Combined Hamartoma of the Optic Disc and Retinal Pigment Epithelium—3 Years of the Follow-Up with
Semi-Automated Kinetic Perimetry
Copyright © 2012 SciRes. OJOph
118
The diagnostics is based on fundoscopy and confirmed
by fluorescein angiography and Ocular Coherence To-
mography (OCT). The presenting syndrome is painless
unilateral silent visual loss. The patients are usually as-
ymptomatic until the late childhood. The anterior seg-
ment is not affected. There are anecdotical reports on
systemic associations with neurofibromatosis type II and
tuberous sclerosis. RPE hamartomas usually show no
growth potential. Hamartoma of the retina and RPE can
generate a large papillary and retinal distortion [3], thu s it
is often accompanied with vascular tortuosity and epire-
tinal membrane. Secondary changes as vitreous hemor-
rhage, Choroidal Neovascular Membrane (CNV) or retinal
detachment [4] on some occasions may cause visual loss.
There have been reports describing pars plana vitrectomy
due to epiretinal membrane following hamartoma [5] or
submacular surgery due to CNV [6].
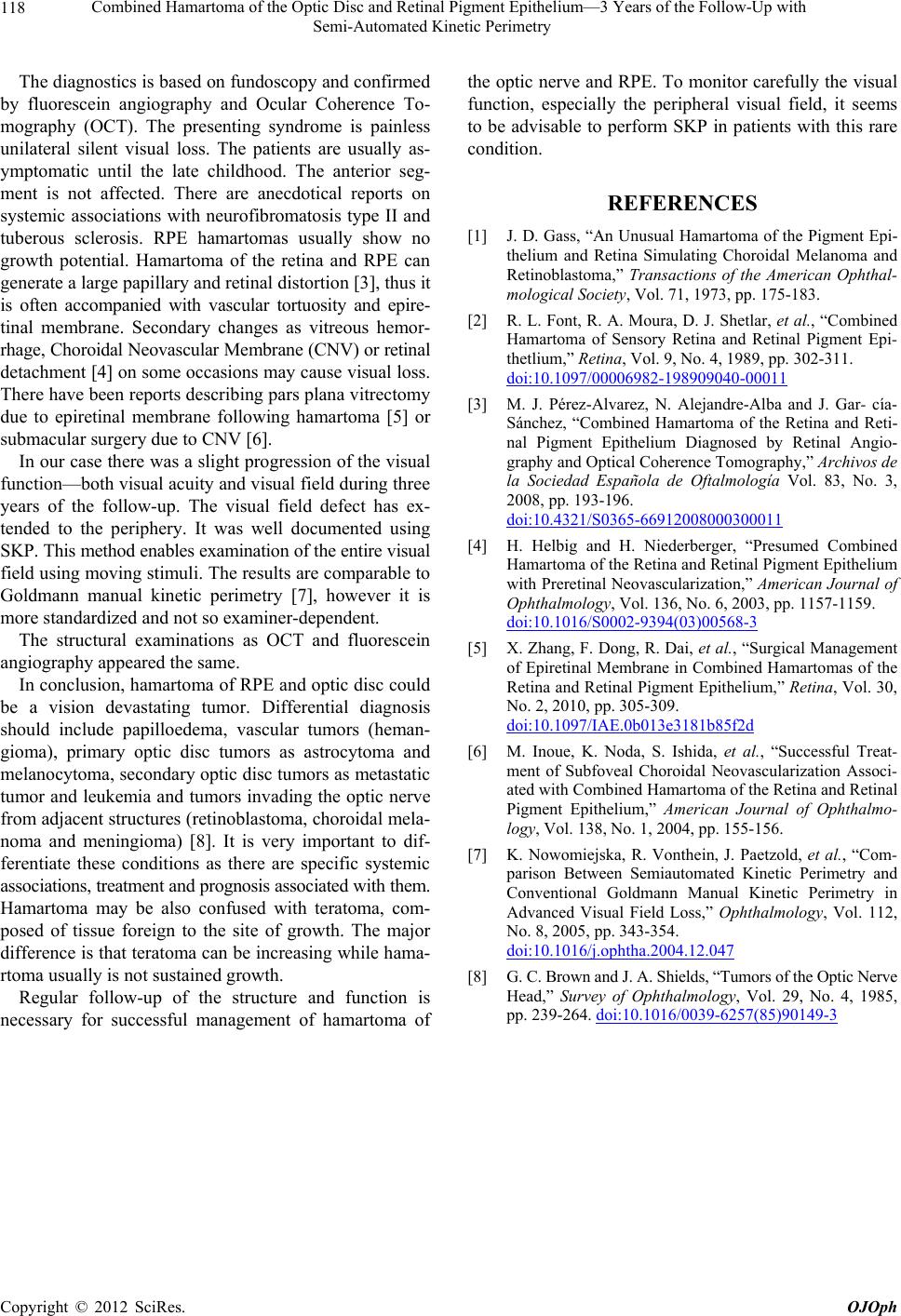
In our case there was a slight progression of the visual
function—both visual acuity and visual field during three
years of the follow-up. The visual field defect has ex-
tended to the periphery. It was well documented using
SKP. This method enables examination of the entire visual
field using moving stimuli. The results are comparable to
Goldmann manual kinetic perimetry [7], however it is
more standardized and not so examiner-dependent.
The structural examinations as OCT and fluorescein
angiography appeared the same.
In conclusion, hamartoma of RPE and optic disc could
be a vision devastating tumor. Differential diagnosis
should include papilloedema, vascular tumors (heman-
gioma), primary optic disc tumors as astrocytoma and
melanocytoma, secondary optic disc tumors as metastatic
tumor and leukemia and tumors invading the optic nerve
from adjacent structures (retinoblastoma, choroidal mela-
noma and meningioma) [8]. It is very important to dif-
ferentiate these conditions as there are specific systemic
associations, treatment and prognosis associated with them.
Hamartoma may be also confused with teratoma, com-
posed of tissue foreign to the site of growth. The major
difference is that teratoma can be increasing while hama-
rtoma usually is not sustained growth.
Regular follow-up of the structure and function is
necessary for successful management of hamartoma of
the optic nerve and RPE. To monitor carefully the visual
function, especially the peripheral visual field, it seems
to be advisable to perform SKP in patients with this rare
condition.
REFERENCES
[1] J. D. Gass, “An Unusual Hamartoma of the Pigment Epi-
thelium and Retina Simulating Choroidal Melanoma and
Retinoblastoma,” Transactions of the American Ophthal-
mological Society, Vol. 71, 1973, pp. 175-183.
[2] R. L. Font, R. A. Moura, D. J. Shetlar, et al., “Combined
Hamartoma of Sensory Retina and Retinal Pigment Epi-
thetlium,” Retina, Vol. 9, No. 4, 1989, pp. 302-311.
doi:10.1097/00006982-198909040-00011
[3] M. J. Pérez-Alvarez, N. Alejandre-Alba and J. Gar- cía-
Sánchez, “Combined Hamartoma of the Retina and Reti-
nal Pigment Epithelium Diagnosed by Retinal Angio-
graphy and Optical Coherence Tomography,” Archivos de
la Sociedad Española de Oftalmología Vol. 83, No. 3,
2008, pp. 193-196.
doi:10.4321/S0365-66912008000300011
[4] H. Helbig and H. Niederberger, “Presumed Combined
Hamartoma of the Retina and Retinal Pigment Epithelium
with Preretinal Neovascularization,” American Journal of
Ophthalmology, Vol. 136, No. 6, 2003, pp. 1157-1159.
doi:10.1016/S0002-9394(03)00568-3
[5] X. Zhang, F. Dong, R. Dai, et al., “Surgical Management
of Epiretinal Membrane in Combined Hamartomas of the
Retina and Retinal Pigment Epithelium,” Retina, Vol. 30,
No. 2, 2010, pp. 305-309.
doi:10.1097/IAE.0b013e3181b85f2d
[6] M. Inoue, K. Noda, S. Ishida, et al., “Successful Treat-
ment of Subfoveal Choroidal Neovascularization Associ-
ated with Combined Hamartoma of the Retina and Retinal
Pigment Epithelium,” American Journal of Ophthalmo-
logy, Vol. 138, No. 1, 2004, pp. 155-156.
[7] K. Nowomiejska, R. Vonthein, J. Paetzold, et al., “Com-
parison Between Semiautomated Kinetic Perimetry and
Conventional Goldmann Manual Kinetic Perimetry in
Advanced Visual Field Loss,” Ophthalmology, Vol. 112,
No. 8, 2005, pp. 343-354.
doi:10.1016/j.ophtha.2004.12.047
[8] G. C. Brown and J. A. Shields, “Tumors of the Optic Nerve
Head,” Survey of Ophthalmology, Vol. 29, No. 4, 1985,
pp. 239-264. doi:10.1016/0039-6257(85)90149-3