A Case of CD34-Negative Superficial Acral Fibromyxoma
Copyright © 2012 SciRes. MPS
79
cicular growth pattern, with myxoid stroma and promi-
nent vascularity [2,4]. It has been reported that the tumor
cells of the SAF are diffusely positiv e for CD34 and may
be focally positive for EMA, CD10, and CD99 [4,5-8].
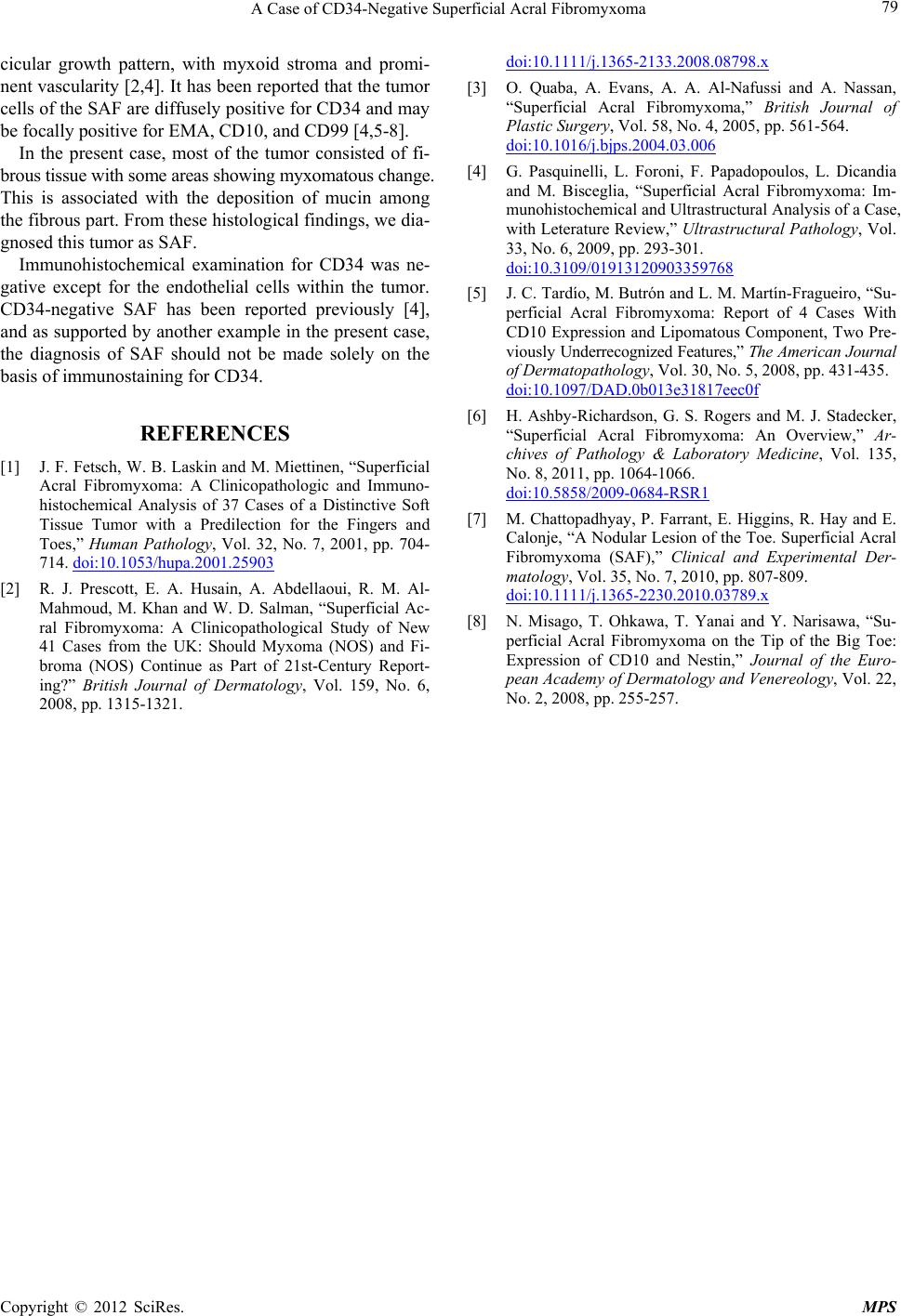
In the present case, most of the tumor consisted of fi-
brous tissue with some areas showing m y xomatous change.
This is associated with the deposition of mucin among
the fibrous part. From these histological findings, we dia-
gnosed this tumor as SAF.
Immunohistochemical examination for CD34 was ne-
gative except for the endothelial cells within the tumor.
CD34-negative SAF has been reported previously [4],
and as supported by another example in the present case,
the diagnosis of SAF should not be made solely on the
basis of immunostaining for CD34.
REFERENCES
[1] J. F. Fetsch, W. B. Laskin and M. Miettinen, “Superficial
Acral Fibromyxoma: A Clinicopathologic and Immuno-
histochemical Analysis of 37 Cases of a Distinctive Soft
Tissue Tumor with a Predilection for the Fingers and
Toes,” Human Pathology, Vol. 32, No. 7, 2001, pp. 704-
714. doi:10.1053/hupa.2001.25903
[2] R. J. Prescott, E. A. Husain, A. Abdellaoui, R. M. Al-
Mahmoud, M. Khan and W. D. Salman, “Superficial Ac-
ral Fibromyxoma: A Clinicopathological Study of New
41 Cases from the UK: Should Myxoma (NOS) and Fi-
broma (NOS) Continue as Part of 21st-Century Report-
ing?” British Journal of Dermatology, Vol. 159, No. 6,
2008, pp. 1315-1321.
doi:10.1111/j.1365-2133.2008.08798.x
[3] O. Quaba, A. Evans, A. A. Al-Nafussi and A. Nassan,
“Superficial Acral Fibromyxoma,” British Journal of
Plastic Surgery, Vol. 58, No. 4, 2005, pp. 561-564.
doi:10.1016/j.bjps.2004.03.006
[4] G. Pasquinelli, L. Foroni, F. Papadopoulos, L. Dicandia
and M. Bisceglia, “Superficial Acral Fibromyxoma: Im-
munohistochemical and Ultrastructural Analysis of a Case,
with Leterature Review,” Ultrastructural Pathology, Vol.
33, No. 6, 2009, pp. 293-301.
doi:10.3109/01913120903359768
[5] J. C. Tardío, M. Butrón and L. M. Martín-Fragueiro, “Su-
perficial Acral Fibromyxoma: Report of 4 Cases With
CD10 Expression and Lipomatous Component, Two Pre-
vio usly Underrecognized Features,” The American Journal
of Dermatopathology, Vol. 30, No. 5, 2008, pp. 431-435.
doi:10.1097/DAD.0b013e31817eec0f
[6] H. Ashby-Richardson, G. S. Rogers and M. J. Stadecker,
“Superficial Acral Fibromyxoma: An Overview,” Ar-
chives of Pathology & Laboratory Medicine, Vol. 135,
No. 8, 2011, pp. 1064-1066.
doi:10.5858/2009-0684-RSR1
[7] M. Chattopadhyay, P. Farrant, E. Higgins, R. Hay and E.
Calonje, “A Nodular Lesion of the Toe. Superficial Acral
Fibromyxoma (SAF),” Clinical and Experimental Der-
matology, Vol. 35, No. 7, 2010, pp. 807-809.
doi:10.1111/j.1365-2230.2010.03789.x
[8] N. Misago, T. Ohkawa, T. Yanai and Y. Narisawa, “Su-
perficial Acral Fibromyxoma on the Tip of the Big Toe:
Expression of CD10 and Nestin,” Journal of the Euro-
pean Academy of Dermatology and Venereology, Vol. 22,
No. 2, 2008, pp. 255-257.