Paper Menu >>
Journal Menu >>
 Engineering, 2012, 5, 46-49 doi:10.4236/eng.2012.410B012 Published Online October 2012 (http://www.SciRP.org/journal/eng) Copyright © 2012 SciRes. ENG A Comparison of Pinch Force between Finger and Palm Grasp tec hniques i n L ap aroscopic G ras ping Susmitha Wi ls K1,4, George Mathew2, M. Manivannan3, Suresh R Devasahayam4 1Department of Biotechnology, Indian Institute of Technology Madras, India 2Faculty of Medicine, Universitas Pelita Harapan, Indonesia 3Department of Applied Mechanics, Indian Institute of Technology Madras, India 4Depar tm ent of Bio engineer ing , Chris tian Med ica l Co lleg e Vellore, I ndia Email: swilswk@gmail.com Received 2012 ABSTRACT Laparoscopic surgery is a new abdominal surgical procedure which helps the patients in many ways like less hospital stay, faster recovery and reduced pain. The main disadvantage in this surgical procedure is the reduced haptic perception by the surgeons due to the usage of laparoscopic instrument to handle tissues which in turn cause damage of it as compared to an open surgery. The primary aim of this investigation was to compare the pinch force applied during two different methods of laparoscopic grasping: Finger and Palm grasp. A low cost force sensing resistor tailor made for the grasper tip was designed and fabricated for quantifying the grasper tip force in the study. The results indicate more pinch force was applied during palm grasp as compared to finger grasp so as to pre- vent the slippage of the tiss ues from the jaws of the laparoscopic grasper s. Keywords: Pinch Force; Grasp ing; Laparoscopic Surgery; Fo r ce Sensing Resistor; Laparoscopic Grasper 1. Introduction Minimally Invasive Surgery (MIS) is a modern surgical proce- dure, which has made its presence felt since three decades and is slowly replacing the conventional open surgery. Laparoscop- ic surgery (LS) is one of the MIS techniques done in the abdo- men with 3-4 small incisions through which surgeons insert long handled laparoscopic instruments and laparoscope so as to manipulate the target organ in the abdominal cavity [1,2].The use of long handled instruments leads to reduced haptic percep- tion which in turn may result in excess force being delivered at the target tissue cau sing un wanted ti ssue damage. Laparo scop ic graspers are one of the most indispensable instruments used for grasping the target tissue in any laparoscopic procedure. The force involved while grasping an object is the pinch force and it’s defined as the force with which an individual holds/ grasps an object without letting it slip off the grasper jaws. There are two methods of grasping: Palm and Finger grasp [3]. In palm grasp (Figure 1(a)), the palm of the operating hand rest on the ring of the movable handle with the fingers 2-5 on the fixed hand while in the finger grasp (Figure 1(b)), the thumb will be inside the ring of the movable handle with other fingers on the fixed hand opposing the thumb. Sensorized laparoscopic tool with/without modification of a commercial tool were used in various studies related to force measurements [4-11]. Different types of force sensors used in the MIS techniques with respect to their size, sterilizability etc were explained in [12]. The objective of our study was to find whether there is any significant difference in pinch force during finger and palm grasping techniques in the laparoscopic surgic- al setup. In this study an efficient force measurement arrange- ment was setup using a cost effective custom made force sens- ing resistor for tip pinch force sensing and strain gauges for handle pinch force measurements. 2. Materials and Methods An atraumati c fenestr ated lap aros cop ic grasp er was us ed for th e finger and palm grasp pin ch force experiment. The grasper was sensorized (Figure 2) and it consists of two force sensors. One sensor was on the handle and another on the tip of the grasper. Custom made force sensing resistor (FSR) was used as tip pinch force sensor. FSR was developed with conductive foam sandwiched between the copper sheets an d wires sold ered on to these sheets were connected to the preamplifier circuit. The sensor was designed in such a way that it fits to the grasper tip and dimension was 2.2x0.4x0.1cm. The custom made FSR ex- hibits decrease in the resistance as the applied force increases. The sensor was calibrated by placing known weights on it and has a sensitivity of 0.224V/N. Silicone gel and plastic sheet were used to insulate the sensor from the conductive grasper tip. In addition to the above sensor arrangement on the grasper, strain gauge senso rs were attach ed to the handl e of it to get t he handle pinch force. The handle of the grasper was assumed as a Figure 1. Picture showing (a) Palm grasping technique (b) Finger grasping techni que usi ng lapar os cop i c grasp er. 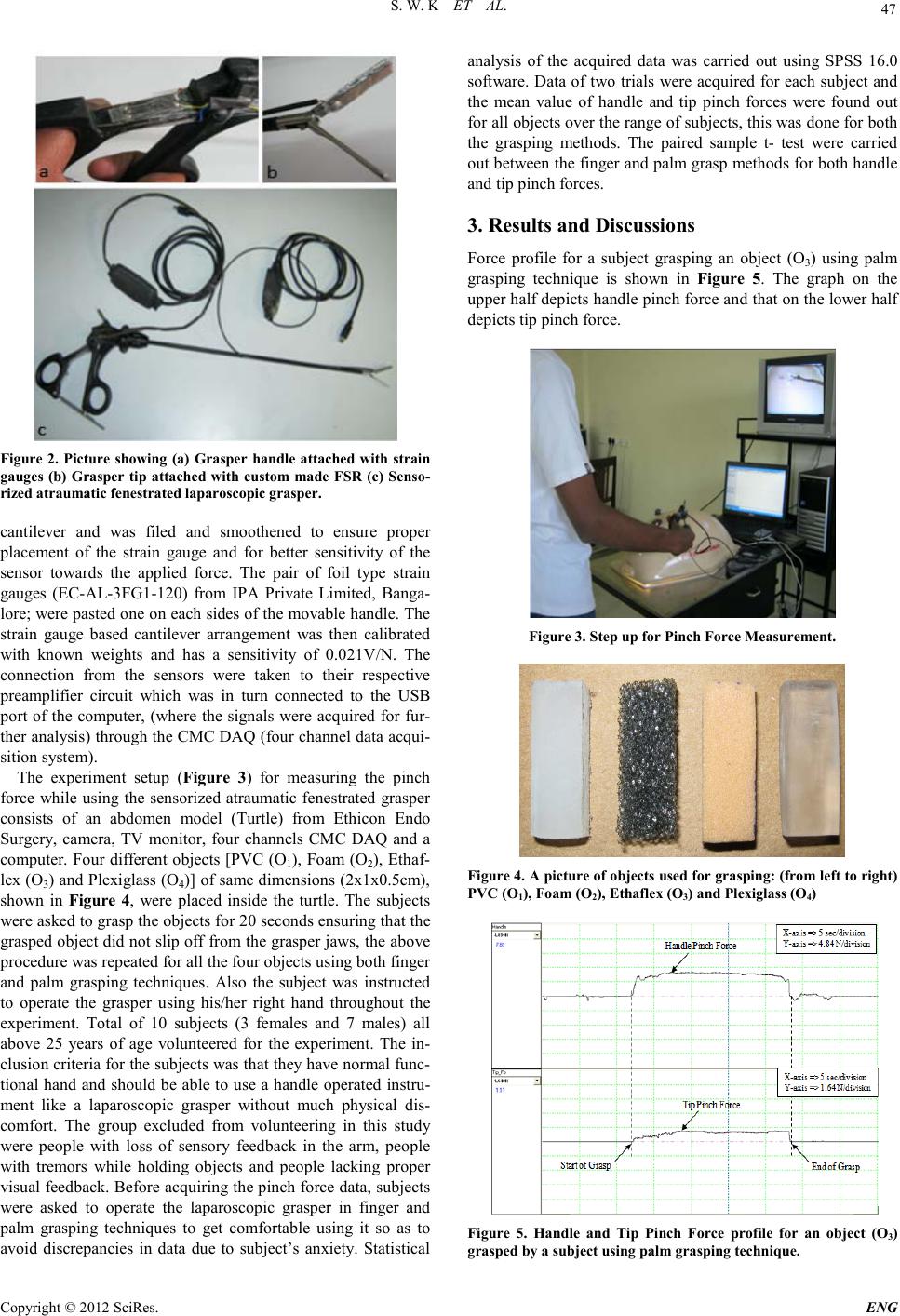 S. W. K ET AL. Copyright © 2012 SciRes. E NG 47 Figure 2. Picture showing (a) Grasper handle attached with strain gauges (b) Grasper tip attached with custom made FSR (c) Senso- rized atraumat ic fenest rated l ap a ro scopic grasp e r. cantilever and was filed and smoothened to ensure proper placement of the strain gauge and for better sensitivity of the sensor towards the applied force. The pair of foil type strain gauges (EC-AL-3 FG1-120) from IPA Private Limited, Banga- lore; were pasted one on each sides of the movable handle. The strain gauge based cantilever arrangement was then calibrated with known weights and has a sensitivity of 0.021V/N. The connection from the sensors were taken to their respective preamplifier circuit which was in turn connected to the USB port of the computer, (where the signals were acquired for fur- ther an alysis) through th e CMC DAQ (four ch annel data acqui- sition system). The experiment setup (Figure 3) for measuring the pinch force while using the sensorized atraumatic fenestrated grasper consists of an abdomen model (Turtle) from Ethicon Endo Surgery, camera, TV monitor, four channels CMC DAQ and a computer. Four different objects [PVC (O1), Foam (O2), Ethaf- lex (O3) and Plexiglas s (O4)] of same dimensions (2x1x0.5cm), shown in Figure 4, were placed inside the turtle. The subjects were asked to grasp the objects for 20 seconds ensuring that the grasped object did not slip off from the grasper jaws, the above procedure was repeated for all the four objects using both finger and palm grasping techniques. Also the subject was instructed to operate the grasper using his/her right hand throughout the experiment. Total of 10 subjects (3 females and 7 males) all above 25 years of age volunteered for the experiment. The in- clusio n criteri a for the subject s was that they have normal func- tional hand and should be able to use a handle operated instru- ment like a laparoscopic grasper without much physical dis- comfort. The group excluded from volunteering in this study were people with loss of sensory feedback in the arm, people with tremors while holding objects and people lacking proper visual feedb ack. Before acq uiring the pin ch force data, subjects were asked to operate the laparoscopic grasper in finger and palm grasping techniques to get comfortable using it so as to avoid discrepancies in data due to subject’s anxiety. Statistical analysis of the acquired data was carried out using SPSS 16.0 software. D ata of two tr ials were acquired for each subject and the mean value of handle and tip pinch forces were found out for all objects over the range of subjects, this was done for both the grasping methods. The paired sample t- test were carried out between the finger and palm grasp methods for both handle and tip pinch forces. 3. Results and Discussions Force profile for a subject grasping an object (O3) using palm grasping technique is shown in Figure 5. The graph on the upper half depicts handle pinch force and that on the lower half depicts tip pinch force. Figure 3. Step up for Pinch Force Measurement. Figure 4. A pictu re of objects used for gras ping: (from left to right) PVC (O1), Foam (O2), Ethaflex (O3) and Pl exigla s s (O4) Figure 5. Handle and Tip Pinch Force profile for an object (O3) grasped by a subject usi ng palm grasping technique. 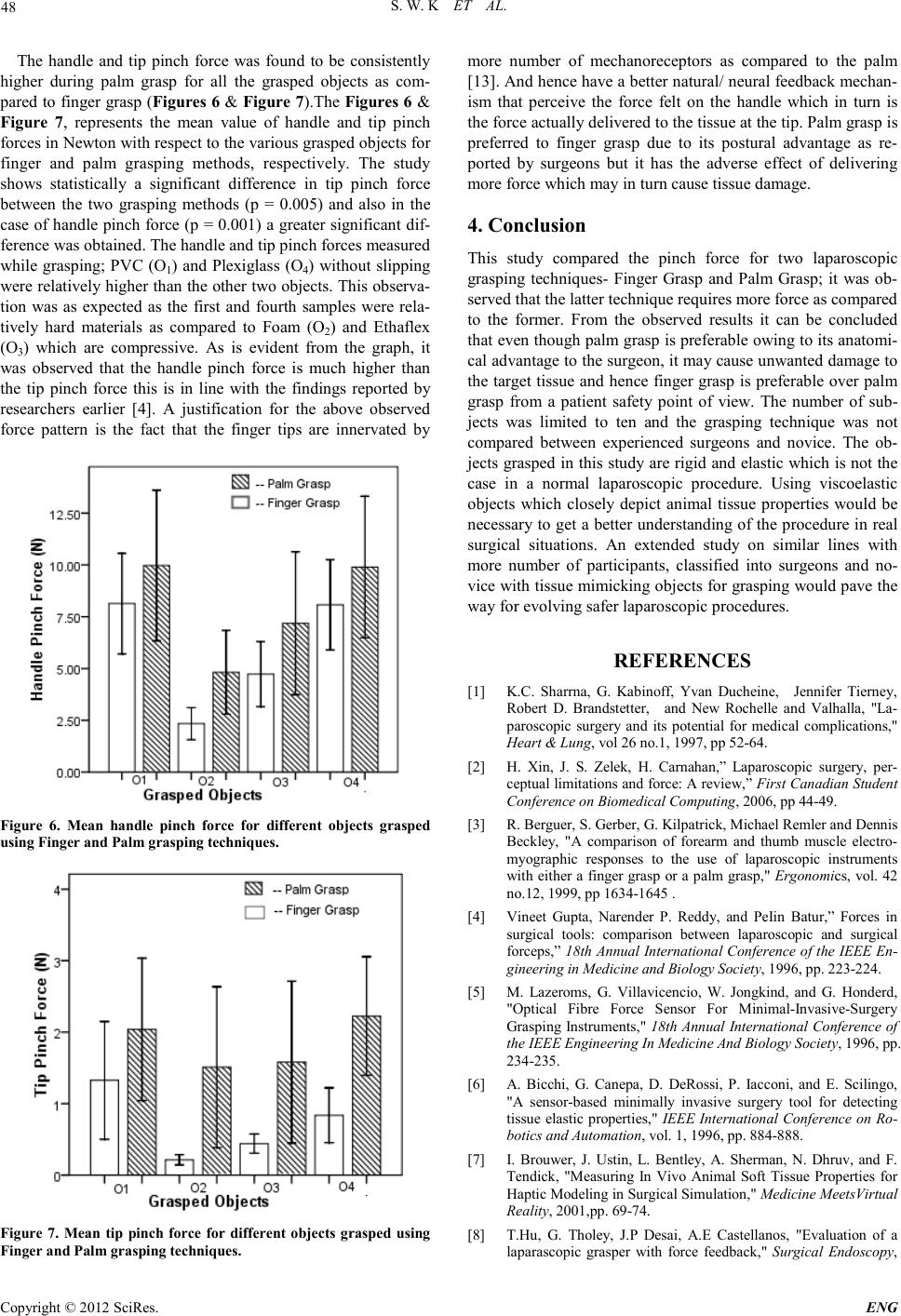 S. W. K ET AL. Copyright © 2012 SciRes. ENG 48 The handle and tip pinch force was found to be consistently higher during palm grasp for all the grasped objects as com- pared to finger grasp (Figures 6 & Figure 7).The Figures 6 & Figure 7, represents the mean value of handle and tip pinch forces in Newton with respect to the various grasped objects for finger and palm grasping methods, respectively. The study shows statistically a significant difference in tip pinch force between the two grasping methods (p = 0.005) and also in the case of hand le pinch force (p = 0.001) a greater sign ificant dif- ference was obtained. The handle and tip pinch forces measured while grasping; PVC (O1) and Plexiglass (O4) without slipping were relati vely higher th an the other two obj ects. This observa- tion was as expected as the first and fourth samples were rela- tively hard materials as compared to Foam (O2) and Ethaflex (O3) which are compressive. As is evident from the graph, it was observed that the handle pinch force is much higher than the tip pinch force this is in line with the findings reported by researchers earlier [4]. A justification for the above observed force pattern is the fact that the finger tips are innervated by Figure 6. Mean handle pinch force for different objects grasped using Finger and Palm graspi ng techniques . Figure 7. Mean tip pinch force for different objects grasped using Finger and Palm grasping techniques. more number of mechanoreceptors as compared to the palm [13] . And hence have a b etter n atural/ n eural feedback mechan- ism that perceive the force felt on the handle which in turn is the force act ual ly delivered to the t issu e at the tip. P alm grasp is preferred to finger grasp due to its postural advantage as re- ported by surgeons but it has the adverse effect of delivering more force which may in tur n cause t issue d amage. 4. Conclusion This study compared the pinch force for two laparoscopic grasping techniques- Finger Grasp and Palm Grasp; it was ob- served that the latter technique requ ires more forc e as compared to the former. From the observed results it can be concluded that even though palm grasp is preferable owing to its anatomi- cal advant age to th e surgeon, it may cause un wanted d amage to the target tissue and h ence finger grasp is preferabl e over palm grasp from a patient safety point of view. The number of sub- jects was limited to ten and the grasping technique was not compared between experienced surgeons and novice. The ob- jects grasped in th is study are rigid and elast ic which is not the case in a normal laparoscopic procedure. Using viscoelastic objects which closely depict animal tissue properties would be necessary to get a better understanding of the procedure in real surgical situations. An extended study on similar lines with more number of participants, classified into surgeons and no- vice with tissue mimicking objects for grasping would pave the way for evolving safer laparoscopic procedures. REFERENCES [1] K.C. Sharrna, G. Kabinoff, Yvan Ducheine, Jennifer Tierney, Robert D. Brandstetter, and New Rochelle and Valhalla, "La- paroscopic surgery and its potential for medical complications," Heart & Lung, vol 26 no.1, 199 7, pp 52-64. [2] H. Xin, J. S. Zelek, H. Carnahan,” Laparoscopic surgery, per- ceptual limitations and force: A review,” First Can adian S tu dent Conf er enc e on Biom edical C om put in g, 2006, pp 44-49. [3] R. Berguer , S. Gerber, G. Kilpatrick, Michael Remler and Dennis Beckley, "A comparison of forearm and thumb muscle electro- myographic responses to the use of laparoscopic instruments with eit her a finger grasp or a pa lm grasp," Ergonomics, vol. 42 no.12, 1999, pp 1634-1645 . [4] Vineet Gupta, Narender P. Reddy, and PeIin Batur,” Forces in surgical tools: comparison between laparoscopic and surgical forceps,” 18th Annual International Conference of the IEEE En- gineering in Medicine and Biology Society, 1996, pp. 223-224. [5] M. Lazeroms, G. Villavicencio, W. Jongkind, and G. Honderd, "Optical Fibre Force Sensor For Minimal-Invasive-Surgery Grasping Instruments," 18th Annual Inte rnational Conf erence of the IEEE Engineering In Medicine And Biology Society, 1996, pp. 234-235. [6] A. Bicchi, G. Canepa, D. DeRossi, P. Iacconi, and E. Scilingo, "A sensor-based minimally invasive surgery tool for detecting tissue elastic properties," IEEE Inte rnation al Conference on Ro- boti cs and Au tomat ion, vol. 1, 1996, pp. 884-888. [7] I. Brouwer, J. Ustin, L. Bentley, A. Sherman, N. Dhruv, and F. Tendick, "Measuring In Vivo Animal Soft Tissue Properties for Haptic Modeling in Surgical Simulation," Medicine MeetsVirtual Reality, 2001,pp. 69-74. [8] T. Hu, G. Thole y, J.P Desai, A.E Castellanos, "Evaluation of a laparascopic grasper with force feedback," Surgical Endoscopy,  S. W. K ET AL. Copyright © 2012 SciRes. E NG 49 2004, pp. 863-867. [9] K. Ikuta, T. Kato, H. Ooe, S. Ando, "Surgery Recorder System for recording position and force of forceps during Laparoscopic Surgery," IEEE International conference on ASME, 2007, pp. 1-6. [10] E.P.Westebring-van der Putten, J.J. Dobbelsteen, R.H.M. Goos- sens, J.J. Jakimowicz, and J. Dankelman, "Effect of laparoscopic grasper force transmission ratio on grasp control," Surgical En- doscopy, 2009, pp. 818 -824. [11] M. Ramezanifard, J. Dargahi, S. Najarian, and N. Narayanan, "Design , Modeling and Fabri cation of a Tact ile Sensor and Di s- play System for Application in Laparoscopic Surgery," Engi- neering and Technology , 2009, pp. 209-213. [12] A.L. Trejos, R.V. Patel, and M.D. Naish, "Force sensing and its application in minimally invasive surgery and therapy: a survey," Journal of Mechanical Engineering Science, vol. 224, 2010 , pp. 1435-1454. [13] Robert F.Schmidt,”Fundamentals of Sensory Physiology,” Ed. Berl in: Spri nger-Verl ag, 1981, p p 81-83. |