Advances in Computed Tomography, 2013, 2, 20-22
http://dx.doi.org/10.4236/act.2013.21004 Published Online March 2013 (http://www.scirp.org/journal/act)
Giant Calcified Renal Artery Aneurysm: Traditional RX
versus Thr ee-Dimensional Computed Tomography
Mauro Gacci1, Omar Saleh1, Annalisa Mantella1, Leonidas Azas2, Paola Romagnani3,
Andrea Minervini1, Sergio Serni1, Marco Carini1
1Department of Urology, University of Florence, Florence, Italy
2Department of Vascular Surgery, University of Florence, Florence, Italy
3Excellence Center for Research, Transfer and High Education (DENOTHE), University of Florence, Florence, Italy
Email: os11nov@hotmail.com
Received November 7, 2012; revised December 16, 2012; accepted December 26, 2012
ABSTRACT
A 65-year-old woman with no history of previous flank trauma, renal stone or upper urinary tract infections, presented
for flank pain and left hydro-uretero-nephrosis seven days after hysterectomy. Percutaneous pielography revealed nar-
rowing of the distal ureter, without endoureteral mass. The plain abdomen film incidentally showed a 3-cm calcified
ring on the left renal shadow, who resulted external to the collecting system at pielography. A 3-dimensional-CT scan
with angiographic reconstruction revealed a 3-cm calcified renal artery aneurysm. The vascular surgeon suggested a
watchful waiting. The patient underwent ur eteral reimplantation with ureteral stenting, allowing a co mplete recovery of
iatrogenic stenosis two months postoperatively.
Keywords: Renal Artery Aneurysm; 3D-CT; Angiographic Reconstruction
1. Introduction
Renal artery aneurysms have been encountered with
increasing frequency over the past decade. It is slightly
more common in women than men and in the right than
left renal artery [1]. Many cases are asymptomatic and
found incidentally, and their occurrence has been recen-
tly increasing with the advancement of imaging techni-
ques. Angiography is the gold standard in the diagnosis
of renovascular injuries, and it has the additional advan-
tage to possesses the poten tial of therapeutic intervention
[2]. Therefore, after any invasive urological procedure,
CT angiography can be considered as the first choice for
renal artery injury [3,4]. In the present case, we inciden-
tally discovered a lesion of the left renal artery and we
completed the diagnostic work-up with a 3D-CT scan.
2. Case Report
A 67-year-old woman was referred to the Department of
Urology for left flank pain developed seven days after
hysterectomy for uterine leiomyomatosis. The patient
had no history of previous flank trauma, renal stone or
upper urinary tract infections. Physical examination was
unremarkable, with only minimal flank pain at Giordano
manoeuvre; body temperature was 37˚C, blood pressure
was 120/75 mmHg. White cell count was within the
limits (9 × 109 white blood cells in a litre of blood); ren al
and liver functions were normal (creatinine 0.9 mg/dL,
total bilirubin 0.8 mg/dL). A severe left hydronephrosis
was detected at ultrasound, with no sign of uretheral
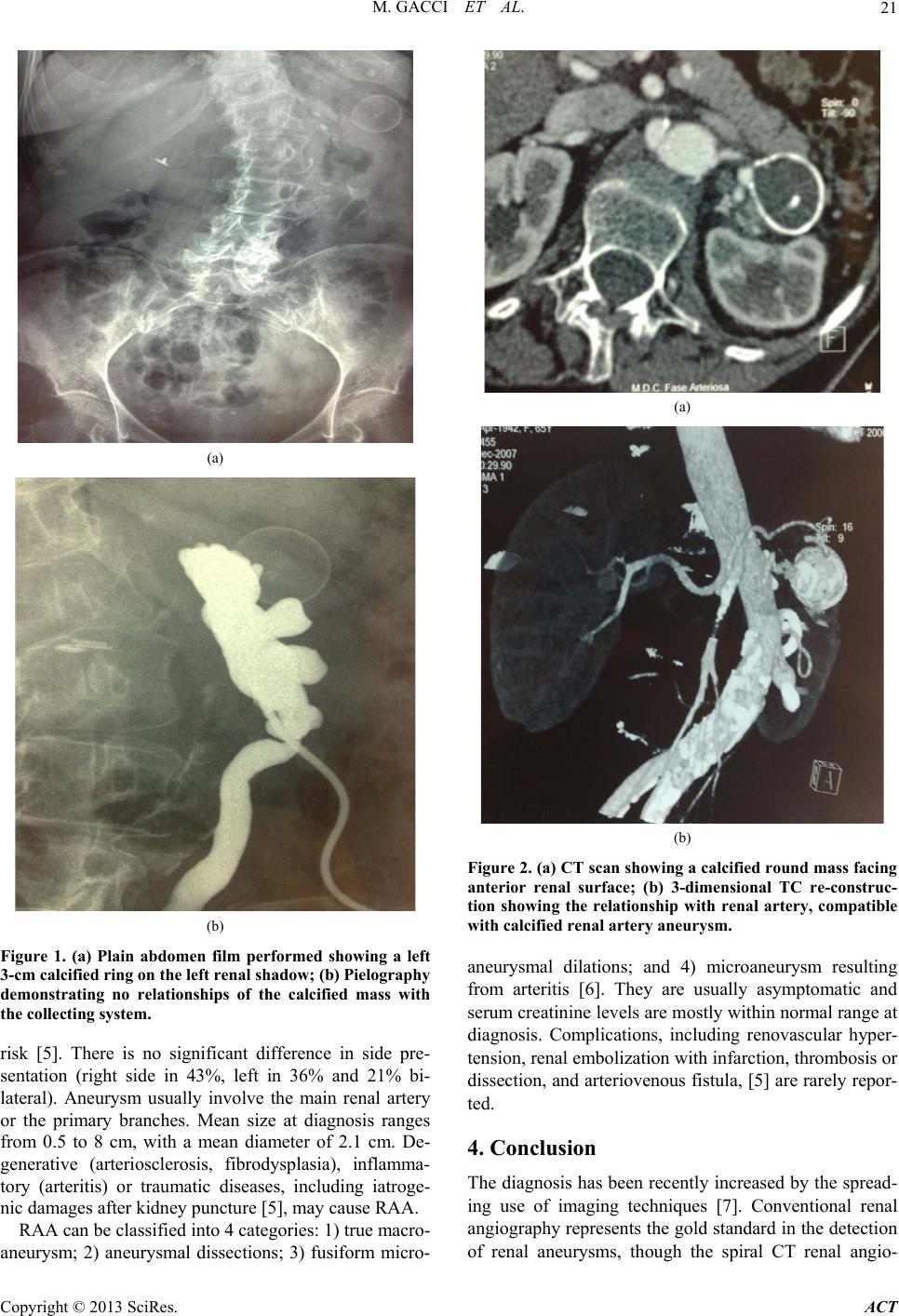
stones or masses. The plain abdomen film showed a 3-cm
calcified ring on the left renal shadow (Figure 1(a)).
Percutaneous pielography confirmed hydronephrosis, and
showed no relationship of the calcified mass with th e col-
lecting system (Figure 1(b)).
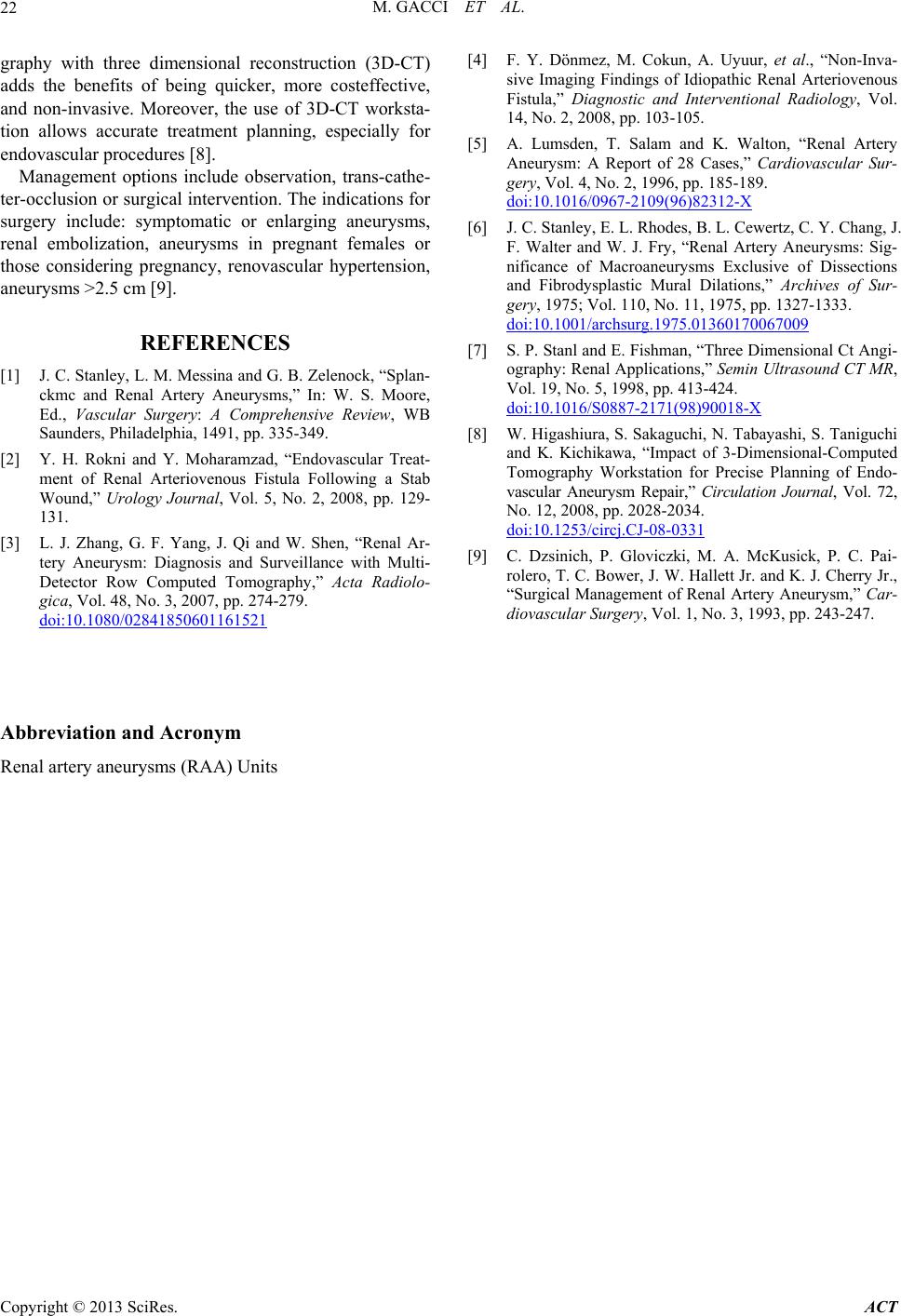
A 3-dimensional-CT scan revealed a 3-cm round hol-
low mass with calcified walls located in front of anterior
renal surface. The lesion had no connection with renal
pelvis (Figure 2(a)) but was firmly related with renal
artery, and it was compatible with calcified renal artery
aneurysm (Figure 2(b)). The patient was treated with an
open access ureteral reimplantation performed on the
suture of the previous surgical approach. A direct ure-
theral reimplantation on the upper bladder wall was per-
formed, with psoas hitch and double J uretheral stenting.
At the 1 month follow up visit there was a complete
recovery of the obstruction. The vascular surgeon sugge-
sted a watchful waiting by monitoring blood pressure,
renal function, and imaging ever y 6 months.
3. Discussion
Renal artery aneurysms (RAA) are rare, with an estima-
ted incidence below 1%. Hypertension and fibro-mus-
cular disease of the renal artery are the leading classes of
C
opyright © 2013 SciRes. ACT