J. H. Andersen et al. / Open Journal of Preve ntive Medicine 3 (2013) 104-110 109
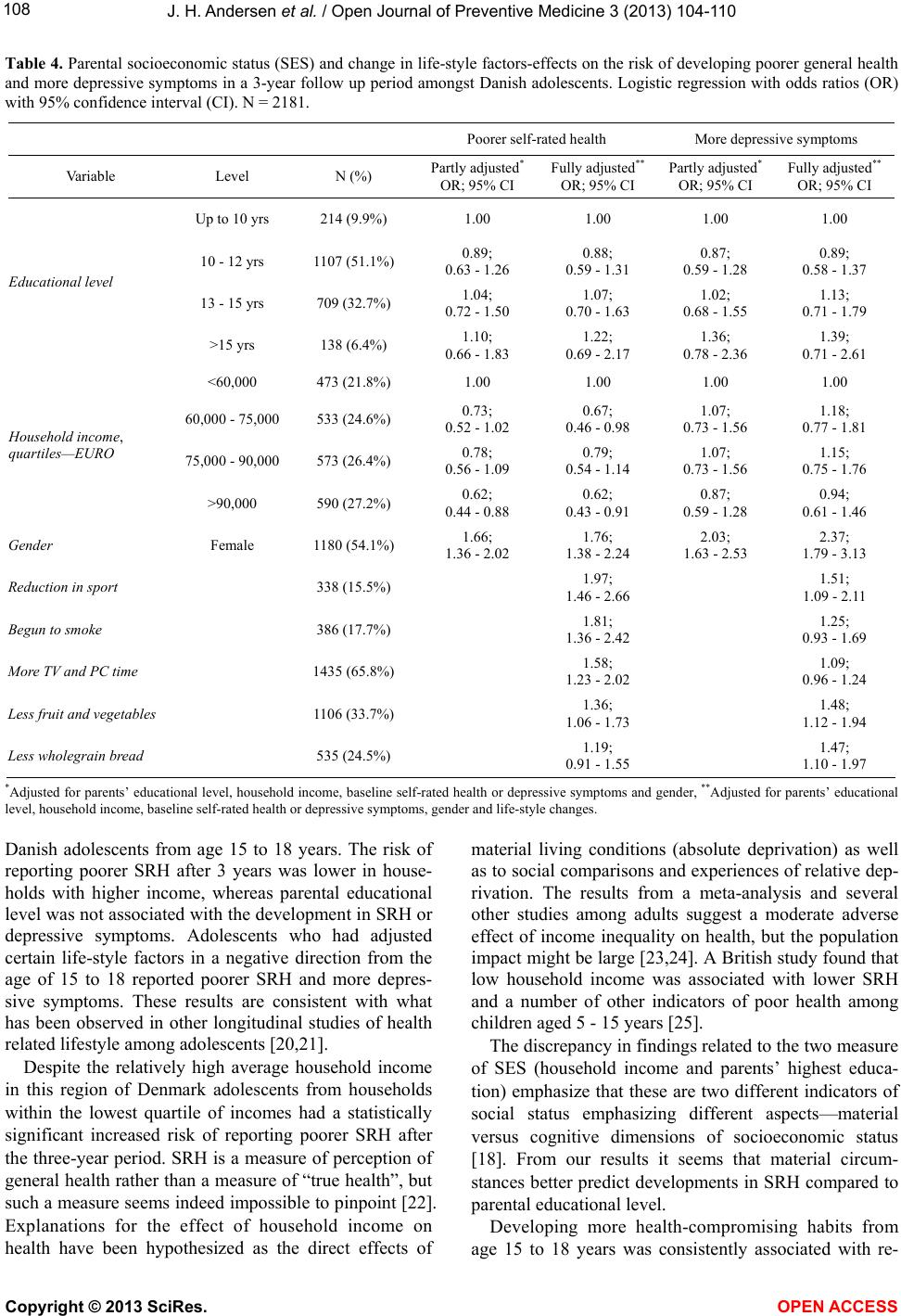
porting both poorer SRH and, to a lesser extent, more
depressive symptoms in this group of adolescents. Even
though the study was prospective there could be reverse
causation in that, for example, a reduction in sporting
activities could be due to developing poorer SRH and
more depressive symptoms in the 3-year period. We
tested for an association between changes in health-
compromising habits as the outcome variables using
SRH and depressive symptoms as explanatory variables,
and found several significant associations indicating that
causation was bidirectional. The protective effect of
positive health behaviour is in line with similar findings
suggested in previous cross sectional studies [16,26,27].
Health-compromising behaviors and a lack of sporting
activity and exercise were also found to be risk factors
for deterioration in SRH in the Young-Hunt-Study,
which benefits from a 4-year observation period [4]. We
conclude that health risk behaviours, such as lack of lei-
sure time sporting activity and smoking may contribute
to later poor self-rated health. This has also been found
to be true over a follow-up period of 25 years [28]. But
in addition, developing more depressive symptoms and
experiencing a deterioration in SRH may also result in
health-compromising behaviours. This study benefits
from using register-based information on parents educa-
tion and household income. Comparing non-responders
at baseline and dropouts in the follow-up period it can be
seen that there were more non-responders and dropouts
from households with low income and the least parental
educational. This selection would tend to bias the results
towards the null.
From a public health perspective, this study supports
the idea that increasing sporting activities and providing
better opportunities for healthy nutrition in schools will
improve chances for the successful prevention of the
development of poorer health among adolescents. A re-
cent Cochrane review [29] found that there is some evi-
dence of positive effects on lifestyle behaviors and
physical health status measures, and that ongoing physi-
cal activity promotion in schools is recommended.
The study also points to the importance of giving spe-
cial attention to adolescents who develop more depres-
sive symptoms or experience a deterioration in SRH: this
group may be at greater risk of developing a health com-
promising lifestyle to put their health at further risk.
This research received no specific grant from any
funding agency in the public, commercial, or not-for-
profit sectors.
REFERENCES
[1] Manderbacka, K. Lahelma, F. and Martikainen, P. (1998)
Examining the continuity of self-rated health. Interna-
tional Journal of Epidemiology, 27, 208-213.
doi:10.1093/ije/27.2.208
[2] Nielsen, A.B.S., Siersma, V. and Hiort, L.C., Drivsholm,
T. Kreiner, S. and Hollnagel, H. (2008) Self-rated general
health among 40-year-old Danes and its association with
all-cause mortality at 10-, 20-, and 29 years’ follow-up.
Scand Journal of Public Health, 36, 3-11.
doi:10.1177/1403494807085242
[3] Boardman, J.D. (2006) Self-rated health among US ado-
lescents. Journal of Adolescent Health, 38, 401-408.
doi:10.1016/j.jadohealth.2005.01.006
[4] Breidablik, H.J. Meland, E. and Lydersen, S. (2009)
Self-rated health during adolescence: Stability and pre-
dictors of change (Young-Hunt study, Norway). European
Journal of Public Health, 19, 73-78.
doi:10.1093/eurpub/ckn111
[5] Ravens-Sieberer, U., Erhart, M., Wille, N. and Bullinger,
M. (2008) Health-related quality of life in children and
adolescents in Germany: Results of the BELLA study.
European Child & Adolescent Psychiatry, 17, 148-156.
doi:10.1007/s00787-008-1016-x
[6] Elstad, JI. (2010) Indirect health-related selection or so-
cial causation? Interpreting the educational differences in
adolescent health behaviours. Social Theory & Health, 8,
134-150. doi:10.1057/sth.2009.26
[7] Belfer, M.L. (2008) Child and adolescent mental disor-
ders: The magnitude of the problem across the globe.
Journal of Child Psychology and Psychiatry, 49, 226-236.
doi:10.1111/j.1469-7610.2007.01855.x
[8] World Health Organization (2001) The World health re-
port. Mental health: New understanding, new hope. WHO,
Geneva. http://www.who.int/whr/2001/en/whr01_en.pdf
[9] Costello, E.J. Egger, H. and Angold, A. (2005) 10-year
research update review: The epidemiology of child and
adolescent psychiatric disorders: I. Methods and public
health burden. Journal of the American Academy of Child
& Adolescent Psychiatry, 44, 972-986.
doi:10.1097/01.chi.0000172552.41596.6f
[10] Patel, V., Flisher, A.J., Hetrick, S. and McGorry, P. (2007)
Mental health of young people: A global public-health
challenge. Lancet, 369, 1302-1313.
doi:10.1016/S0140-6736(07)60368-7
[11] Birmaher, B., Ryan, N.D., Williamson, D.E., Brent, D.A.
and Kaufman, J. (1996) Childhood and adolescent de-
pression: A review of the past 10 years. Part II. Journal of
the American Academy of Child and Adolescent Psychia-
try, 35, 1575-1583.
doi:10.1097/00004583-199612000-00008
[12] Clarke, G.N. Hornbrook, M., Lynch, F., Polen, M., Gale,
J., Beardslee, W., O’Connor, E. and Seeley, J. (2001) A
randomized trial of a group cognitive intervention for pre-
venting depression in adolescent offspring of depressed
parents. Archives of General Psychiatry, 58, 1127-1134.
doi:10.1001/archpsyc.58.12.1127
[13] Lewinsohn, P
.M. and Clarke, G.N. (1999) Psychosocial
treatments for adolescent depression. Clinical Psychology
Review, 19, 329-342.
doi:10.1016/S0272-7358(98)00055-5
[14] Dopheide, J.A. (2006) Recognizing and treating depres-
Copyright © 2013 SciRes. OPEN ACCESS