 Vol.3, No.1, 128-131 (2013) Open Journal of Preventive Medicine http://dx.doi.org/10.4236/ojpm.2013.31016 Bone mineral density in Iranian patients: Effects of age, sex, and body mass index Mehrdad Aghaei1, Hamid Reza Bazr Afshan1*, Mostafa Qorbani2, Hossien Shadpour Dashti3, Roya Safari4 1Bone joints & Connective Tissue Disease Research Center, Golestan University of Medical Sciences, Gorgan, Iran; *Corresponding Author: Mahdieh.shojaa_mw@yahoo.com 2Department of Epidemiology & Biostatistics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran 3Department of Internal Medicine, Golestan University of Medical Sciences, Gorgan, Iran 4Department of Internal Medicine, Tehran University of Medical Sciences, Tehran, Iran Received 22 June 2012; revised 28 July 2012; accepted 5 August 2012 ABSTRACT Introduction: Osteoporosis is a multifactorial skeletal disease that is characterized by reduced bone mineral density (BMD). BMD values de- pend on several factors such as age, sex and age at menopause. The purpose of this study was to determine the prevalence and changes in bone mineral density in Iranian patients. Meth- ods: Three hundred patients were selected through random sampling technique in 2009. BMD was assessed by Norland (Excell) technique at the lumbar and femoral neck. Weight and height were measured through standard methods. A thorough history was taken from each patient. The data was analyzed using SPSS software version 13.0. P-values less than 0.05 were con- sidered statistically significant. Results: From among the 300 studied patients, 86.6% were fe- male. their mean age was 52.7 years. Their av- erage body mass index (BMI) was 28.14 kg/m2. Mean T-Score at lumbar spine and femoral neck was −1.07 ± 1.19 and −1.75 ± 1.33 respectively. Mean BMD value at lumbar spine and femoral neck was 0.92 ± 0.19 and 0.77 ± 0.16 respectively. The prevalence of osteoporosis at lumbar spine and femoral neck was 33.7% and 16.7, respec- tively. There was a significant correlation be- tween age, BMI and BMD values (P-Value < 0.01). Correlation between gender and BMD value at the lumbar spine and femoral neck was not sig- nificant. Conclusion: This study shows that age- ing and low BMI are risk factors associated with bone loss. it is recommended to measure BMD and implement prevention programs for high- risk people. Keywords: Bone Mineral Density; Body Mass Index; Age; Gender 1. INTRODUCTION Osteoporosis is a multifactorial skeletal disease char- acterized by reduced bone mineral density (BMD) along with the deterioration of the microarchitectural structure of bone tissue, and a consequent increase in bone fragil- ity and fracture risk [1,2]. Osteoporosis is a common disease among the elderly, particularly the post-meno- pausal women [3-7]. BMD values depend on such factors as age, sex and age at menopause [8-10]. It has been pre- dicted that in 2050, 50% of all hip fractures in the world will be occurring in Asia [11]. Osteoporosis is a disease that affects many millions of people around the world. It affects more than 75 million people in the United States, Europe and Japan [12]. It is estimated that world’s an- nual incidence of hip fracture will increase from 1.26 million cases in 1990 to 2.6 million by 2025 and to 4.5 million by 2050 [13]. Osteoporotic fractures affect the quality of life and are associated with premature mortal- ity [14]. The prevalence of osteoporosis among Iranian women varies from 6 to 34.4 percent in different cities and provinces [15-18]. In the present study, we evaluated the prevalence and correlation of osteoporosis with demo- graphic factors among patients referred to a densitometry center in Gorgan, a city located in North Iran. 2. MATERIAL & METHODS From among 3000 patients who were referred to the Azar 5th teaching hospital affiliated to Gorgan Univer- sity of Medical Sciences, 300 patients were selected through random sampling technique in 2009. The indi- viduals with underlying diseases affecting bone mass such as rheumatoid arthritis, renal and liver failure and any cansers were excluded. BMD was assessed by Nor- land (Excell) technique at the lumbar and femoral neck. Based on WHO classification, individuals with T-score Copyright © 2013 SciRes. OPEN ACCESS 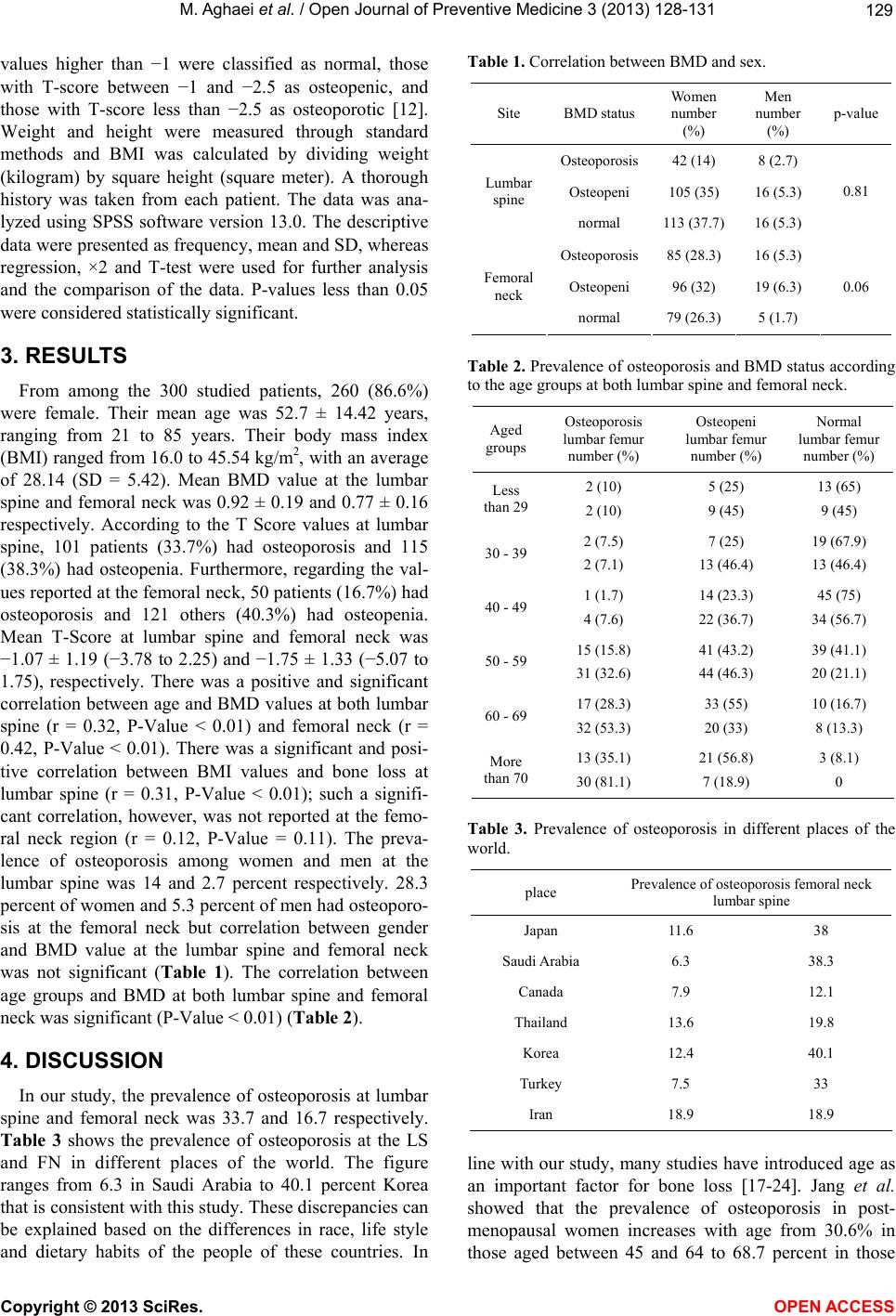 M. Aghaei et al. / Open Journal of Preventive Medicine 3 (2013) 128-13 1 129 values higher than −1 were classified as normal, those with T-score between −1 and −2.5 as osteopenic, and those with T-score less than −2.5 as osteoporotic [12]. Weight and height were measured through standard methods and BMI was calculated by dividing weight (kilogram) by square height (square meter). A thorough history was taken from each patient. The data was ana- lyzed using SPSS software version 13.0. The descriptive data were presented as frequency, mean and SD, whereas regression, ×2 and T-test were used for further analysis and the comparison of the data. P-values less than 0.05 were considered statistically significant. 3. RESULTS From among the 300 studied patients, 260 (86.6%) were female. Their mean age was 52.7 ± 14.42 years, ranging from 21 to 85 years. Their body mass index (BMI) ranged from 16.0 to 45.54 kg/m2, with an average of 28.14 (SD = 5.42). Mean BMD value at the lumbar spine and femoral neck was 0.92 ± 0.19 and 0.77 ± 0.16 respectively. According to the T Score values at lumbar spine, 101 patients (33.7%) had osteoporosis and 115 (38.3%) had osteopenia. Furthermore, regarding the val- ues reported at the femoral neck, 50 patients (16.7%) had osteoporosis and 121 others (40.3%) had osteopenia. Mean T-Score at lumbar spine and femoral neck was −1.07 ± 1.19 (−3.78 to 2.25) and −1.75 ± 1.33 (−5.07 to 1.75), respectively. There was a positive and significant correlation between age and BMD values at both lumbar spine (r = 0.32, P-Value < 0.01) and femoral neck (r = 0.42, P-Value < 0.01). There was a significant and posi- tive correlation between BMI values and bone loss at lumbar spine (r = 0.31, P-Value < 0.01); such a signifi- cant correlation, however, was not reported at the femo- ral neck region (r = 0.12, P-Value = 0.11). The preva- lence of osteoporosis among women and men at the lumbar spine was 14 and 2.7 percent respectively. 28.3 percent of women and 5.3 percent of men had osteoporo- sis at the femoral neck but correlation between gender and BMD value at the lumbar spine and femoral neck was not significant (Table 1). The correlation between age groups and BMD at both lumbar spine and femoral neck was significant (P-Value < 0.01) (Table 2). 4. DISCUSSION In our study, the prevalence of osteoporosis at lumbar spine and femoral neck was 33.7 and 16.7 respectively. Table 3 shows the prevalence of osteoporosis at the LS and FN in different places of the world. The figure ranges from 6.3 in Saudi Arabia to 40.1 percent Korea that is consistent with this study. These discrepancies can be explained based on the differences in race, life style and dietary habits of the people of these countries. In Table 1. Correlation between BMD and sex. Site BMD status Women number (%) Men number (%) p-value Osteoporosis42 (14) 8 (2.7) Osteopeni 105 (35) 16 (5.3) Lumbar spine normal 113 (37.7) 16 (5.3) 0.81 Osteoporosis85 (28.3) 16 (5.3) Osteopeni 96 (32) 19 (6.3) Femoral neck normal 79 (26.3) 5 (1.7) 0.06 Table 2. Prevalence of osteoporosis and BMD status according to the age groups at both lumbar spine and femoral neck. Aged groups Osteoporosis lumbar femur number (%) Osteopeni lumbar femur number (%) Normal lumbar femur number (%) Less than 29 2 (10) 2 (10) 5 (25) 9 (45) 13 (65) 9 (45) 30 - 392 (7.5) 2 (7.1) 7 (25) 13 (46.4) 19 (67.9) 13 (46.4) 40 - 491 (1.7) 4 (7.6) 14 (23.3) 22 (36.7) 45 (75) 34 (56.7) 50 - 5915 (15.8) 31 (32.6) 41 (43.2) 44 (46.3) 39 (41.1) 20 (21.1) 60 - 6917 (28.3) 32 (53.3) 33 (55) 20 (33) 10 (16.7) 8 (13.3) More than 70 13 (35.1) 30 (81.1) 21 (56.8) 7 (18.9) 3 (8.1) 0 Table 3. Prevalence of osteoporosis in different places of the world. place Prevalence of osteoporosis femoral neck lumbar spine Japan 11.6 38 Saudi Arabia 6.3 38.3 Canada 7.9 12.1 Thailand 13.6 19.8 Korea 12.4 40.1 Turkey 7.5 33 Iran 18.9 18.9 line with our study, many studies have introduced age as an important factor for bone loss [17-24]. Jang et al. showed that the prevalence of osteoporosis in post- menopausal women increases with age from 30.6% in those aged between 45 and 64 to 68.7 percent in those Copyright © 2013 SciRes. OPEN ACCESS 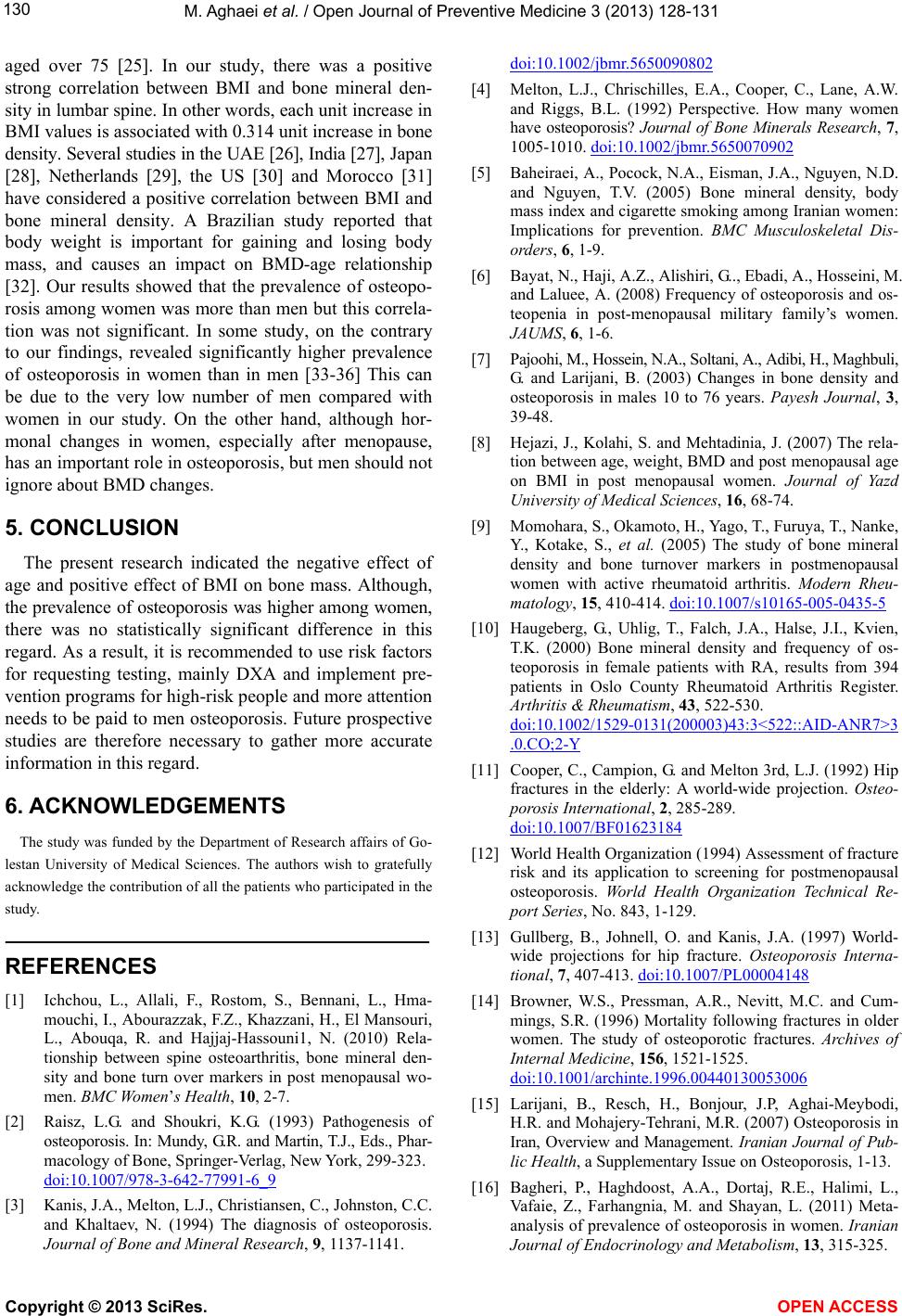 M. Aghaei et al. / Open Journal of Preventive Medicine 3 (2013) 128-13 1 130 aged over 75 [25]. In our study, there was a positive strong correlation between BMI and bone mineral den- sity in lumbar spine. In other words, each unit increase in BMI values is associated with 0.314 unit increase in bone density. Several studies in the UAE [26], India [27], Japan [28], Netherlands [29], the US [30] and Morocco [31] have considered a positive correlation between BMI and bone mineral density. A Brazilian study reported that body weight is important for gaining and losing body mass, and causes an impact on BMD-age relationship [32]. Our results showed that the prevalence of osteopo- rosis among women was more than men but this correla- tion was not significant. In some study, on the contrary to our findings, revealed significantly higher prevalence of osteoporosis in women than in men [33-36] This can be due to the very low number of men compared with women in our study. On the other hand, although hor- monal changes in women, especially after menopause, has an important role in osteoporosis, but men should not ignore about BMD changes. 5. CONCLUSION The present research indicated the negative effect of age and positive effect of BMI on bone mass. Although, the prevalence of osteoporosis was higher among women, there was no statistically significant difference in this regard. As a result, it is recommended to use risk factors for requesting testing, mainly DXA and implement pre- vention programs for high-risk people and more attention needs to be paid to men osteoporosis. Future prospective studies are therefore necessary to gather more accurate information in this regard. 6. ACKNOWLEDGEMENTS The study was funded by the Department of Research affairs of Go- lestan University of Medical Sciences. The authors wish to gratefully acknowledge the contribution of all the patients who participated in the study. REFERENCES [1] Ichchou, L., Allali, F., Rostom, S., Bennani, L., Hma- mouchi, I., Abourazzak, F.Z., Khazzani, H., El Mansouri, L., Abouqa, R. and Hajjaj-Hassouni1, N. (2010) Rela- tionship between spine osteoarthritis, bone mineral den- sity and bone turn over markers in post menopausal wo- men. BMC Wo m en’s Health, 10, 2-7. [2] Raisz, L.G. and Shoukri, K.G. (1993) Pathogenesis of osteoporosis. In: Mundy, G.R. and Martin, T.J., Eds., Phar- macology of Bone, Springer-Verlag, New York, 299-323. doi:10.1007/978-3-642-77991-6_9 [3] Kanis, J.A., Melton, L.J., Christiansen, C., Johnston, C.C. and Khaltaev, N. (1994) The diagnosis of osteoporosis. Journal of Bone and Mineral Research, 9, 1137-1141. doi:10.1002/jbmr.5650090802 [4] Melton, L.J., Chrischilles, E.A., Cooper, C., Lane, A.W. and Riggs, B.L. (1992) Perspective. How many women have osteoporosis? Journal of Bone Minerals Research, 7, 1005-1010. doi:10.1002/jbmr.5650070902 [5] Baheiraei, A., Pocock, N.A., Eisman, J.A., Nguyen, N.D. and Nguyen, T.V. (2005) Bone mineral density, body mass index and cigarette smoking among Iranian women: Implications for prevention. BMC Musculoskeletal Dis- orders, 6, 1-9. [6] Bayat, N., Haji, A.Z., Alishiri, G.., Ebadi, A., Hosseini, M. and Laluee, A. (2008) Frequency of osteoporosis and os- teopenia in post-menopausal military family’s women. JAUMS, 6, 1-6. [7] Pajoohi, M., Hossein, N.A., Soltani, A., Adibi, H., Maghbuli, G. and Larijani, B. (2003) Changes in bone density and osteoporosis in males 10 to 76 years. Payesh Journal, 3, 39-48. [8] Hejazi, J., Kolahi, S. and Mehtadinia, J. (2007) The rela- tion between age, weight, BMD and post menopausal age on BMI in post menopausal women. Journal of Yazd University of Medical Sciences, 16, 68-74. [9] Momohara, S., Okamoto, H., Yago, T., Furuya, T., Nanke, Y., Kotake, S., et al. (2005) The study of bone mineral density and bone turnover markers in postmenopausal women with active rheumatoid arthritis. Modern Rheu- matology, 15, 410-414. doi:10.1007/s10165-005-0435-5 [10] Haugeberg, G., Uhlig, T., Falch, J.A., Halse, J.I., Kvien, T.K. (2000) Bone mineral density and frequency of os- teoporosis in female patients with RA, results from 394 patients in Oslo County Rheumatoid Arthritis Register. Arthritis & Rheumatism, 43, 522-530. doi:10.1002/1529-0131(200003)43:3<522::AID-ANR7>3 .0.CO;2-Y [11] Cooper, C., Campion, G. and Melton 3rd, L.J. (1992) Hip fractures in the elderly: A world-wide projection. Osteo- porosis International, 2, 285-289. doi:10.1007/BF01623184 [12] World Health Organization (1994) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. World Health Organization Technical Re- port Series, No. 843, 1-129. [13] Gullberg, B., Johnell, O. and Kanis, J.A. (1997) World- wide projections for hip fracture. Osteoporosis Interna- tional, 7, 407-413. doi:10.1007/PL00004148 [14] Browner, W.S., Pressman, A.R., Nevitt, M.C. and Cum- mings, S.R. (1996) Mortality following fractures in older women. The study of osteoporotic fractures. Archives of Internal Medicine, 156, 1521-1525. doi:10.1001/archinte.1996.00440130053006 [15] Larijani, B., Resch, H., Bonjour, J.P, Aghai-Meybodi, H.R. and Mohajery-Tehrani, M.R. (2007) Osteoporosis in Iran, Overview and Management. Iranian Journal of Pub- lic Health, a Supplementary Issue on Osteoporosis, 1-13. [16] Bagheri, P., Haghdoost, A.A., Dortaj, R.E., Halimi, L., Vafaie, Z., Farhangnia, M. and Shayan, L. (2011) Meta- analysis of prevalence of osteoporosis in women. Iranian Journal of Endocrinology and Metabolism, 13, 315-325. Copyright © 2013 SciRes. OPEN ACCESS  M. Aghaei et al. / Open Journal of Preventive Medicine 3 (2013) 128-13 1 Copyright © 2013 SciRes. OPEN ACCESS 131 [17] Derakhshan, S., Salehi, R. and Reshadmanesh, N. (2006) Prevalence of osteoporosis, osteopenia and their related factors in post-menopausal women referring to Kurdistan densitometry center. Scientific Journal of Kurdistan Uni- versity of Medical Sciences, 11, 59-67. [18] Mojibian, M., Owlia, M.B., Beiki, B.O. and Kochak, Y.L. (2006) Osteoporosis in postmenopausal women. Iranian Journal of Surgery, 14, 62-70. [19] Namwongprom, S., Ekmahachai, M., Vilasdechanon, N., Klaipetch, A., Wongboontan, C. and Boonyaprapa, S. (2011) Bone mineral density: Correlation between the lumbar spine, proximal femur and radius in northern Thai women. Journal of the Medical Association of Thailand, 94, 725-731. [20] Pinheiro, M.M., Reis Neto, E.T., Machado, F.S., Omura, F., Yang, J.H.K., Szejnfeld, I.J. and Szejnfeld, V.L. (2010) Risk factors for osteoporotic fractures and low bone den- sity in pre and postmenopausal women. Revista de Saúde Pública, 44, 479-485. doi:10.1590/S0034-89102010000300011 [21] Meiyanti (2010) Epidemiology of osteoporosis in post- menopausal women aged 47 to 60 years. Universa Medi- cina, 29, 169-176. [22] Heidari, Z., Zyaie, S. and Moghassemi, S. (2010) The relationship between BMI and reproductive histories and bone density in postmenopausal women. Arak Medical University Journal, (AMUJ), 13, 53-60. [23] Jamshidian-Tehrani, M., Kalantari, N., Azadbakht, L., Esmaillzadeh, A., Rajaie, A., Houshiar-rad, A., Golestan, B. and Kamali, Z. (2004) Osteoporosis risk factors in Te- hrani women aged 40-60 years. Endocrinology and Me- tabolism, 6, 139-145. [24] Zhang, H.C., Kushida, K., Atsumi, K., Kin, K. and Na- gano, A. (2002) Effects of age and menopause on spinal bone mineral density in Japanese women: A ten-year pro- spective study. Calcified Tissue International, 70, 153- 157. doi:10.1007/s00223-001-1037-7 [25] Jang, S.N., Choi, Y.H., Choi, M.G., Kang, S.H., Jeong, J.Y., Choi, Y.J. and Kim, D.H. (2006) Prevalence and as- sociated factors of osteoporosis among postmenopausal women in Chuncheon: Hallym aging study (HAS). Jour- nal of Preventive Medicine and Public Health, 39, 389- 396. [26] Fawzy, T, Muttappallymyalil, J., Sreedharan, J., Ahmed, A., Saeed, A.S.O., Al Ali, M.S. and Al Balsooshi, K.A. (2011) Association between body mass index and bone mineral density in patients referred for dual-energy x-ray absorptiometry scan in Ajman, UAE. Journal of Osteopo- ro si s, 4 Pages. [27] Elizabeth, J., Dayananda, G., Satyavati, K. and Kumar, P. (2009) Bone mineral density in healthy south Indian men. Journal of Physiological and Biomedical Sciences, 2, 41-44. [28] Arimatsu, M., Kitano, T., Kitano, N., Inomoto, T., Shono, M., Futatsuka, M. (2005) Correlation between forearm bone mineral density and body composition in Japanese females aged 18-40 years. Environmental Health and Preventive Medicine, 10, 144-149. doi:10.1007/BF02900807 [29] van der Voort, D.J., Geusens, P.P. and Dinant, G.J. (2001) Risk factors for osteoporosis related to their outcome: Fractures. Osteoporosis International, 12, 630-638. doi:10.1007/s001980170062 [30] Castro, J.P., Joseph, L.A., Shin, J.J., Arora, S.K., Nicasio, J., Shatzkes, J., et al. (2005) Differential effect of obesity on bone mineral density in White, Hispanic and African American women: A cross sectional study. Nutrition & Metabolism, 2, 9. doi:10.1186/1743-7075-2-9 [31] Maghraoui, A.E., Guerboub, A.A., Mounach, A., Ghozlani, I., Nouijai, A., Ghazi, M., et al. (2007) Body mass index and gynecological factors as determinants of bone mass in healthy Moroccan women. Maturitas, 56, 375-382. doi:10.1016/j.maturitas.2006.10.004 [32] Lewin, S., Gouveia, C.H., Marone, M.M., Wehba, S., Malvestiti, L.F. and Bianco, A.C. (1997) Densidade min- eral óssea vertebral e femoral em 724 mulheres brancas brasileiras: Influência da idade e do peso corporal. Re- vista da Associação Médica Brasileira, 43, 127-136. doi:10.1590/S0104-42301997000200009 [33] Cui, L.H., Choi, J.S., Shin, M.H., Kweon, S.S., Park, K.S., Lee, Y.H., et al. (2008) Prevalence of osteoporosis and reference data for lumbar spine and hip bone mineral density in a Korean population. Journal of Bone and Mineral Metabolism, 26, 609-617. doi:10.1007/s00774-007-0847-8 [34] Tuck S.P., Pearce, M.S., Rawlings, D.J., Birrell, F.N., Parker, L. and Francis, R.M. (2005) Differences in bone mineral density and geometry in men and women: The Newcastle thousand families study at 50 years old. British Journal of Radiology, 78, 493-498. doi:10.1259/bjr/42380498 [35] Anburajan, M., Ashok, K.D. and Sapthagirivasan, V. (2011) Evaluation of osteoporosis in Indian women and men us- ing peripheral dual energy x-ray absorptiometry (pDXA). IPCBEE, 5, 470-474. [36] Lei, S.F., Deng, F.Y., Li, M.-X., Dvornyk, V. and Deng, H.W. (2004) Bone mineral density in elderly Chinese: Effects of age, sex, weight, height, and body mass index. Journal of Bone and Mineral Metabolism, 22, 71-78. doi:10.1007/s00774-003-0452-4
|