Driving Skills in HIV-Infected Patients Well Controlled with Antiretroviral Therapy
124
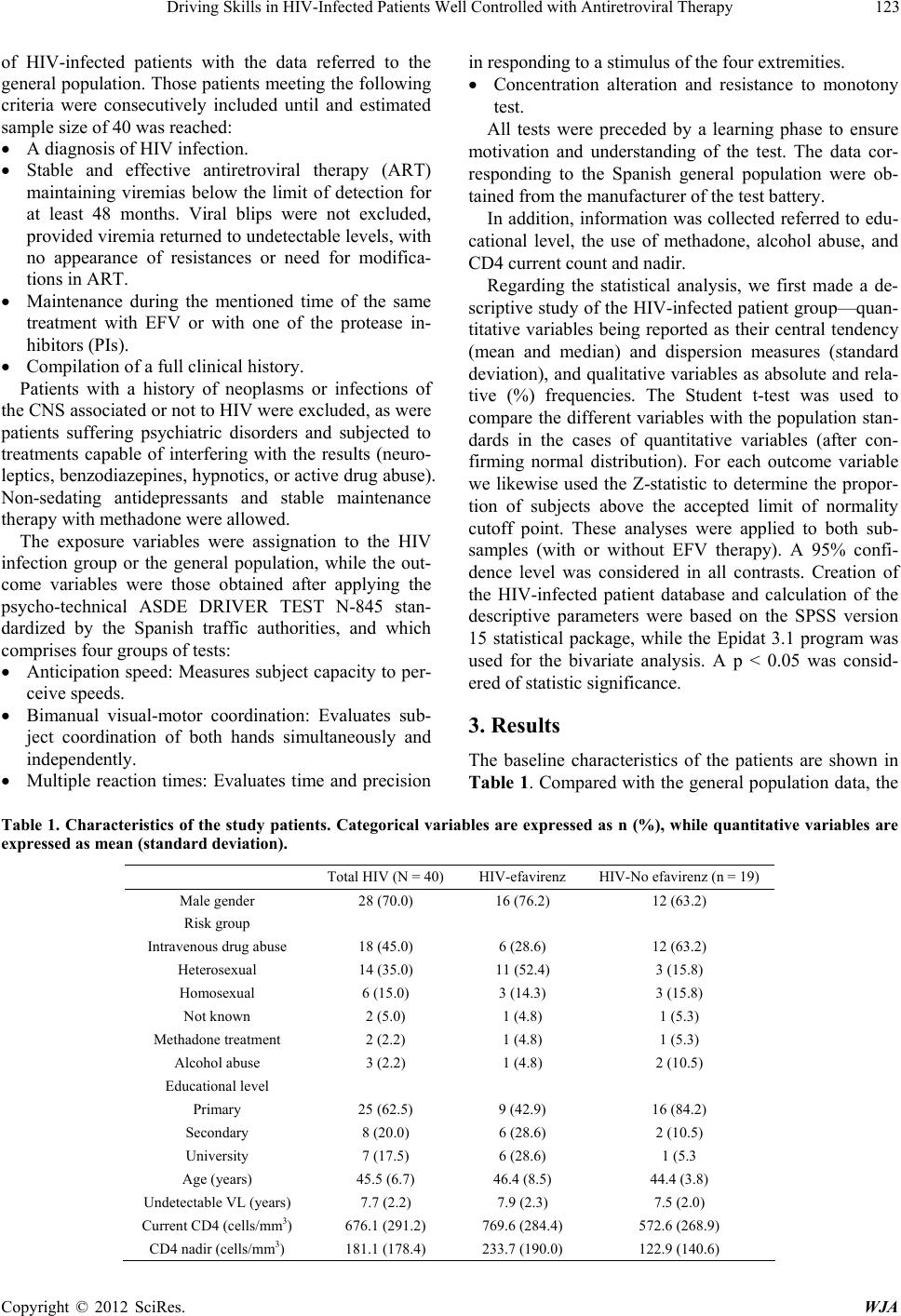
scores in the HIV-infected patient group were signifi-
cantly poorer in one of th e anticipation speed tests (mean
deviation time (p = 0.03)) and in one of the multiple re-
action tests (mean reaction time (p = 0.05)). In contrast,
in relation to bimanual visual-motor coordination, the
HIV-infected patients obtained better results in all three
tests (p < 0.01). There were no differences in the per-
centages of patients with scores below the recommended
limits versus the general population, in any of the tests.
On comparing the treatment subgroups (EFV versus PI),
no differences were recorded in any of the study vari-
ables, and the differences with respect to the general
population were the same as those described for the glo-
bal group.
4. Comments
Driving is a complex activity requ iring the integration of
perception, attention and motor response. The ASDE
DRIVER TEST N-845 [8] is a test battery with equip-
ment homologated by the Spanish traffic authorities, de-
signed to assess psychological and physical aptitude for
obtaining the driving license in Spain. The battery in-
cludes tests relating to anticipation speed, bimanual vis-
ual-motor coordination, multiple reaction times, concen-
trated attention, and resistance to monotony. Aptitude is
declared by the examiner after the global evaluation,
though it is considered that the results should exceed
percentile 10 in the reference tables. The ASDE DRI-
VER TEST N-845 has also been used to assess driving
aptitude in other scenarios such as dementias [9] and
residents after the duty shift [10].
The great interest in neurocognitive disorders among
well controlled HIV-infected patients is not without con-
troversy [11,12]. The results of our study support the
existence of small differences in driving skill between
these patients and the general population—with poorer
results in some of the tests referred to anticipation speed
and reaction time, but with better performance in biman-
ual coordination. Given the different age distribution
with respect to the reference tables of the general popula-
tion (data not shown), poorer performance could have
greater importance. In contrast, th e good results obtained
in terms of bimanual coordination among the HIV-in-
fected patients possibly could be attributed in part to
widespread playing of videogames, which exercises
skills of this kind.
On the other hand, EFV is well known to induce CNS
alterations in the first weeks of treatment [13]. The ef-
fects over the long term are less clear, and in the present
study we found no differences in test performance among
the patients administered EFV versus those treated with
PIs. Assignment to treatment based on supervising phy-
sician criterion could interfere with interpretation of
these results, and factors such as a lower CD4 nadir
among the patients treated with PIs theoretically would
favor greater neurocognitive alterations in this group—a
situation no observed in our study, however.
The strength of our study is that it involves a highly
selected group of patients with few comorbidities, and
who have received stable ART for long periods of time.
In contrast, a limitation of the study is the fact that treat-
ment assignment was based on physician criterion; as a
result, there were baseline differences in relation to CD4
nadir and current count.
5. Conclusion
Assuming the limitations inherent to non-randomized,
cross-sectional studies, we observed minor differences in
test performance among the HIV-infected patients versus
the data contained in the normality tables. These dif-
ferences are of arguable clinical significance, and no dif-
ferences were found in driving skills b etween th e pa tien ts
administered EFV and those receiving PI treatment on a
chronic basis. Further studies are needed to evaluate the
effects of EFV in the first weeks of treatment.
REFERENCES
[1] D. B. Clifford, S. Evans, Y. Yang, E. P. Acosta, K.
Goodkin and K. Tashima, “Impact of Efavirenz on Neu-
ropsychological Performance and Symptoms in HIV
Infected Individuals,” Annals of Internal Medicine, Vol.
143, No. 10, 2005, pp. 714-721.
[2] T. Hawkins, C. Geist, B. Young, A. Giblin, R. C. Mercier,
K. Thornton, et al., “Comparison of Neuropsychiatric
Side Effects in an Observational Cohort of Efavirenz- and
Protease Inhibitor-Treated Patients,” HIV Clinical Trials,
Vol. 6, 2005, pp. 187-196.
doi:10.1310/92VR-FP24-J8GA-B49Q
[3] C. R. Fumaz, J. A. Munoz-Moreno, J. Moltó, E. Negredo,
M. J. Ferrer, G. Sirera, et al., “Long-Term Neuro-
psychiatric Disorders on Efavirenz-Based Approaches:
Quality of Life, Psychologic Issues, and Adherence,”
Journal of Acquired Immune Deficiency Syndromes, Vol.
38, No. 5, 2005, pp. 560-565.
doi:10.1097/01.qai.0000147523.41993.47
[4] R. K. Heaton, D. B. Clifford, D. R. Franklin Jr., S. P.
Woods, C. Ake, et al., “HIV-Associated Neurocognitive
Disorders Persist in the Era of Potent Antiretroviral
Therapy CHARTER Study,” Neurology, Vol. 75, No. 23,
2010, pp. 2087-2096.
doi:10.1212/WNL.0b013e318200d727
[5] S. Simioni, M. Cavassini, J. M. Annoni, A. R. Abraham, I.
Bourquin, V. Schiffer, A. Calmy, J. P. Chave, E. Gia-
cobini, B. Hirschel and R. A. Du Pasquier, “Cognitive
Dysfunction in HIV Patients Despite Long-Standing
Suppression of Viremia,” AIDS, Vol. 24, No. 9, 2010, pp.
1243-1250.
[6] T. D. Marcotte, T. Wolfson, T. J. Rosenthal, R. K. Heaton,
Copyright © 2012 SciRes. WJA