A Clinico-Pathological Study of Poly Morphous Light Eruption
222
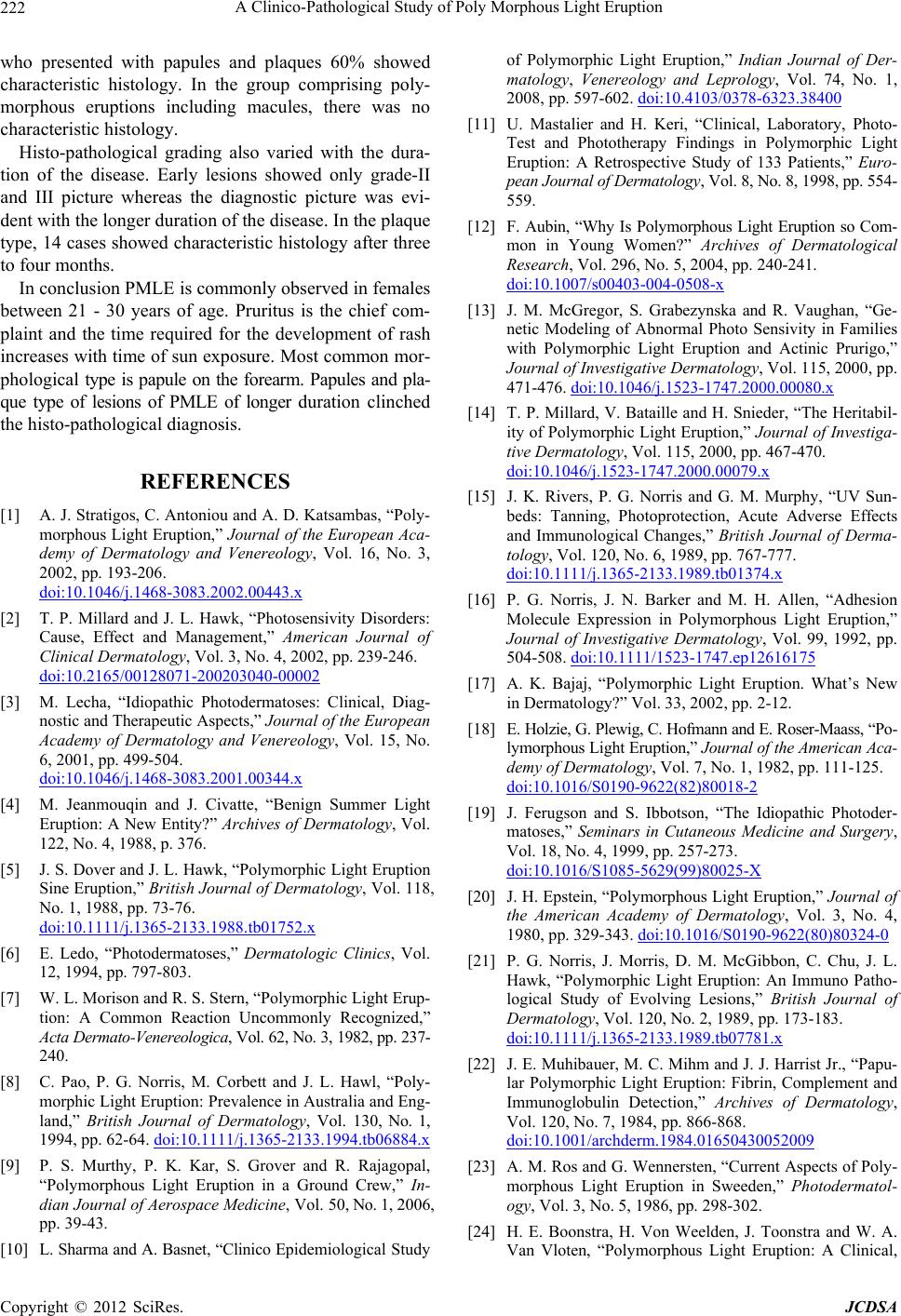
who presented with papules and plaques 60% showed
characteristic histology. In the group comprising poly-
morphous eruptions including macules, there was no
characteristic histology.
Histo-pathological grading also varied with the dura-
tion of the disease. Early lesions showed only grade-II
and III picture whereas the diagnostic picture was evi-
dent with the longer duration of the disease. In the plaque
type, 14 cases showed characteristic histology after three
to four months.
In conclusion PMLE is commonly observed in females
between 21 - 30 years of age. Pruritus is the chief com-
plaint and the time required for the development of rash
increases with time of sun exposure. Most common mor-
phological type is papule on the forearm. Papules and pla-
que type of lesions of PMLE of longer duration clinched
the histo-pathological diagnosis.
REFERENCES
[1] A. J. Stratigos, C. Antoniou and A. D. Katsambas, “Poly-
morphous Light Eruption,” Journal of the European Aca-
demy of Dermatology and Venereology, Vol. 16, No. 3,
2002, pp. 193-206.
doi:10.1046/j.1468-3083.2002.00443.x
[2] T. P. Millard and J. L. Hawk, “Photosensivity Disorders:
Cause, Effect and Management,” American Journal of
Clinical Dermatology, Vol. 3, No. 4, 2002, pp. 239-246.
doi:10.2165/00128071-200203040-00002
[3] M. Lecha, “Idiopathic Photodermatoses: Clinical, Diag-
nostic and Therapeutic Aspects,” Journal of the European
Academy of Dermatology and Venereology, Vol. 15, No.
6, 2001, pp. 499-504.
doi:10.1046/j.1468-3083.2001.00344.x
[4] M. Jeanmouqin and J. Civatte, “Benign Summer Light
Eruption: A New Entity?” Archives of Dermatology, Vol.
122, No. 4, 1988, p. 376.
[5] J. S. Dover and J. L. Hawk, “Polymorphic Light Eruption
Sine Eruption,” British Journal of Dermatology, Vol. 118,
No. 1, 1988, pp. 73-76.
doi:10.1111/j.1365-2133.1988.tb01752.x
[6] E. Ledo, “Photodermatoses,” Dermatologic Clinics, Vol.
12, 1994, pp. 797-803.
[7] W. L. Morison and R. S. Stern, “Polymorphic Light Erup-
tion: A Common Reaction Uncommonly Recognized,”
Acta Dermato-Venereologica, Vol. 62, No. 3, 1982, pp. 237-
240.
[8] C. Pao, P. G. Norris, M. Corbett and J. L. Hawl, “Poly-
morphic Light Eruption: Prevalence in Australia and Eng-
land,” British Journal of Dermatology, Vol. 130, No. 1,
1994, pp. 62-64. doi:10.1111/j.1365-2133.1994.tb06884.x
[9] P. S. Murthy, P. K. Kar, S. Grover and R. Rajagopal,
“Polymorphous Light Eruption in a Ground Crew,” In-
dian Journal of Aerospace Medicine, Vol. 50, No. 1, 2006,
pp. 39-43.
[10] L. Sharma and A. Basnet, “Clinico Epidemiological Study
of Polymorphic Light Eruption,” Indian Journal of Der-
matology, Venereology and Leprology, Vol. 74, No. 1,
2008, pp. 597-602. doi:10.4103/0378-6323.38400
[11] U. Mastalier and H. Keri, “Clinical, Laboratory, Photo-
Test and Phototherapy Findings in Polymorphic Light
Eruption: A Retrospective Study of 133 Patients,” Euro-
pean Journal of Dermatology, Vol. 8, No. 8, 1998, pp. 554-
559.
[12] F. Aubin, “Why Is Polymorphous Light Eruption so Com-
mon in Young Women?” Archives of Dermatological
Research, Vol. 296, No. 5, 2004, pp. 240-241.
doi:10.1007/s00403-004-0508-x
[13] J. M. McGregor, S. Grabezynska and R. Vaughan, “Ge-
netic Modeling of Abnormal Photo Sensivity in Families
with Polymorphic Light Eruption and Actinic Prurigo,”
Journal of Investigative Dermatology, Vol. 115, 2000, pp.
471-476. doi:10.1046/j.1523-1747.2000.00080.x
[14] T. P. Millard, V. Bataille and H. Snieder, “The Heritabil-
ity of Polymorphic Light Eruption,” Journal of Investiga-
tive Dermatology, Vol. 115, 2000, pp. 467-470.
doi:10.1046/j.1523-1747.2000.00079.x
[15] J. K. Rivers, P. G. Norris and G. M. Murphy, “UV Sun-
beds: Tanning, Photoprotection, Acute Adverse Effects
and Immunological Changes,” British Journal of Derma-
tology, Vol. 120, No. 6, 1989, pp. 767-777.
doi:10.1111/j.1365-2133.1989.tb01374.x
[16] P. G. Norris, J. N. Barker and M. H. Allen, “Adhesion
Molecule Expression in Polymorphous Light Eruption,”
Journal of Investigative Dermatology, Vol. 99, 1992, pp.
504-508. doi:10.1111/1523-1747.ep12616175
[17] A. K. Bajaj, “Polymorphic Light Eruption. What’s New
in Dermatology?” Vol. 33, 2002, pp. 2-12.
[18] E. Holzie, G. Plewig, C. Hofmann and E. Roser-Maass, “Po-
lymorphous Light Eruption,” Journal of the American Aca-
demy of Dermatology, Vol. 7, No. 1, 1982, pp. 111-125.
doi:10.1016/S0190-9622(82)80018-2
[19] J. Ferugson and S. Ibbotson, “The Idiopathic Photoder-
matoses,” Seminars in Cutaneous Medicine and Surgery,
Vol. 18, No. 4, 1999, pp. 257-273.
doi:10.1016/S1085-5629(99)80025-X
[20] J. H. Epstein, “Polymorphous Light Eruption,” Journal of
the American Academy of Dermatology, Vol. 3, No. 4,
1980, pp. 329-343. doi:10.1016/S0190-9622(80)80324-0
[21] P. G. Norris, J. Morris, D. M. McGibbon, C. Chu, J. L.
Hawk, “Polymorphic Light Eruption: An Immuno Patho-
logical Study of Evolving Lesions,” British Journal of
Dermatology, Vol. 120, No. 2, 1989, pp. 173-183.
doi:10.1111/j.1365-2133.1989.tb07781.x
[22] J. E. Muhibauer, M. C. Mihm and J. J. Harrist Jr., “Papu-
lar Polymorphic Light Eruption: Fibrin, Complement and
Immunoglobulin Detection,” Archives of Dermatology,
Vol. 120, No. 7, 1984, pp. 866-868.
doi:10.1001/archderm.1984.01650430052009
[23] A. M. Ros and G. Wennersten, “Current Aspects of Poly-
morphous Light Eruption in Sweeden,” Photodermatol-
ogy, Vol. 3, No. 5, 1986, pp. 298-302.
[24] H. E. Boonstra, H. Von Weelden, J. Toonstra and W. A.
Van Vloten, “Polymorphous Light Eruption: A Clinical,
Copyright © 2012 SciRes. JCDSA