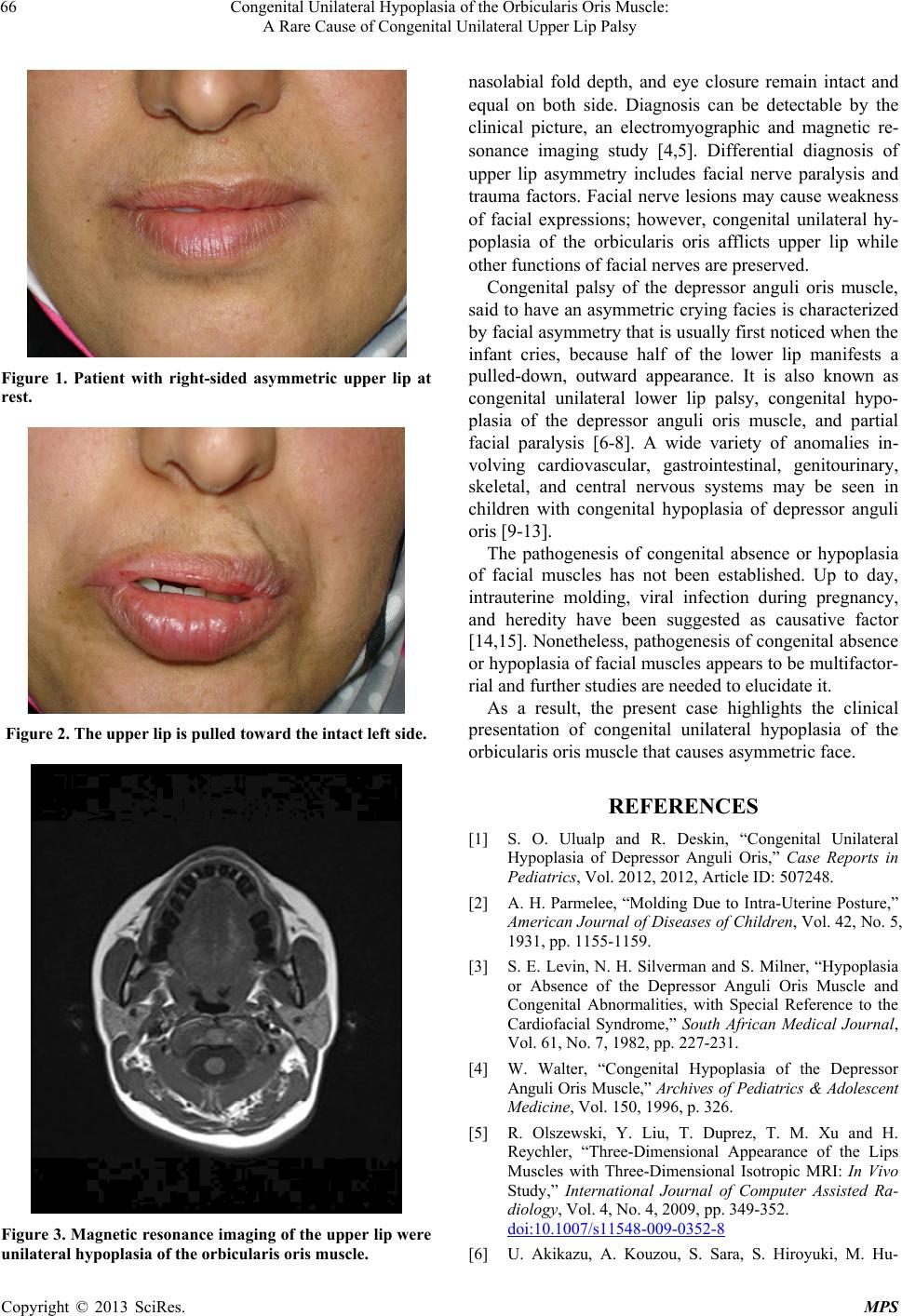
Figure 3. Magnetic resonance imaging of the upper lip were
unilateral hypoplasia of the orbicularis oris muscle.
nasolabial fold depth, and eye closure remain intact and
equal on both side. Diagnosis can be detectable by the
clinical picture, an electromyographic and magnetic re-
sonance imaging study [4,5]. Differential diagnosis of
upper lip asymmetry includes facial nerve paralysis and
trauma factors. Facial nerve lesions may cause weakness
of facial expressions; however, congenital unilateral hy-
poplasia of the orbicularis oris afflicts upper lip while
other functions of facial nerves are preserved.
Congenital palsy of the depressor anguli oris muscle,
said to have an asymmetric crying facies is characterized
by facial asymmetry that is usually first noticed when the
infant cries, because half of the lower lip manifests a
pulled-down, outward appearance. It is also known as
congenital unilateral lower lip palsy, congenital hypo-
plasia of the depressor anguli oris muscle, and partial
facial paralysis [6-8]. A wide variety of anomalies in-
volving cardiovascular, gastrointestinal, genitourinary,
skeletal, and central nervous systems may be seen in
children with congenital hypoplasia of depressor anguli
oris [9-13].
The pathogenesis of congenital absence or hypoplasia
of facial muscles has not been established. Up to day,
intrauterine molding, viral infection during pregnancy,
and heredity have been suggested as causative factor
[14,15]. Nonetheless, pathogenesis of congenital absence
or hypoplasia of facial muscles appears to be multifactor-
rial and further studies are needed to elucidate it.
As a result, the present case highlights the clinical
presentation of congenital unilateral hypoplasia of the
orbicularis oris muscle that causes asymmetric face.
REFERENCES
[1] S. O. Ulualp and R. Deskin, “Congenital Unilateral
Hypoplasia of Depressor Anguli Oris,” Case Reports in
Pediatrics, Vol. 2012, 2012, Article ID: 507248.
[2] A. H. Parmelee, “Molding Due to Intra-Uterine Posture,”
American Journal of Diseases of Children, Vol. 42, No. 5,
1931, pp. 1155-1159.
[3] S. E. Levin, N. H. Silverman and S. Milner, “Hypoplasia
or Absence of the Depressor Anguli Oris Muscle and
Congenital Abnormalities, with Special Reference to the
Cardiofacial Syndrome,” South African Medical Journal,
Vol. 61, No. 7, 1982, pp. 227-231.
[4] W. Walter, “Congenital Hypoplasia of the Depressor
Anguli Oris Muscle,” Archives of Pediatrics & Adolescent
Medicine, Vol. 150, 1996, p. 326.
[5] R. Olszewski, Y. Liu, T. Duprez, T. M. Xu and H.
Reychler, “Three-Dimensional Appearance of the Lips
Muscles with Three-Dimensional Isotropic MRI: In Vivo
Study,” International Journal of Computer Assisted Ra-
diology, Vol. 4, No. 4, 2009, pp. 349-352.
doi:10.1007/s11548-009-0352-8
[6] U. Akikazu, A. Kouzou, S. Sara, S. Hiroyuki, M. Hu-
Copyright © 2013 SciRes. MPS