 Vol.3, No.1, 51-57 (2013) Open Journal of Preventive Medicine http://dx.doi.org/10.4236/ojpm.2013.31007 Mixed methods evaluation of a randomized control pilot trial targeting sugar-sweetened beverage behaviors Jamie Zoellner1*, Emily Cook1, Yvonnes Chen2, Wen You3, Brenda Davy1, Paul Estabrooks1 1Department of Human Nutrition Foods and Exercise, Virginia Tech, Blacksburg, USA; *Corresponding Author: zoellner@vt.edu 2Department of Communications, Virginia Tech, Blacksburg, USA 3Department of Agriculture and Applied Economics, Virginia Tech, Blacksburg, USA Received 6 December 2012; revised 8 January 2013; accepted 17 January 2013 ABSTRACT This Excessive sugar-sweetened beverage (SSB) consumption and low health literacy skills have emerged as two public health concerns in the United States (US); however, there is limited re- search on how to effectively address these is- sues among adults. As guided by health liter- acy concepts and the Theory of Planned Be- havior (TPB), this randomized controlled pilot trial applied the RE-AIM framework and a mixed methods approach to examine a sugar-sweet- ened beverage (SSB) intervention (SipSmartER), as compared to a matched-contact control in- tervention targeting physical activity (Move- More). Both 5-week interventions included two interactive group sessions and three support telephone calls. Executing a patient-centered developmental process, the primary aim of this paper was to evaluate patient feedback on in- tervention content and structure. The secondary aim was to understand the potential reach (i.e., proportion enrolled, representativeness) and effectiveness (i.e. health behaviors, theorized mediating variables, quality of life) of SipS- martER. Twenty-five participants were random- ized to SipSmartER (n = 14) or MoveMore (n = 11). Participants’ intervention feedback was positive, ranging from 4.2 - 5.0 on a 5-point scale. Qualita- tive assessments reavealed several opportune- ties to improve clarity of learning materials, en- hance instructions and communication, and re- fine research protocols. Although SSB con- sumption decreased more among the SipS- martER participants (−256.9 ± 622.6 kcals), there were no significant group differences when compared to control participants (−199.7 ± 404.6 kcals). Across both groups, there were signifi- cant improvements for SSB attitudes, SSB be- havioral intentions, and two media literacy con- structs. The value of using a patient-centered approach in the developmental phases of this intervention was apparent, and pilot findings suggest decreased SSB may be achieved through targeted health literacy and TPB strategies. Fu- ture efforts are needed to examine the potential public health impact of a large-scale trial to ad- dress health literacy and reduce SSB. Keywords: Beverages; Health Literacy; Health Education; Public Health; Health Behavior; Pilot Projects 1. INTRODUCTION High sugar-sweetened beverage (SSB) consumption and low health literacy skills have emerged as two broad public health concerns in the United States (US). For example, SSB consumption has approximately doubled in the past two decades and contributes about 10% of the total calories (kcal) in the US diet [1]. While excessive SSB intake has been associated with numerous adverse health outcomes [2], there is limited research on how to effectively improve SSB behaviors among adults. Fur- thermore, it is estimated that one-third of Americans have low health literacy skills [3]. Low health literacy has been associated with poorer health outcomes [4], and one study found health literacy was a stronger predictor of SSB consumption relative to educational achievement or income [5]. However, taken as a whole, intervention approaches to mitigate the effects of low health literacy have been mixed [4]. Two plausible explanations include the deficiency of health behavior theory to guide health literacy intervention approaches and the lack of pilot studies to refine intervention messages, strategies to im- prove health literacy, and recruitment and retention ap- Copyright © 2013 SciRes. OPEN ACCESS  J. Zoellner et al. / Open Journal of Preventive Medicine 3 (2013) 51-57 52 proaches for low literate audiences [4,6]. Collectively, these findings highlight the potential of addressing SSB intake through intervention approaches guided by health behavior theory and health literacy, as well as the need for pilot studies to help advance intervention develop- ment and implementation. To date, there is limited research on how to address SSB behaviors among adults [7-9], and none of which report an underlying theoretical approach or the potential influence of health literacy status on behavior change. Likewise, no study, to date, has reported on engaging prospective participants to elicit feedback on the devel- opment of SSB intervention content and structure to en- sure that it is relevant to the target population [10]. Therefore, an important starting point for assessing the acceptability and potential effectiveness of an SSB be- havioral intervention is to gather information directly from the target population [11]. In addition to the re- finement of research methods, instrumentation, and hy- pothesis, taking advantage of opportunities to execute a patient-centered developmental process can help more fully understand patients’ receipt and value of the theory- driven intervention content and communication approaches [11,12]. The overall goals of this 5-week, 2-arm randomized controlled trial was to apply a patient-centered develop- mental process to inform the refinement of intervention content and communication approaches, as well as pilot test the effects of an intervention to decrease SSB con- sumption (SipSmartER) when compared to a matched- contact control condition targeting increasing physical activity behaviors (MoveMore). Both treatment condi- tions were guided by the Theory of Planned Behavior (TPB) [13] and concepts in health literacy [14], including media literacy [15]. Further, the structure and evaluation of the intervention was informed by the RE-AIM framework to heighten its likelihood for translation into practice by considering factors related to reach and ef- fectiveness at the individual level and the potential adop- tion, implementation, and maintenance at the organiza- tional level [16]. Hence, the primary aim of this paper is to evaluate patient feedback on intervention content and structure. The secondary aim was to understand the po- tential reach (i.e., proportion enrolled, representativeness) and effectiveness (i.e. health behaviors, theorized medi- ating variables, quality of life) of SipSmartER. Although the small sample of this pilot study limits statistical power, it was hypothesized that when compared to the matched-contact control participants, SipSmartER par- ticipants would trend towards greater decreases in SSB intake and improvements in mediating TPB-SSB vari- ables. 2. METHODS After approval by Virginia Tech’s Institutional Review Board, written informed consent was obtained prior to enrollment in October 2011. Both conditions consisted of two 90-minute small group sessions and three 5 - 10- minute telephone calls (Figure 1). Previously executed focus groups guided content development for key mes- sages [17], and program components were specifically designed to address TPB constructs including attitudes, subjective norms, percieved behavioral control, and be- havioral intentions for the referent behaviors (i.e. either SSB or PA). Integration of health literacy concepts in- cluded minimization of print materials, use of engaging visual-based activities, use of simplifed print materials written at <8th grade level, strong integration of media literacy concepts, and use of intervention staff trained in clear communication techniques. Throughout the pro- gram, participants developed and updated personalized action plans and used diaries to track behaviors. Participants were recruited via flyers and word of mouth from one community and one healthcare center in Roanoke, Virginia. Eligibility criteria included >18 years of age, English-speaking, without medical conditions that contraindicate physical activity, and consuming > 200 SSB kcals/day as assessed with the validated 15- item Beverage Questionnaire (BEVQ-15) [18]. Forty- two of sixty-three screened individuals were eligible. Twenty-five completed enrollment and were randomized to SipSmartER (n = 14) or Move More (n = 11) (Figure 1). At the end of each group session, participants com- pleted a self-administered process evaluation regarding session content and delivery which included seven 5- point likert scale questions and three open-ended ques- tions. After the program, participants completed an inter- viewer-administered qualitative assessment that included 24 semi-structured questions related to group sessions, personal action plans, diaries, and telephone calls. Outcome data collection occurred at baseline and upon completion of the program (week 6), and each took ap- proximately 45 - 60 minutes. Previously validated in- struments were utilized, including: 1) 15-item BEVQ-15 [18]; 2) 20-item Theory of Planned Behavior question- naire for SSB [19]; 3) 9-item media literacy adapted to reflect SSB [20]; and 4) 2 quality of life questions from the Centers for Disease Control and Prevention [21]. Ad- ditional baseline measures included 9 demographic ques- tions, the 6-item validated Newest Vital Sign to assess health literacy [22], and height and weight using stan- dardized protocol. Participants were provided $25 and $50 gift cards, respectively, for completing baseline and follow-up assessments. Qualitative data were coded as specific to group ses- sions, personal action plans, diaries, telephone calls, or non-specific, then coded as positive or negative, and Copyright © 2013 SciRes. OPEN ACCESS 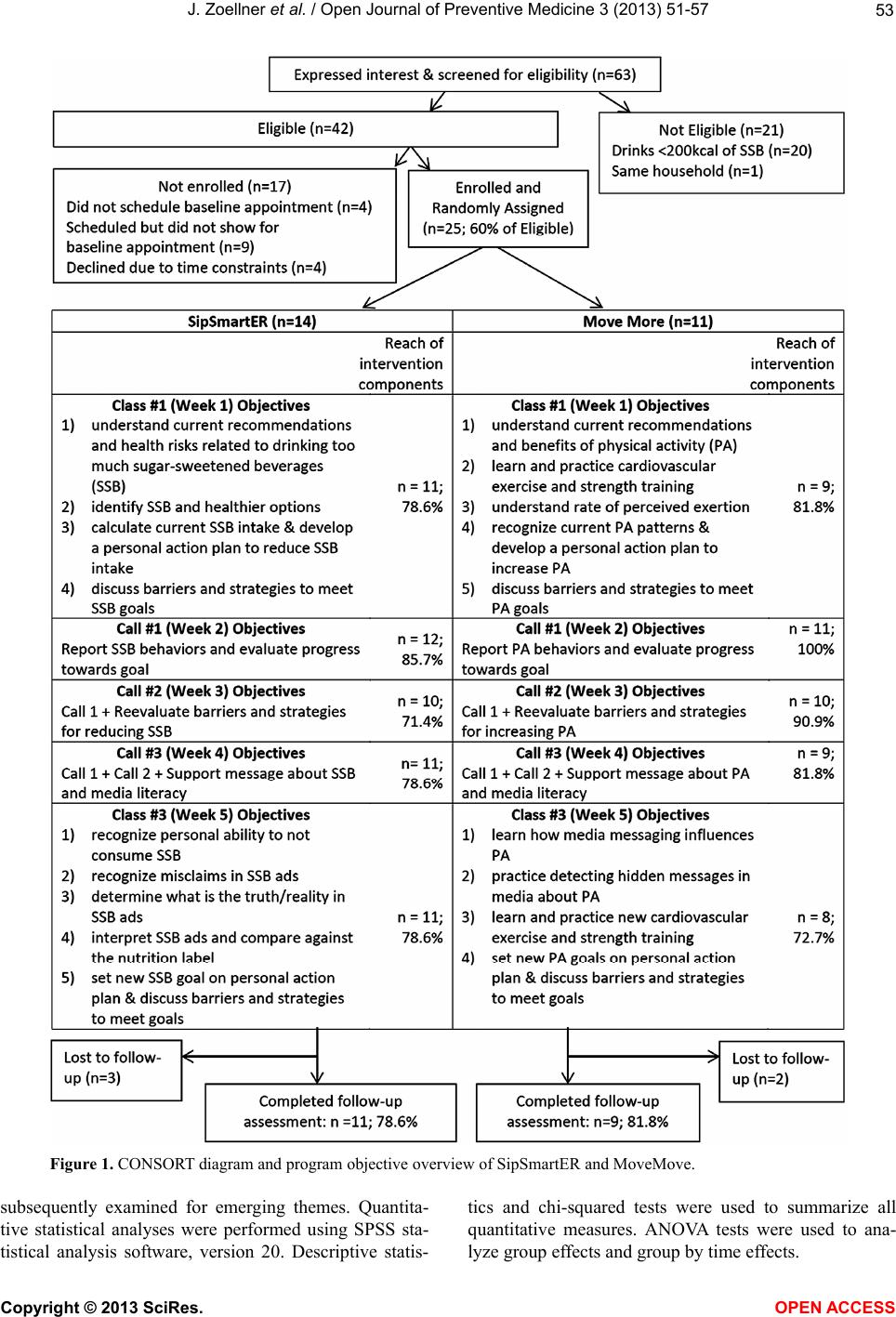 J. Zoellner et al. / Open Journal of Preventive Medicine 3 (2013) 51-57 Copyright © 2013 SciRes. 53 Figure 1. CONSORT diagram and program objective overview of SipSmartER and MoveMove. subsequently examined for emerging themes. Quantita- tive statistical analyses were performed using SPSS sta- tistical analysis software, version 20. Descriptive statis- tics and chi-squared tests were used to summarize all quantitative measures. ANOVA tests were used to ana- lyze group effects and group by time effects. OPEN ACCESS  J. Zoellner et al. / Open Journal of Preventive Medicine 3 (2013) 51-57 54 3. RESULTS Of the 25 enrolled participants, 19 (76%) were female and 6 (24%) were male. Participants’ mean age was 42 (SD = 14) years, and were primarily Caucasian (n = 13; 52%) or African American (n = 12; 48%). Nine (36%) had a high school education or less and 21 (84%) re- ported <$25,000 annual household income. Health liter- acy status indicated 6 (24%) participants with a high likelihood of limited literacy skills, 7 (28%) with a pos- sibility of limited literacy skills, and 11 (44%) with ade- quate literacy skills. Eight participants (32%) were over- weight and 16 (64%) were obese. There were no signifi- cant differences between groups for any demographic variables except education level (SipSmartER > Move- More; F = 5.57; p = 0.03). When compared to US census data, our sample appeared representative with the excep- tion that men were underrepresented, while African Americans and those with lower income or education levels were overrepresented. The conditions did not dif- fer on the reach of different intervention components (i.e., attendance, F = 0.01; p = 0.94; call completion, F = 0.91; p = 0.35; Figure 1). Related to participants’ assessment of content and structure of the group classes, mean scores were rela- tively high for both conditions and both classes, ranging from 4.2 - 5.0 on a Likert scale of 1 (strongly disagree) to 5 (strongly agree) (Ta b l e 1 ). Lesson components that were favored among SipSmartER group sessions emerged: realizing how much sugar is in beverages, recognizing the health risks associated with drinking too much sugar, understanding how much sugar they were consuming, learning about better alternatives, and learning about the media’s role in influencing SSB companies and how ad- vertisements leave out important information on health. Participants concluded that hands on activities (e.g. learning about serving sizes, counting sugar packets) were fun and engaging. Overall, participants thought group sessions were “very beneficial,” “very informa- tive,” “fun,” “captivating,” and “time well spent.” Sug- gested improvements included bringing speakers for the laptops, increasing the session duration, and encouraging more participant discussion and questions. Themes that emerged for the personal action plans were that it encouraged responsibility and accountability, offered ideas about strategies to overcome barriers, helped make goals achievable, and helped to visualize goals. The primary dislike was about the time needed to complete it. While some participants enjoyed the chal- lenge of setting and achieving goals, other participants stated this challenge as a dislike. The major positive emergent theme related to drink diaries included the accountability with tracking daily amounts of SSB. However, most participants disliked the amount of time to record behaviors and struggled with remembering to complete the diary. Most participants expressed ease when asked about figuring out SSB weekly averages, “All you have to do is add them up and divide by the days.” However, a few participants ex- pressed difficulties, “It was hard to look through each day and each time per day.” When asked about the telephone calls, SipSmartER participants concluded that they were “supportive,” “kept me motivated,” and “made it fun.” Dislikes included the timing of the calls with one participant stating, “It was hard to get calls at work or when I was driving.” Most participants liked reporting their SSB intake over the phone with one stating, “It was nice to speak with some- one and set another goal.” When asked about strategies offered over the phone, one participant stated, “They were helpful, gave me new ideas, and nothing that I had thought about before.” Only one participant stated that the calls were not helpful, because they did not have any barriers, while another participant suggested that the phone calls needed to be less scripted. Quantitatively, there was a significant time effect on a number of study outcomes (Table 1). Specifically, across groups, there were significant im- provements in SSB behaviors, SSB affective and instru- mental attitudes, SSB behavioral intention, and two me- dia literacy outcomes (meanings/messages, e.g., SSB com- panies create messages for certain purposes; representa- tion/reality, e.g., SSB commercials omit certain health information). However, SSB reduction differences be- tween SipSmartER compared to MoveMore participants were not significant (SipSmartER −256.9 + 622.6 kcals versus MoveMore −199.7 + 404.6 kcals). There were no significant differences for quality of life measures, sug- gesting no unintended or potential negative conse- quences. 4. DISCUSSION This is the first known study to engage participants in the refinement of an intervention integrating concepts from health literacy with the TPB to reduce SSB behav- iors among adults. As identified in the seminal health literacy review by Berkman and colleagues [4], pilot tested interventions, which engage the target population, result in greater effects. Similarly to conclusions by Berkman and colleagues [4], the observations of, and information gathered from representatives of the target population provided a number of key points to consider for the larger trial, including: 1) refinement of small group sessions (e.g. earlier integration of action planning, promote more participant dialogue, change duration to 120 minutes); 2) incorporate explicit teach back methods in the calls (e.g. assess understanding of SSB types, servings sizes, calculating averages) to add clarity to the instructions and learning materials, as well as reduce Copyright © 2013 SciRes. OPEN ACCESS 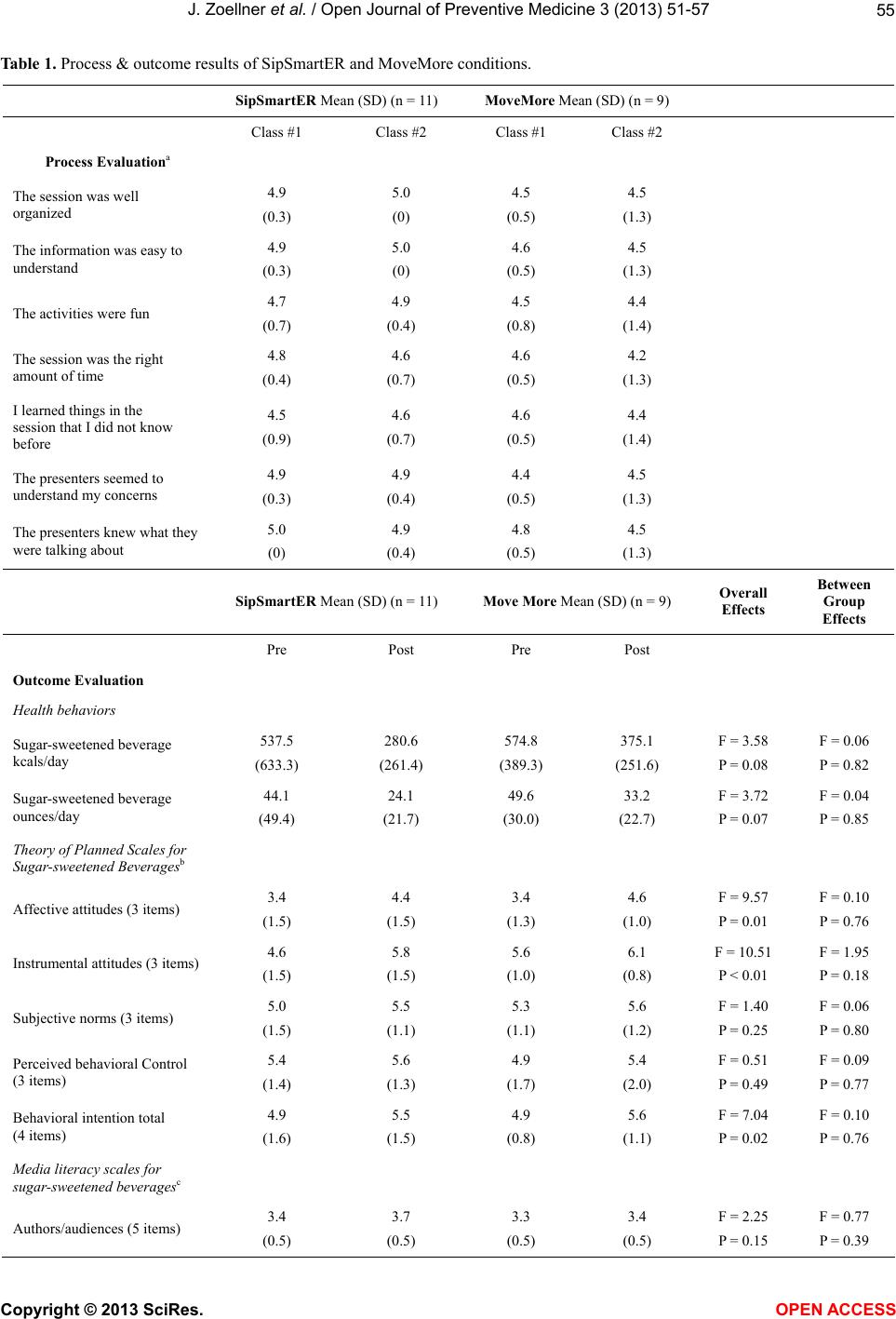 J. Zoellner et al. / Open Journal of Preventive Medicine 3 (2013) 51-57 Copyright © 2013 SciRes. OPEN ACCESS 55 Table 1. Process & outcome results of SipSmartER and MoveMore conditions. SipSmartER Mean (SD) (n = 11) MoveMore Mean (SD) (n = 9) Class #1 Class #2 Class #1 Class #2 Process Evaluationa The session was well organized 4.9 (0.3) 5.0 (0) 4.5 (0.5) 4.5 (1.3) The information was easy to understand 4.9 (0.3) 5.0 (0) 4.6 (0.5) 4.5 (1.3) The activities were fun 4.7 (0.7) 4.9 (0.4) 4.5 (0.8) 4.4 (1.4) The session was the right amount of time 4.8 (0.4) 4.6 (0.7) 4.6 (0.5) 4.2 (1.3) I learned things in the session that I did not know before 4.5 (0.9) 4.6 (0.7) 4.6 (0.5) 4.4 (1.4) The presenters seemed to understand my concerns 4.9 (0.3) 4.9 (0.4) 4.4 (0.5) 4.5 (1.3) The presenters knew what they were talking about 5.0 (0) 4.9 (0.4) 4.8 (0.5) 4.5 (1.3) SipSmartER Mean (SD) (n = 11) Move More Mean (SD) (n = 9) Overall Effects Between Group Effects Pre Post Pre Post Outcome E valuation Health behaviors Sugar-sweetened beverage kcals/day 537.5 (633.3) 280.6 (261.4) 574.8 (389.3) 375.1 (251.6) F = 3.58 P = 0.08 F = 0.06 P = 0.82 Sugar-sweetened beverage ounces/day 44.1 (49.4) 24.1 (21.7) 49.6 (30.0) 33.2 (22.7) F = 3.72 P = 0.07 F = 0.04 P = 0.85 Theory of Planned Scales for Sugar-sweetened Beveragesb Affective attitudes (3 items) 3.4 (1.5) 4.4 (1.5) 3.4 (1.3) 4.6 (1.0) F = 9.57 P = 0.01 F = 0.10 P = 0.76 Instrumental attitudes (3 items) 4.6 (1.5) 5.8 (1.5) 5.6 (1.0) 6.1 (0.8) F = 10.51 P < 0.01 F = 1.95 P = 0.18 Subjective norms (3 items) 5.0 (1.5) 5.5 (1.1) 5.3 (1.1) 5.6 (1.2) F = 1.40 P = 0.25 F = 0.06 P = 0.80 Perceived behavioral Control (3 items) 5.4 (1.4) 5.6 (1.3) 4.9 (1.7) 5.4 (2.0) F = 0.51 P = 0.49 F = 0.09 P = 0.77 Behavioral intention total (4 items) 4.9 (1.6) 5.5 (1.5) 4.9 (0.8) 5.6 (1.1) F = 7.04 P = 0.02 F = 0.10 P = 0.76 Media literacy scales for sugar-sweetened beveragesc Authors/audiences (5 items) 3.4 (0.5) 3.7 (0.5) 3.3 (0.5) 3.4 (0.5) F = 2.25 P = 0.15 F = 0.77 P = 0.39  J. Zoellner et al. / Open Journal of Preventive Medicine 3 (2013) 51-57 56 Continued Meanings/messages (9 items) 3.5 (0.4) 3.8 (0.3) 3.3 (0.5) 3.7 (0.3) F = 16.06 P < 0.01 F = 0.05 P = 0.83 Representation/reality (5 items) 3.4 (0.6) 3.8 (0.3) 3.3 (0.7) 3.5 (0.5) F = 4.31 P = 0.05 F = 0.57 P = 0.46 Quality of life Rate your general healthd 2.7 (0.6) 2.9 (1.0) 2.8 (1.3) 2.8 (1.0) F = 0.31 P = 0.59 F = 0.31 P = 0.59 In past 30 day, how many days did poor physical or mental health keep you from usual activities 5.3 (8.9) 5.6 (9.0) 5.2 (10.5) 6.1 (10.2) F = 0.87 P = 0.36 F = 0.12 P = 0.74 aReported on a 5-point Likert Scale: 1 = strongly disagree, 5 = strongly agree. bReported on a 5-point Likert Scale: 1 = worse, 5 = better attitudes, subjective norms, perceived behavioral control, behavioral intentions. cReported on a 4-point Likert Scale: 1 = definetly no, 4 = definetly yes. dReported on a 5-point Likert Scale: 1 = excellent, 5 = poor. recall bias and variability while addressing the sensitivity of the primary outcome measure; and 3) refinement of recruitment and enrollment protocols. The value of using a patient-centered approach in the developmental phases of this theory-guided SSB behavioral intervention was apparent. In general, the behavior change, while not signifi- cantly different between groups, trended in the direction hypothesized (i.e. greater SSB improvements in the SipSmartER as compared to the MoveMore). Being made aware of the study purpose through informed con- sent procedures and the repeated exposure to SSB rec- ommendations through the assessment process may have prompted SSB improvements in the control group. This is consistent with the literature on mere-measurement effects, which demonstrates short-term (but not long- term) behavioral responses to sets of questions related to measurement of behavioral and psychosocial constructs similar to those proposed in our study [23]. It is hypothe- sized that an adequately powered trial, of longer duration and timing between data assessment points, will over- come this challenge. The RE-AIM approach for planning the intervention seemed to be successful in creating a structure that could consistently reach the study sample and including con- tent that they enjoyed [16]. This initial feedback from participants provides promising directions for under- standing the reach (including representativeness) and effectiveness of a TPB and health literacy-based SSB intervention. Future evaluative efforts will include as- sessing reach, effectiveness, adoption, implementation, and maintenance to promote comprehensive understand- ing of internal and external validity factors, as well as potential public health impact of a large-scale trial to reduce SSB. 5. ACKNOWLEDGEMENTS We acknowledge the research support provided by Terri Corsi, Sarah Wall, Valisa Hedrick, Lauren Noel, Angie Bailey, Ramine Alexander, and Felicia Reese. We are particularly grateful for contributions from Eileen Lepro at New Horizons Healthcare and staff at the Presbyterian Community Center. This research was funded, in part, by National Institutes of Health/National Cancer Institute 1R01CA154364-01A1 (Zoellner, PI). REFERENCES [1] Duffey, K.J. and Popkin, B.M. (2007) Shifts in patterns and consumption of beverages between 1965 and 2002. Obesity, 15, 2739-2747. doi:10.1038/oby.2007.326 [2] Vartanian, L.R, Schwartz, M.B. and Brownell, K.D. (2007) Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. American Journal of Public Health, 97, 667-675. doi:10.2105/AJPH.2005.083782 [3] Nielsen-Bohlman, L., Panzer, A.M. and Kindig, D.A. (2004) Health Literacy: A Prescription to End Confusion. National Academies Press,Washington DC. [4] Berkman, N.S.S., Donahue, K., et al. (2011) Health liter- acy interventions and outcomes: An update of the literacy and health outcomes systematic review of the literature. RTI International-University of North Carolina Evidence- Based Practice Center, Chapel Hill. [5] Zoellner, J., You, W., Connell, C., et al. (2011) Health literacy is associated with Healthy Eating Index scores and sugar-sweetened beverage intake: Findings from the rural lower Mississippi Delta. Journal of American Die- tetic Association , 111, 1012-1020. doi:10.1016/j.jada.2011.04.010 [6] Allen, K., Zoellner, J., Motley, M., et al. (2010) Under- standing the internal and external validity of health liter- acy interventions: A systematic literature review using the RE-AIM framework. The Journal of Health Communica- tion, 16, 55-72. doi:10.1080/10810730.2011.604381 [7] Tate, D.F., Turner-McGrievy, G., Lyons, E., et al. (2012) Replacing caloric beverages with water or diet beverages for weight loss in adults: Main results of the Choose Copyright © 2013 SciRes. OPEN ACCESS  J. Zoellner et al. / Open Journal of Preventive Medicine 3 (2013) 51-57 57 Healthy Options Consciously Everyday (CHOICE) ran- domized clinical trial. American Journal of Clinical Nu- trition, 95, 555-563. doi:10.3945/ajcn.111.026278 [8] Stookey, J.D., Constant, F., Popkin, B.M., et al. (2008) Drinking water is associated with weight loss in over- weight dieting women independent of diet and activity. Obesity, 16, 2481-2488. doi:10.1038/oby.2008.409 [9] Chen, L.W., Appel, L.J., Loria, C., et al. (2009) Reduc- tion in consumption of sugar-sweetened beverages is as- sociated with weight loss: The PREMIER trial. American Journal of Clinical Nutrition, 89, 1299-1306. doi:10.3945/ajcn.2008.27240 [10] Wen, K.-Y., Miller, S.M., Stanton, A.L., et al. (2012) The development and preliminary testing of a multimedia pa- tient-provider survivorship communication module for breast cancer survivors. Patient Education and Counsel- ing, 88, 344-349. doi:10.1016/j.pec.2012.02.003 [11] Helfand, M., Berg. A., Flum, D., et al. (2012) Draft Meth- odology report: Our questions, our decisions: Standards for patient-centered outcomes research. http://pcori.org/assets/MethodologyReport-Comment.pdf [12] Venetis, M.K., Robinson, J.D. Turkiewicz, K.L., et al. (2009) An evidence base for patient-centered cancer care: A meta-analysis of studies of observed communication be- tween cancer specialists and their patients. Patient Edu- cation and Counseling, 77, 379-383. doi:10.1016/j.pec.2009.09.015 [13] Ajzen, I. (1985) From intentions to actions: A theory of planned behavior. In: Kuhl, J. and Beckmann, J., Eds., Action-Control: From Cognition to Behavior, Springer, Heidelberg, 11-39. [14] Zarcadoolas, C., Pleasant, A. and Greer, D. (2006) Ad- vancing health literacy: A framework for understanding and action. Jossey-Bass, San Francisco. [15] Aufderheide, P. (1993) Part II: Conference Proceedings and Next Steps. Communications and Society Program of the Aspen Institute, Washington DC. [16] Glasgow, R.E., Vogt, T.M. and Boles, S.M. (1999) Evalu- ating the public health impact of health promotion inter- ventions: The RE-AIM framework. American Journal of Public Health, 89, 1322-1327. doi:10.2105/AJPH.89.9.1322 [17] Zoellner, J., Krzeski, E., Harden, S., et al. (2012) Qualita- tive application of the theory of planned behavior to un- derstand beverage consumption behaviors among adults. Journal of the Academy of Nutrition and Dietetics, 112, 1774-1784. doi:10.1016/j.jand.2012.06.368 [18] Hedrick, V.E., Savla, J., Comber, D.L., et al. (2012) De- velopment of a brief questionnaire to assess habitual bev- erage intake (BEVQ-15): Sugar-sweetened beverages and total beverage energy intake. Journal of the Academy of Nutrition and Dietetics, 112, 840-849. doi:10.1016/j.jand.2012.01.023 [19] Zoellner, J., Estabrooks, P., Davy, B., et al. (2012) Ex- ploring the theory of planned behavior to explain sugar- sweetened beverage consumption. Journal of Nutrition Education and Behavior, 44, 172-177. doi:10.1016/j.jneb.2011.06.010 [20] Primack, B.A., Gold, M.A., Switzer, G.E., et al. (2006) Development and validation of a smoking media literacy scale for adolescents. Archives of Pediatric and Adoles- cent Medicine, 160, 369-374. doi:10.1001/archpedi.160.4.369 [21] Klesges, R., Eck, L., Mellon, M., et al. (1990) The accu- racy of self-reports of physical activity. Medical Science Sports and Exercise, 22, 690-697. doi:10.1249/00005768-199010000-00022 [22] Weiss, B., Mays, M., Martz, W., et al. (2005) Quick as- sessment of literacy in primary care: The newest vital sign. Annuals of Family Medicine, 3, 514-522. doi:10.1370/afm.405 [23] Levav, J. and Fitzsimons, G. (2006) When questions change behavior: The role of ease representation. Phy- scological Science, 17, 207-213. Copyright © 2013 SciRes. OPEN ACCESS
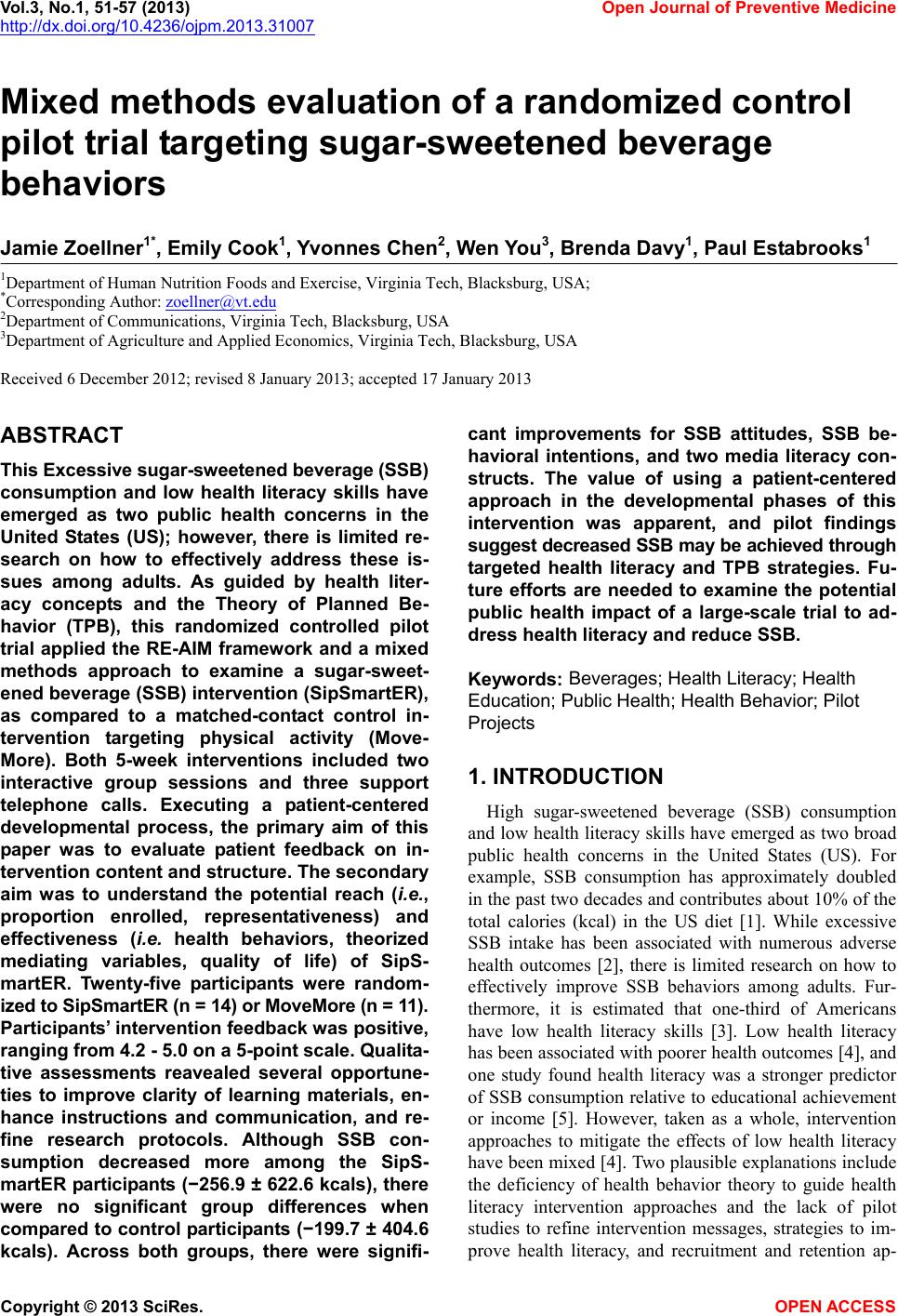
|