M. KHODAYARIFARD, S. A. ZARDKHANEH
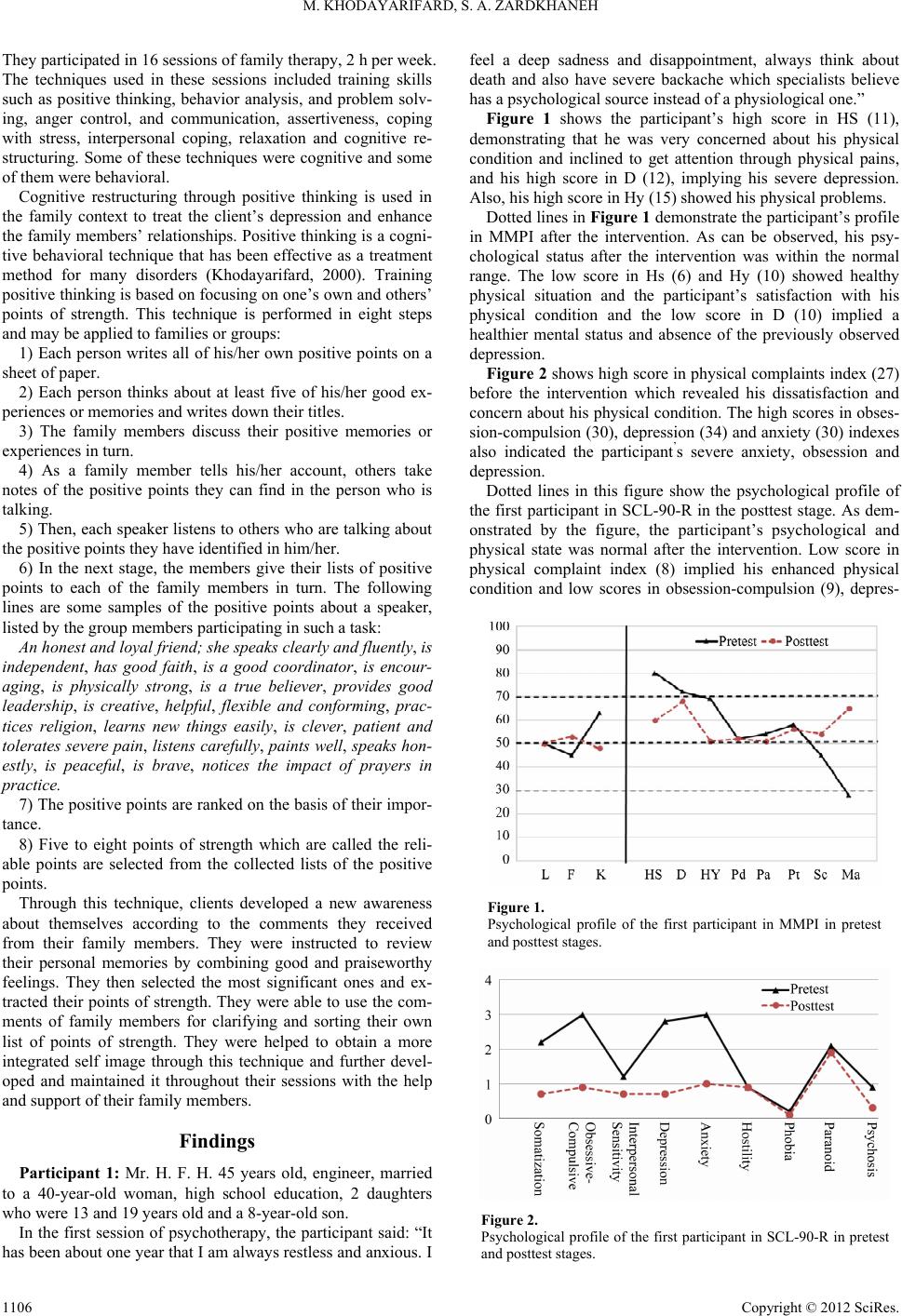
observed that family therapy based on cognitive behavioral
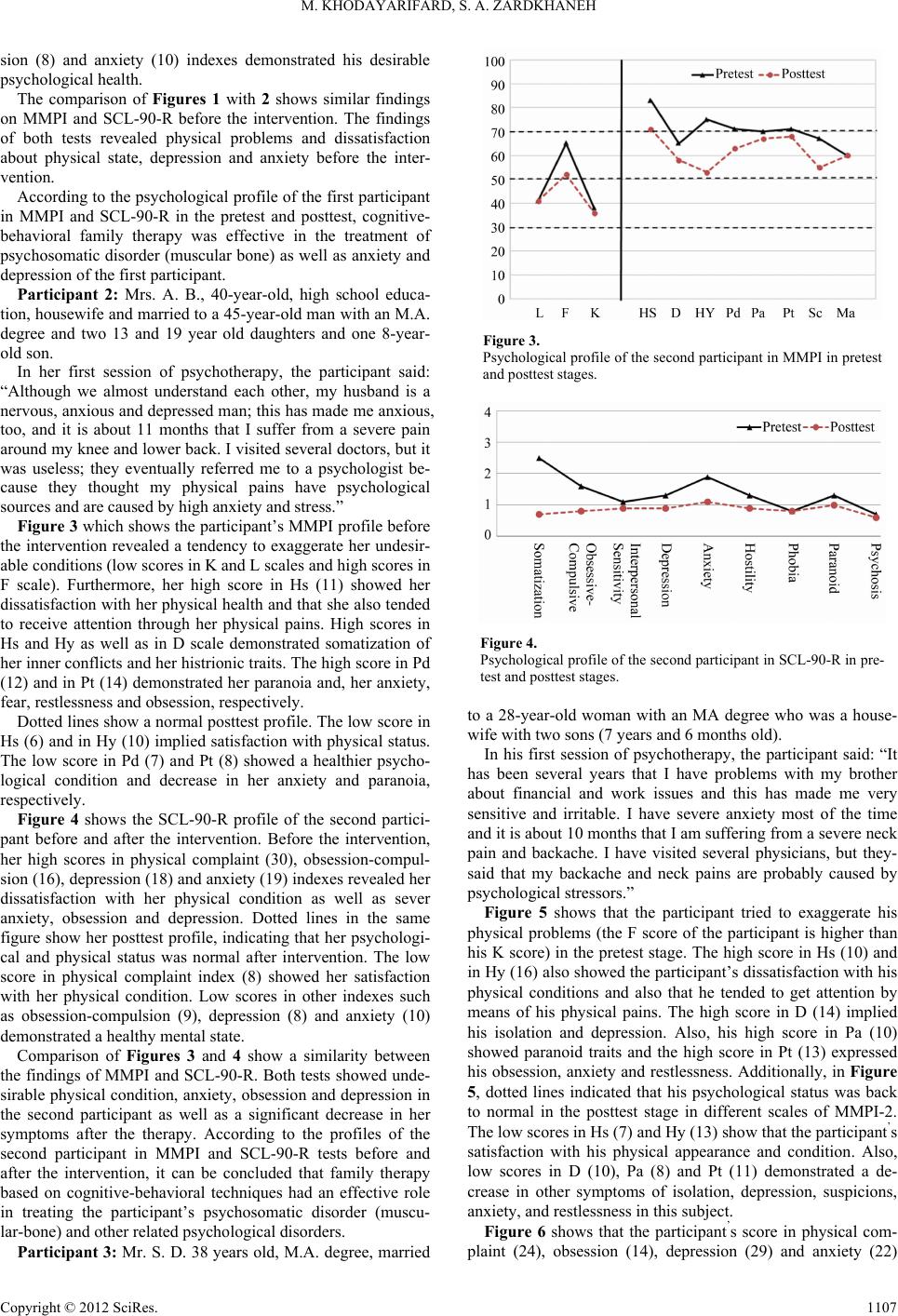
techniques can be effective in treating children who have psy-
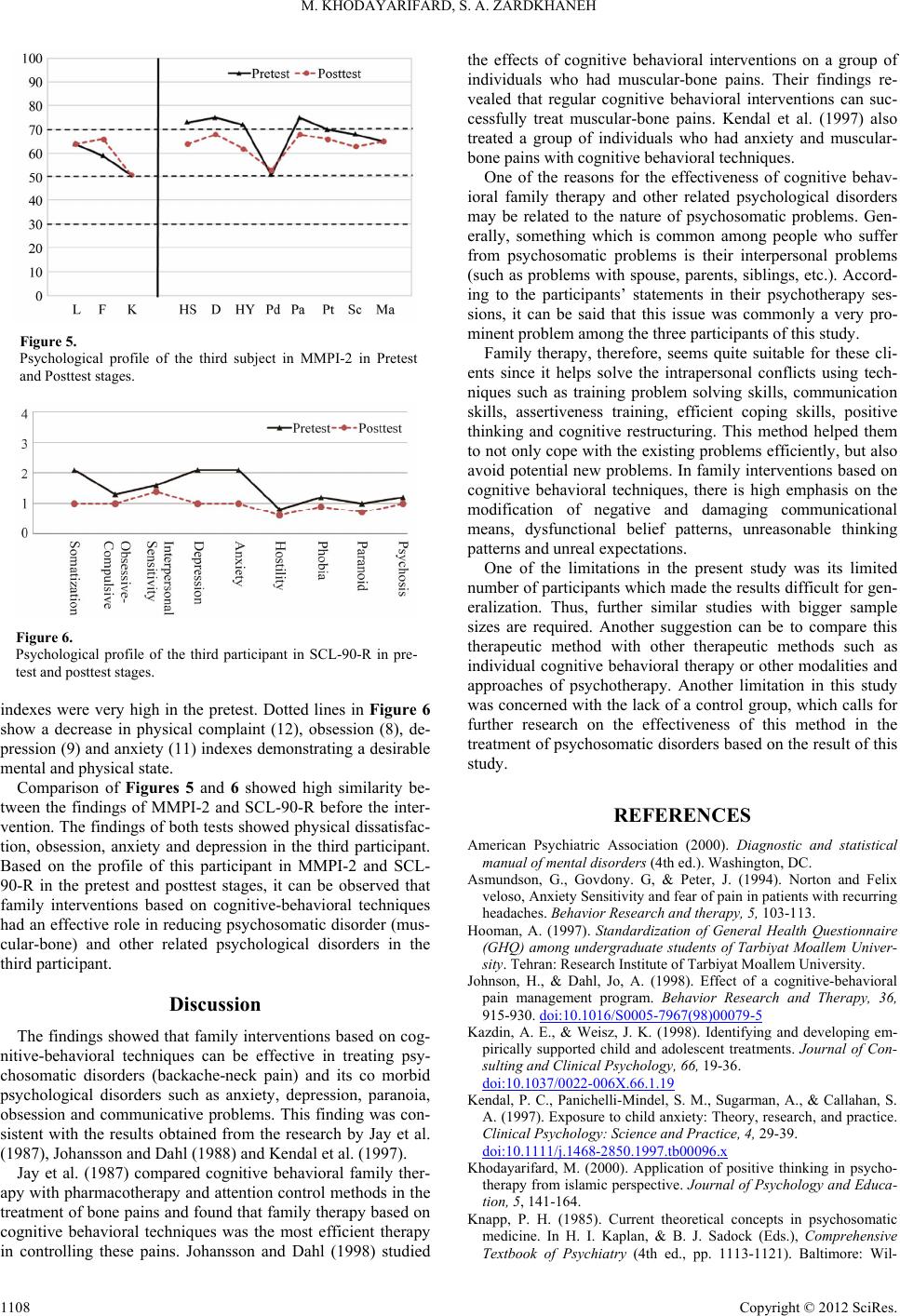
chosomatic disorders. Leibman et al. (1974) used cognitive
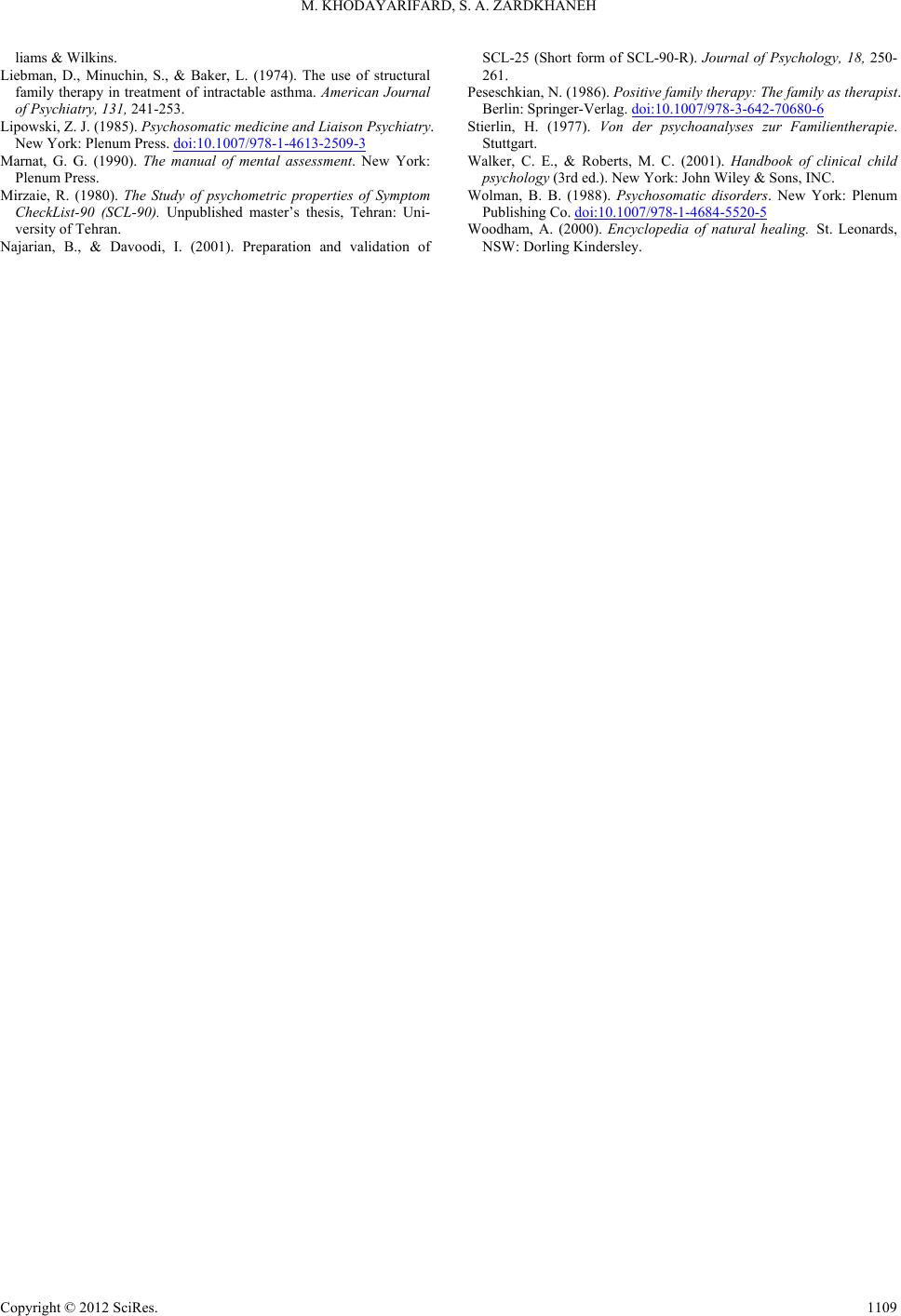
behavioral techniques for treating a group of children who had
severe asthma. In this psychosomatic disorder, the primary
allergic tendency in the patient can be combined with emotional
factors and, particularly with family problems and conflicts.
The members of a family are all elements of an interactive
system in which one individual constantly influences and is
influenced by all other members (Stierlin, 1977). Therefore, a
symptom can be only understood within the framework and
web of relationships in which that symptom is expressed. This
is especially true for psychic and psychosomatic illnesses. The
role that the symptom plays within the family, within its rules
of conduct and within its social context can be only understood
considering this viewpoint (Peseschkian, 1986).
Cognitive behavioral family therapy aims at reducing the
symptoms as well as changing the dysfunctional family struc-
ture and roles through cognitive behavioral approach. This
approach consists of different techniques such as training
communication skills, problem solving, relaxation and reward-
ing system management.
Psychosomatic disorders (muscular/joint) are local reflec-
tions of anxiety, tension or other emotions in an individual as a
muscular tonus. Anxiety plays an important role in the cogni-
tion, affection and behavior of the patients who have chronic
muscular/joint pains (Asmundson, 1994). Among the re-
searches who have studied the efficiency of cognitive behav-
ioral family therapy in the treatment of psychosomatic muscu-
lar-joint pains, the following examples can be pointed out:
Kendal et al. (1997) treated a group of individuals suffering
from anxiety disorders and muscular pains using a cognitive
behavioral approach. In this research, the cognitive components
of anxiety (such as recognizing physiological symptoms of
anxiety, correcting stressful conversations, compromising dif-
ferent stressful situations and self-monitoring) were applied to
the experimental group during 16 weeks. They were also
trained with some behavioral techniques (like modeling, desen-
sitization, role playing and relaxation) in order to control anxi-
ety. At the end of the treatment period, anxiety symptoms were
significantly reduced in the experimental group as compared
with the control g r o u p .
Kazdin and Weisz (1998) compared individual and family
cognitive behavioral therapy in the reduction of psychosomatic
symptoms. The results for individual and family cognitive be-
havioral therapy were 57.1% and 84% improvement, respec-
tively. Johnson and Dahl (1998) investigated the effects of a
cognitive behavioral pain control program in a group of par-
ticipants with muscular bone pains in two groups: the control
group (study 1) and a sample of patients (study 2) that were
studied during a long period. The four-week therapy programs
included instructional sessions, explaining objectives, nerve
calming, practice of social skills, reduction of the use of medi-
cines and reversion to work programs.
Clinicians have been interested in applying different methods
of psychotherapy including behavior therapy (Kazdin & Wesiz,
1998) and positive family therapy (Peseschkian, 1986) in treat-
ing psychosomatic disorders and also investigating the effi-
ciency of cognitive behavioral techniques in the treatment of
muscular and bone disorders (Johnson & Dahl, 1998). The
main goal of the present research was to study the effect of
cognitive behavioral family therapy on the treatment of psy-
chosomatic disorders (muscular and bone pains).
Method
The present research was a single-subject study using an A-B
design. In order to choose the research sample, 3 individuals (2
male and 1 female) with muscular-bone type of psychosomatic
disorders were chosen from individuals who referred to a pri-
vate psychotherapy clinic. However, since two of these partici-
pants (1 man and 1 woman) did not continue to participate in all
of their therapy sessions, they were eliminated from the original
sample and the sample was eventually consisted of three re-
maining participants.
All of the participants were diagnosed with psychosomatic
disorder like muscular-bone problems (backache-neck pain)
without physiological sources. The diagnosis was confirmed by
X-ray, clinical interview made by psychotherapist based on
DSM-IV-TR, SCL-90-R and MMPI-2 testes. Data collection
was conducted in two stages of pretest (stage A) and posttest
(stage B).
Minnesota Multiphase Personality Inventory (MMPI) has 13
subscales, 3 subscales of which are related to test validity (L, F
and K) and other 10 subscales of Hypochondria (Hs), Depres-
sion (D), Hysteria (Hy), Psychosocial Deviation (Pd), Mascu-
linity-Feminity (MF), Paranoia (P), Psychasthenia (Pt), Sc hizo-
phrenia (Sc), Hypomania (Ma) and Social Introversion (Si) are
related to personality and clinical indexes. The method of an-
swering these questions is true/false; each true answer receives
1 score while the false answer receives 0.
The validity of MMPI has been confirmed. The reliability of
all MMPI subscales was also confirmed in a meta-analysis
study and the range of reliability coefficients was reported be-
tween 0.71 for Ma scale and 0.84 for Pt scale (Marnat, 1990).
In the present research, the short form of MMPI was used
which included 71 questions. The participants’ scores in Hs
scale (or hypochondria) were considered as an index of their
physical problems.
The Symptom Checklist-90-Revised (SCL-90-R) is a diag-
nostic and screening test used mainly for mental patients and
drug addicts and alcoholics (Mirzaei, 1980). It consists of 90
items and 9 dimensions which measure different psychological
aspects including somatization, obsessive-compulsive traits,
interpersonal sensitivity, depression, anxiety, hostility, phobia,
paranoia and psychoticism. By applying Cronbach’s alpha co-
efficient, Mirzaei (1980) reported the reliability of the SCL-
90-R as 0.70 and its concurrent validity with the MMPI-2 was
0.51. According to Hooman (1997), the internal consistency
coefficients of this instrument’s subscales, which ranged from
0.69 to 0.88, were acceptable. The construct validity and con-
current validity of this instrument were also acceptable accord-
ing to Hooman (1997) and Nadjarian and Davoodi (2001). In
the present study, the Cronbach’s alpha coefficient was 0.97 for
the whole test which ranged from 0.74 to 0.87 in the subtests.
The correlation between the two halves of the test was 0.89. In
this research, the participants’ score in the subscale of physical
complaints was considered as the index of their physical prob-
lems.
Procedure
As mentioned before, the research sample included 3 indi-
viduals diagnosed with muscular bone psychosomatic disorder.
Copyright © 2012 SciRes. 1105