M. Nakada et al. / HEALTH 2 (2010) 713-721
Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journa l/HEALTH/
720
bone mass with a rapid decline of estrogen levels in
postmenopausal females [13]. The OSI is generally higher
in males than females. Average OSI of 20-44 years peo-
ple also in this study showed a significant gender differ-
ence (males: OSI = 3.034 ± 0.396, females: OSI = 2.742
± 0.350, t = 5.283, P = 0.000). The proper criteria has
not been reported for males, so this study conveniently
utilized the adult female criteria creation method devel-
oped by the Japan Osteoporosis Foundation [2]. It is
considered that males’ OSI level is higher and thus the
criteria for the group requiring close examination or
guidance differs between genders. Hence, from now, the
OSI standard for males will need to be hastily created
based on a large amount of data.
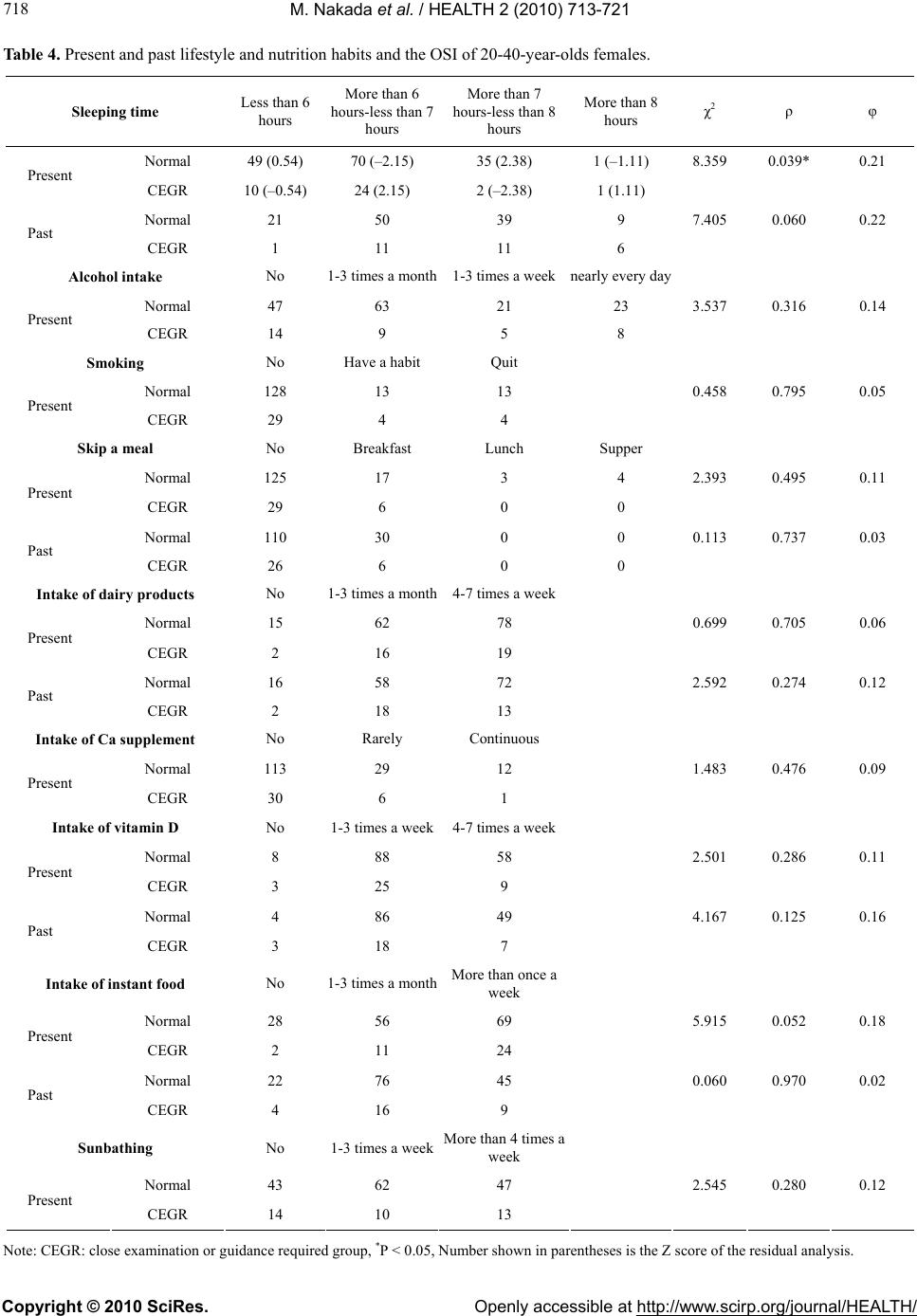
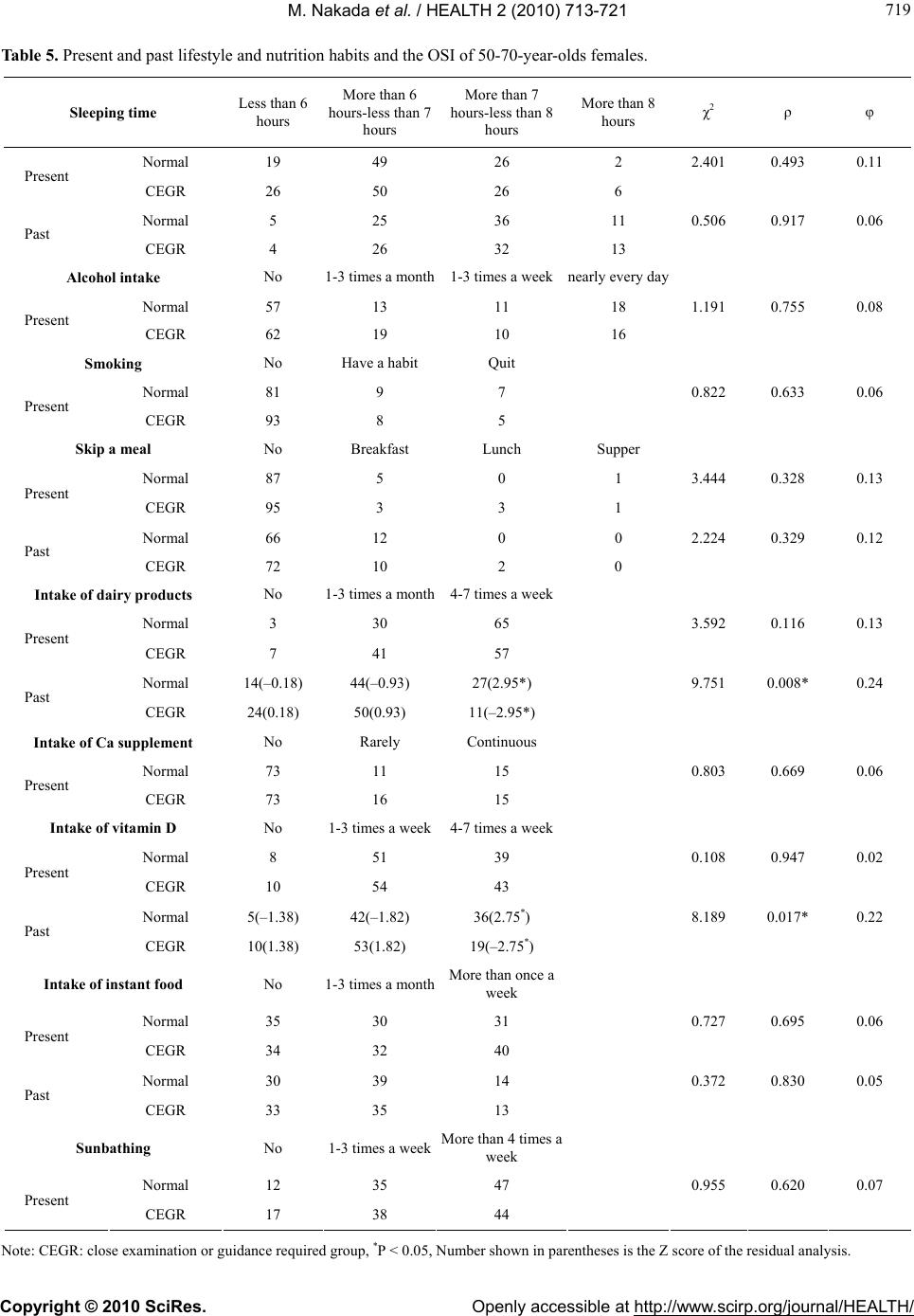
The group requiring close examination or guidance in
50-70 year-old females had a lower proportion of sub-
jects with weekly intake (4-7 times a week) of dairy
products and vitamin D (fish, chicken egg, fungi) in the
past than the normal group. Tomita et al. [7] reported
that, in the study of junior college dietetics students, the
intake of milk, dairy products, and vegetables on a rou-
tine basis is useful to increase bone mass. Nakata et al.
[6] reported that calcaneal OSI in women’s junior col-
lege students was higher in the high milk intake group.
The three year longitudinal study by Dawson-Hughes et
al. [14] found that the proper intake of vitamin D in ad-
dition to calcium intake reduces the decline of BMD. It
was reported also that inadequate metabolism of vitamin
D decreases calcium absorption in both osteoporotics
and elderly subjects [15]. From the present results, it is
considered that the 50-70 year-old females belonging to
the group requiring close examination or guidance were
deficient in calcium intake through dairy products and
intake of vitamin D which is very important for the ab-
sorption of calcium during puberty to increase bone
mass with skeletal growth. In addition, the above sug-
gests that it is important to have adequate calcium and
vitamin D intake in puberty in addition to old age.
Meanwhile, males showed an insignificant relation-
ship between OSI and items involving the present and
past lifestyle and nutrition habits. Because they do not
have a large physiological change as females when they
experience menopause in middle age, the effect of the
intake of calcium and vitamin D during puberty on
maintenance of BMD and bone formation may be lower
than in females. Many bone fractures that occur in eld-
erly people are of the femoral neck and this fracture
causes bedriddenness and disturbances of gait. Therefore
preventing the cause, osteoporosis, is very important
[2,5].
From now, it will be necessary to compare bone min-
eral density between young adults and the elderly longi-
tudinally, and to examine the combined effect of the past
and present lifestyle and exercise habits on BMD.
In summary, the OSI is higher in males than females
and it is higher in 20 year-olds than 30-70 year-olds in
males and is higher in 20-40 year-olds than 50-70 year-
olds in females. The proportion of the group requiring
close examination or guidance is high in 50-70 year-olds,
particularly in females with a rapid increase after their
50s. The 50-70 year-old females in the group requiring
close examination or guidance were deficient in calcium
intake through dairy products in addition to the intake of
vitamin D, which is important for the absorption of cal-
cium during puberty when bone mass increases with
skeletal growth. The intake of calcium and vitamin D
during puberty may be very important to prevent the
decrease of bone mineral density in old age.
REFERENCES
[1] Gushiken, M. and Akisaka, M. (2004) A survey of cal-
caneus bone mineral density related to physique in young
females and comparison of the findings to those of eld-
erly females in Okinawa. The Journal of Education and
Health Science, 49(4), 239-247.
[2] Japan Osteoporosis Foundation (2000) This handbook for
preventing osteoporosis is based on the Health and
Medical Service Act for the Aged. Japan Medical Jour-
nal, 2nd Edition, Tokyo, 1-135.
[3] Kim, H., Tanaka, K., Nakanishi, T. and Amagai, H. (1999)
Effects of age and body composition on rate of bone
mineral density loss in Japanese adult women. Japanese
Journal of Physical Fitness and Sports Medicine, 48(1),
81-90.
[4] Yokouchi, J., Ando, D., Ono, Y., Ozaki, Y., Asakawa, K.,
Kitagawa, J., Nakahara, Y. and Koyama, K. (2003) The
relationship between calcaneal quantitative ultrasound
parameters and anthropometric measures in university
women. Japanese Journal of Physical Fitness and Sports
Medicine, 52(5), 639-646.
[5] Naka, T., Nakajima, D., Oh, T.W., Han, I., Sakurai, T. and
Igawa, S. (2004) Effects of lifestyle on bone metabolism
in middle-aged and aged Japanese women. Japanese
Journal of Physiological Anthropology, 9(3), 85-92.
[6] Nakata, H., Okazaki, N., Yagita, K., Ohtsuki, S., Satoh, H.
and Mimura, K. (2003) The relationship between ultra-
sound calcaneal bone mass, physique, and daily habits in
women’s junior college students. The Journal of Educa-
tion and Health Science, 49(52), 155-162.
[7] Tomita, N. and Akisaka, M. (2007) A study on the rela-
tionship between bone mineral density and dietary habits
and regular exercise activity of junior college dietetics
students. The Journal of Education and Health Science,
52(4), 212-224.
[8] Kim, H., Tanaka, K., Amagai, H. and Suzuki, T. (1999)
Age-related changes of body composition by dual-energy
X-ray absorptiometry in Japanese men and women. Ja-
pan Journal of Physical Education, 44(6), 500-509.
[9] Dawson-Hughes, B. (1996) Calcium and vitamin D nu-
tritional needs of elderly women. The Journal of Nutri-