Y. Uchiyama-Tanaka / Health 5 (2013) 253-258 257
temperature in the study was 0.597˚C, less than 1.0˚C
suggested by Tei’s et al. Furthermore, the renal impair-
ment of hemodialysis patients in the present study may
lead to accumulation of levels of N-terminal proBNP [7,
15,24,25]. Moreover, this study included a small popula-
tion that was followed up for a very limited duration.
5. CONCLUSION
Using such a convenient and simple method for ther-
mal therapy, the author demonstrated an improvement in
patients who suffered from pain and experienced diffi-
culty with mobility. The therapy also could be conducted
without the side effects associated with other effective
therapies. The author concludes that thermal therapy
using hot water bottles is very safe and tends to decrease
plasma BNP levels in hemodialysis patients with CHF.
6. KEY SUMMARY POINTS
The author assessed the efficacy of substituting infra-
red dry sauna with hot water bottle thermal therapy.
A total of nine patients whose brain natriuretic pep-
tide (BNP) levels were more than 500 pg/mL agreed
to be enrolled in this study and received thermal
therapy using hot water bottles.
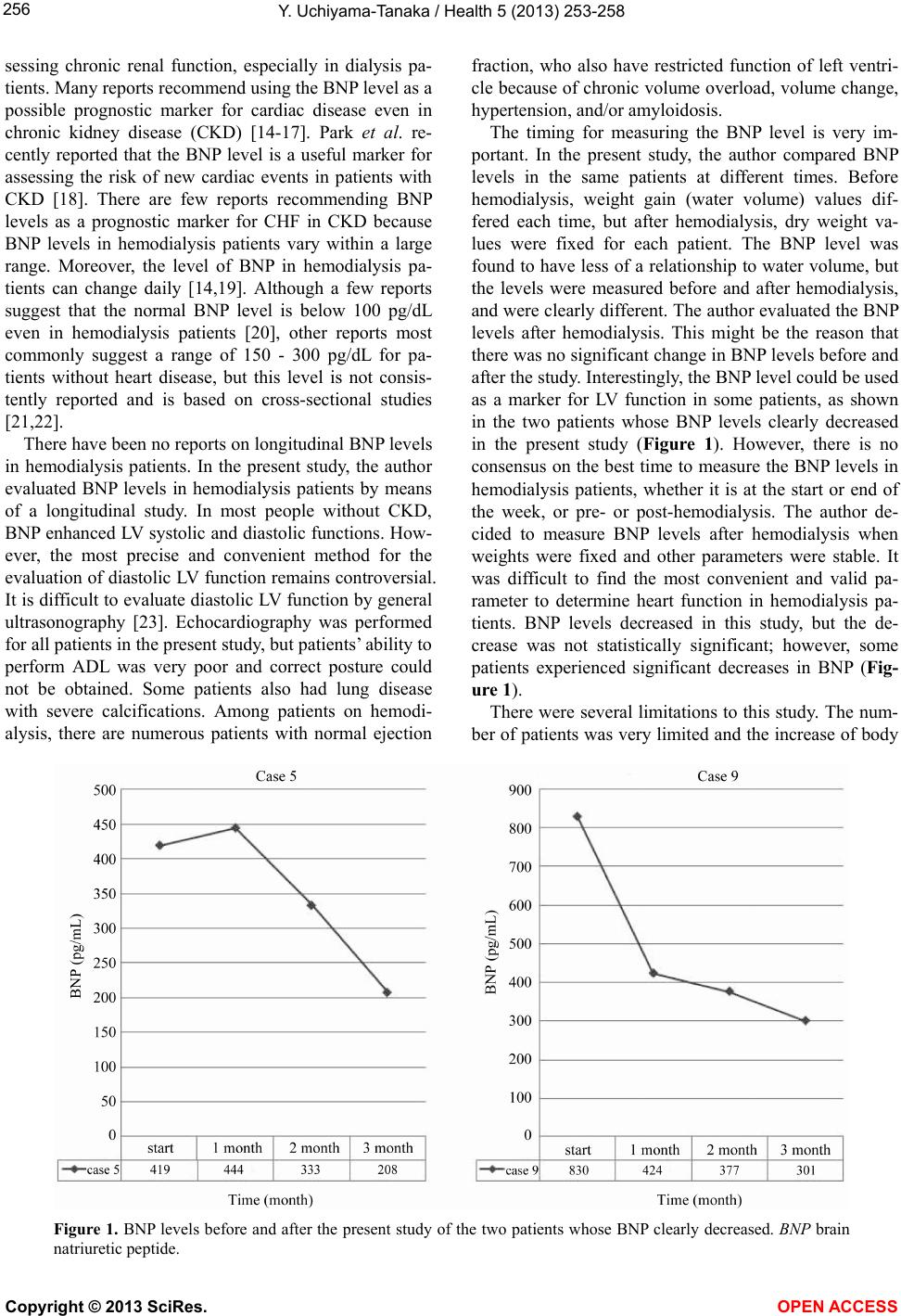
Plasma BNP levels tends to decrease (891 ± 448
pg/mL to 680 ± 339 pg/mL), but there was no signi-
ficant difference (P = 0.0845). The oral temperature
changed 36.44˚C ± 0.45˚C to 37.04˚C ± 0.48˚C
(+0.597˚C, P < 0.0001).
Most patients showed an improvement in their symp-
toms and ability to perform activities of daily living.
The author concludes that thermal therapy using hot
water bottle is a very safe and tends to reduce plasma
BNP levels in hemodialysis patients with chronic
heart failure.
7. ACKNOWLEDGMENTS
Dr. Uchiyama-Tanaka is the guarantor for this article, and takes re-
sponsibility for the integrity of the work as a whole.
Open Access. This article is distributed under the terms of the Crea-
tive Commons Attribution Noncommercial License which permits any
noncommercial use, distribution, and reproduction in any medium,
provided the original author(s) and source are credited.
REFERENCES
[1] Parfery, P.S. and Foley, R.N. (1999) The clinical epide-
miology of cardiac disease in chronic heart failure. Jour-
nal of the American Society of Nephrology, 10, 1606-
1615.
[2] Hamett, J.D., Foley, R.N., Kent, G.M., et al. (1995) Con-
gestive heart failure in dialysis patients: Prevalence, inci-
dence, prognosis and risk factors. Kidney International,
47, 884-890. doi:10.1038/ki.1995.132
[3] Ronco, C., Happio, M., House, A.A., et al. (2008) Cardio-
renal syndrome. Journal of the American College of Car-
diology, 52, 1527-1539. doi:10.1016/j.jacc.2008.07.051
[4] Kihara, T., Miyata, M., Fukudome, T., et al. (2009) Waon
therapy improves the prognosis of patients with chronic
heart failure. Journal of Cardiology, 53, 214-218.
doi:10.1016/j.jjcc.2008.11.005
[5] Miyata, M., Kihara, T., Kubozono, T., et al. (2008) Bene-
ficial effects of Waon therapy on patients with chronic
heart failure: Results of a prospective multicenter study.
Journal of Cardiology, 52, 79-85.
doi:10.1016/j.jjcc.2008.07.009
[6] Kihara, T., Biro, S., Ikeda, Y., et al. (2004) Effects of
repeated sauna treatment on ventricular arrhythmia inpa-
tients with chronic heart failure. Circulation Journal, 68,
1146-1151. doi:10.1253/circj.68.1146
[7] Wilkins, M.R., Redondo, J. and Brown, L.A. (1997) The
natriuretic-peptide family. Lancet, 349, 1307-1310.
doi:10.1016/S0140-6736(96)07424-7
[8] Hunt, S.A., Baker, D.W., Chin, M.H., American College
of Cardiology/American Heart Association, et al. (2001)
ACC/AHA guidelines for the evaluation and management
of chronic heart failure in the adult: Executive summary.
A Report of the American College of Cardiology/Ameri-
can Heart Association Task Force on Practice Guidelines
(Committee to revise the 1995 Guidelines for the Evalua-
tion and Management of Heart Failure). Journal of Ameri -
can College of Cardiology, 38, 2101-2113.
doi:10.1016/S0735-1097(01)01683-7
[9] Tei, C., Prihara, K. and Fukudome, T. (2007) Remarkable
efficacy of thermal therapy for Sjogren syndrome. Journal
of Cardiology, 49, 217-219.
[10] Biro, S., Masuda, A., Kihara, T., et al. (2003) Clinical
implications of thermal therapy in lifestyle-related dis-
eases. Experimental Biology and Medicine, 228, 1245-
1249.
[11] Madarame, H. and Kawashima, A. (2006) Use of hot water
bottles can improve lymphocytopenia. Biomedical Re-
search, 27, 45-48. doi:10.2220/biomedres.27.45
[12] Toyabe, S., Iiai, T., Fukuda, M., et al. (1997) Identifica-
tion of nicotinic acetylcholine receptors on lymphocytes
in the periphery as well as thymus in mice. Immunology,
92, 201-205. doi:10.1046/j.1365-2567.1997.00323.x
[13] Watanabe, M., Tomiyama-Miyaji, C., Kainuma, E., et al.
(2008) Role of alpha-adrenergic stimulus in stress-in-
duced modulation of body temperature, blood glucose
and innate immunity. Immunology Letters, 115, 43-49.
doi:10.1016/j.imlet.2007.09.010
[14] Nishikimi, T., Futoo, Y., Tamano, K., et al. (2001) Plasma
brain natriuretic peptide levels in chronic hemodialysis
patients: Influence of coronary artery disease. American
Journal of Kidney Disease, 37, 1201-1208.
doi:10.1053/ajkd.2001.24523
[15] Austin, W.J., Bhalla, V., Hernandez-Arce, I., et al. (2006)
Correlation and prognostic utility of B-type natriuretic
peptide and its amino-terminal fragment in patients with
chronic kidney disease. American Journal of Clinical Pa-
Copyright © 2013 SciRes. OPEN A CCESS