K. OZAWA ET AL.
Copyright © 2012 SciRes. OJNe ph
43
care is significantly correlated with the mental state,
QOL, renal function and symptoms of the patient [18].
Therefore, it is important to improve patients’ satisfac-
tion, psychological adaptation and QOL.
As we showed a strong connection between behavior
of taking medicine and patients’ satisfaction for the di-
alysis care provided by medical staff, more attention
should be placed on the consultation situation of medical
staff when patients have doubts in taking medicine and
questions about their health, for further understanding of
the patient’s relationship with medical staff.
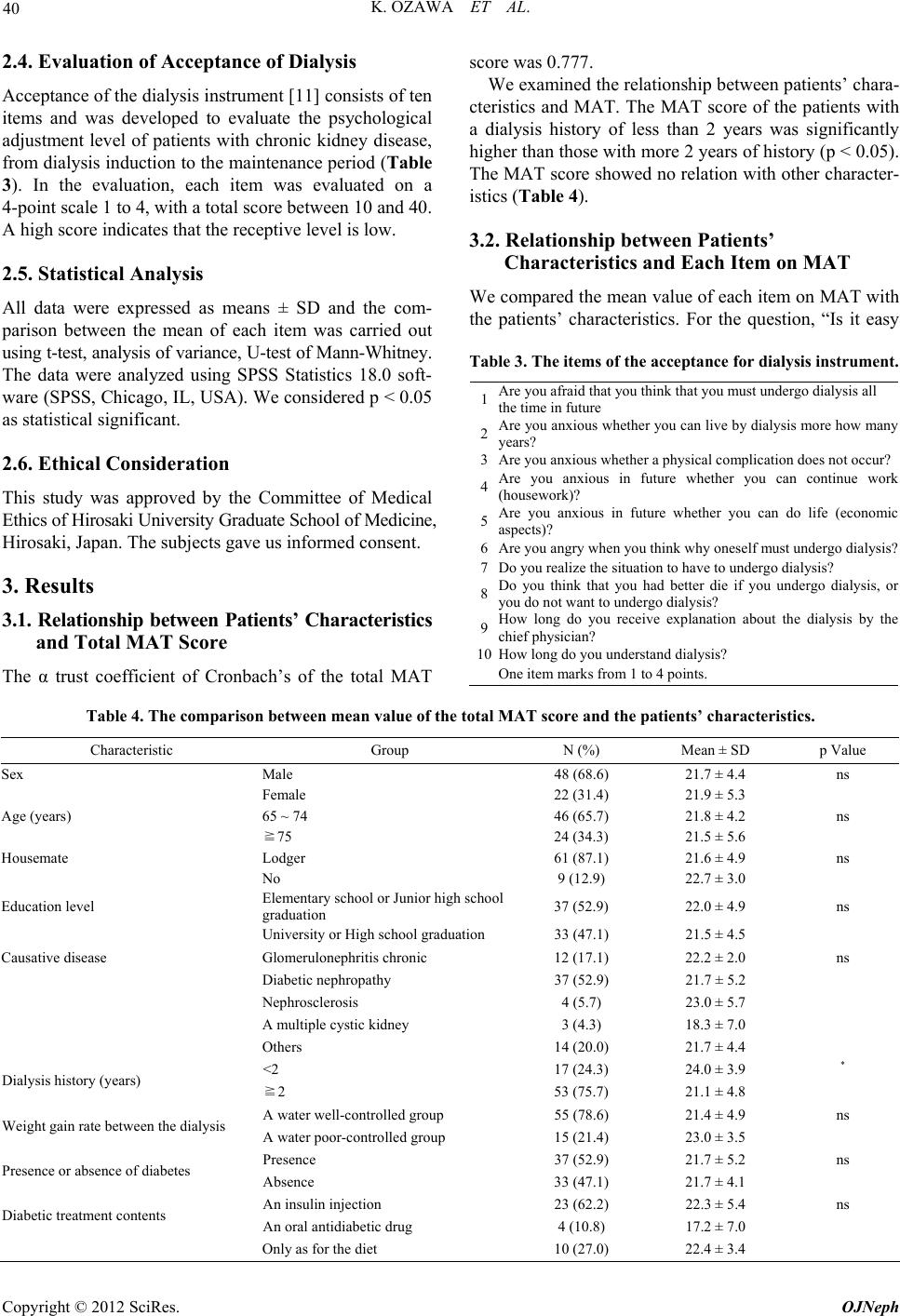
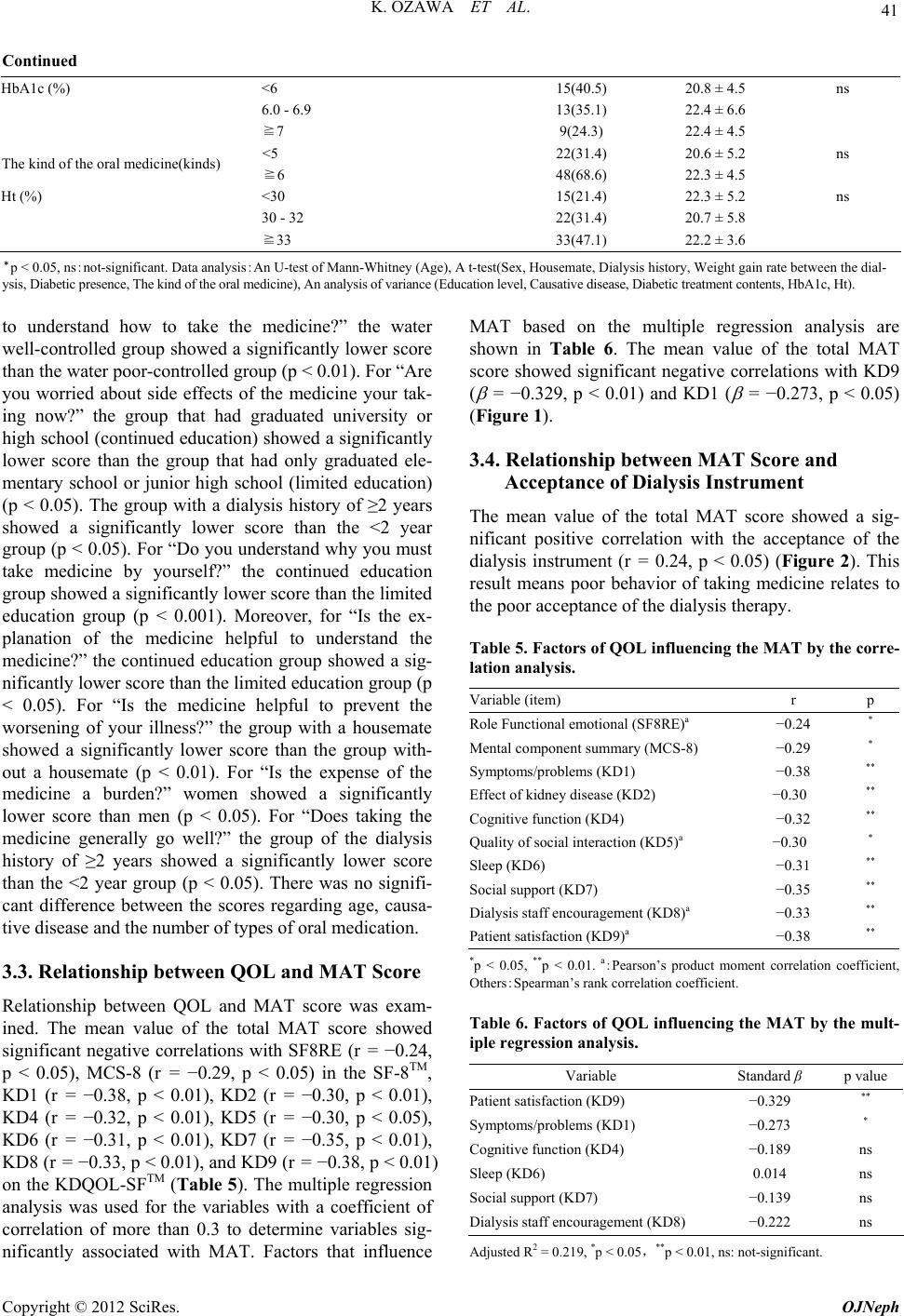
Moreover, the total MAT score showed a significant
positive correlation with acceptance of the dialysis in-
strument. Thus, more acceptable dialysis treatment may
lead to improved adherence. Much effort is still needed
to help patients accept dialysis therapy.
5. Conclusion
Poor behavior of taking medicine is related to a short
dialysis period and the degree of patient satisfaction for
dialysis therapy. It is important to improve patient satis-
faction for dialysis care, increase healthy satisfaction
regarding symptoms, and allow patients to better accept
their disease.
REFERENCES
[1] Japanese Society for Dialysis Therapy, “An Overview of
Regular Dialysis Treatment in Japan as of December 31,
2010,” Tokyo, 2011.
[2] E. A. Graveley and C. S. Oseasohn, “Multiple Drug
Regimens Medication Compliance among Veterans 65
Years and Older,” Resarch in Nursing & Health, Vol. 14,
No. 1, 1991, pp. 51-58. doi:10.1002/nur.4770140108
[3] J. M. Cargill, “Medication Compliance in Elderly People,
Influencing Variables and Interventions,” Journal of Ad-
vanced Nursing, Vol. 17, No. 4, 1992, pp. 422-426.
doi:10.1111/j.1365-2648.1992.tb01925.x
[4] A. W. Deborah, “Evaluation of Medication Interventions
for the Elderly,” Home Healthcare Nurse, Vol. 16, No. 9,
1998, pp. 612-617.
doi:10.1097/00004045-199809000-00008
[5] T. T. Fulmer, P. H. Feldman, T. S. Kim, B. Carty, M.
Beers, M. Molina and M. Putnam, “An Intervention
Study to Enhance Medication Compliance in Commu-
nity-Dwelling Elderly Individuals,” Journal of Gerontol-
ogy Nursing, Vol. 25, No. 8, 1999, pp. 6-13.
[6] A. A. Ryan, “Medication Compliance and Older People:
A Review of the Literature,” International Journal of
Nursing Study, Vol. 36, No. 2, 1999, pp. 153-162.
doi:10.1016/S0020-7489(99)00003-6
[7] J. Petermans, A. S. Suarez and T. V. Hees, “Therapeutic
Adherence in Elderly,” Revue Medical of Liege, Vol. 65,
No. 5-6, 2010, pp. 261-266.
[8] Y. Yuzawa, “Making and the Usefulness of the Medica-
tion Assessment Tool of the Outpatient,” Ochanomizu
Medical Journal, Vol. 50, No. 3, 2002, pp. 133-143.
[9] Y. Miura, J. Green and S. Fukuhara, “Manual of the
KDQOL Japanese Version 1.3,” Institute for Health Out-
comes & Process Evaluation Research, Kyoto, 2004.
[10] S. Fukuhara and Y. Suzukamo, “Manual of the SF-8
Japanese Version,” Institute for Health Outcomes &
Process Evaluation Research, Kyoto, 2004.
[11] I. Fukunishi, “Development of the Measure of the Psy-
chological Acceptance Level of the Dialysis Treatment,”
OFF TIME Chugai Pharmaceutical, Tokyo, 2002, p. 67.
[12] E. Uegima, S. Mikami and H. Morimoto, “Drug Compli-
ance in the Elderly,” Nippon Ronen Igakkai Zasshi, Vol.
29, No. 1, 1992, pp. 855-863.
doi:10.3143/geriatrics.29.855
[13] B. R. Siegal, R. J. Calsyn and R. M. Cuddihee, “The Re-
lationship of Social Support to Psychological Adjustment
in End-Stage Renal Disease Patient,” Journal of Chronic
Disease, Vol. 40, No. 4, 1987, pp. 337-344.
[14] D. Cukor, D. S. Rosenthal, R. M. Jindal, C. D. Brown and
P. L. Kimmel, “Depression Is an Important Contributor to
Low Medication Adherence in Hemodialyzed Patients
and Transplant Recipients,” Kidney International, Vol. 75,
No. 11, 2009, pp. 1223-1229. doi:10.1038/ki.2009.51
[15] M. Lindberg and P. Lindberg, “Overcoming Obstacles for
Adherence to Phosphate Binding Medication in Dialysis
Patients: A Qualitative Study,” Pharmacy World & Sci-
ence, Vol. 30, No. 5, 2008, pp. 571-576.
doi:10.1007/s11096-008-9212-9
[16] C. M. Hughes, “Medication Non-Adherence in the Eld-
erly,” Drugs & Aging, Vol. 21, No. 12, 2004, pp. 793-
811.
[17] R. Horne and J. Weinman, “Patients’ Beliefs about Pre-
scribed Medicines and Their Role in Adherence to
Treatment in Chronic Physical Illness,” Journal of Psy-
chosomatic Research, Vol. 47, No. 6, 1999, pp. 555-567.
[18] C. E. Ferranns, M. J. Powers and C. R. Kasch, “Satisfac-
tion with Health Care of Hemodialysis Patients” Research
of Nursing & Health, Vol. 10, No. 6, 1987, pp. 367-374.