I. S. C. Jones, A. Jones / Open Journal of Obstetrics and Gynecology 2 (2012) 210-212
212
pruritus vulvae for example candidiasis, lichen planus
and HPV infection. Most VDs occur in post menopausal
women but can occur in the child and during reproduc-
tive years. Even pregnant women with their high levels
of female hormones can present with VDs suggesting
that theories to explain the basis of these conditions can
not be solely due to a lack of female hormones.
The study found an association between autoimmune
thyroid disease and LS of 10%, which is in line with
other reports. There are reports of LS having a hereditary
basis with mothers and sisters of sufferers being reported
however this was not recognised in the current study. The
associations between VDs and diabetes, other skin dis-
orders (psoriasis, vitiligo and lichen planus), drug aller-
gies and non genital cancers did not reach statistical sig-
nificance. Depression requiring treatment was present in
14% of LS patients, 29% of LSC and 20% of MD. No
significant difference was found between these three
groups using z scores (LS v LSC z = 1.822; LS v MD z =
0.338; LSC v MD z = 0.44). The benefits of anti depres-
sants include their ability to modify pain.
Of available treatments, most were based on the use of
potent glucocorticoid steroid creams, although once sym-
ptoms settled the weekly or bi-weekly use of 1% hydro-
cortisone proved effective. The concern with long-term
use of steroid creams is the atrophying effect this has on
vulval skin, especially that affected by LS. Another pro-
blem with the use of steroid creams is the development
of fungal infection, which is frequently worse in the
presence of obesity and diabetes. Steroid creams can also
be used in conjunction with vaginal oestrogen cream
when vaginal atrophy causes coital difficulties. Steroid
cream was a popular and effective treatment for LSC,
findings which are in agreement with a series of 976 pa-
tients reported by Ayhan et al. [6].
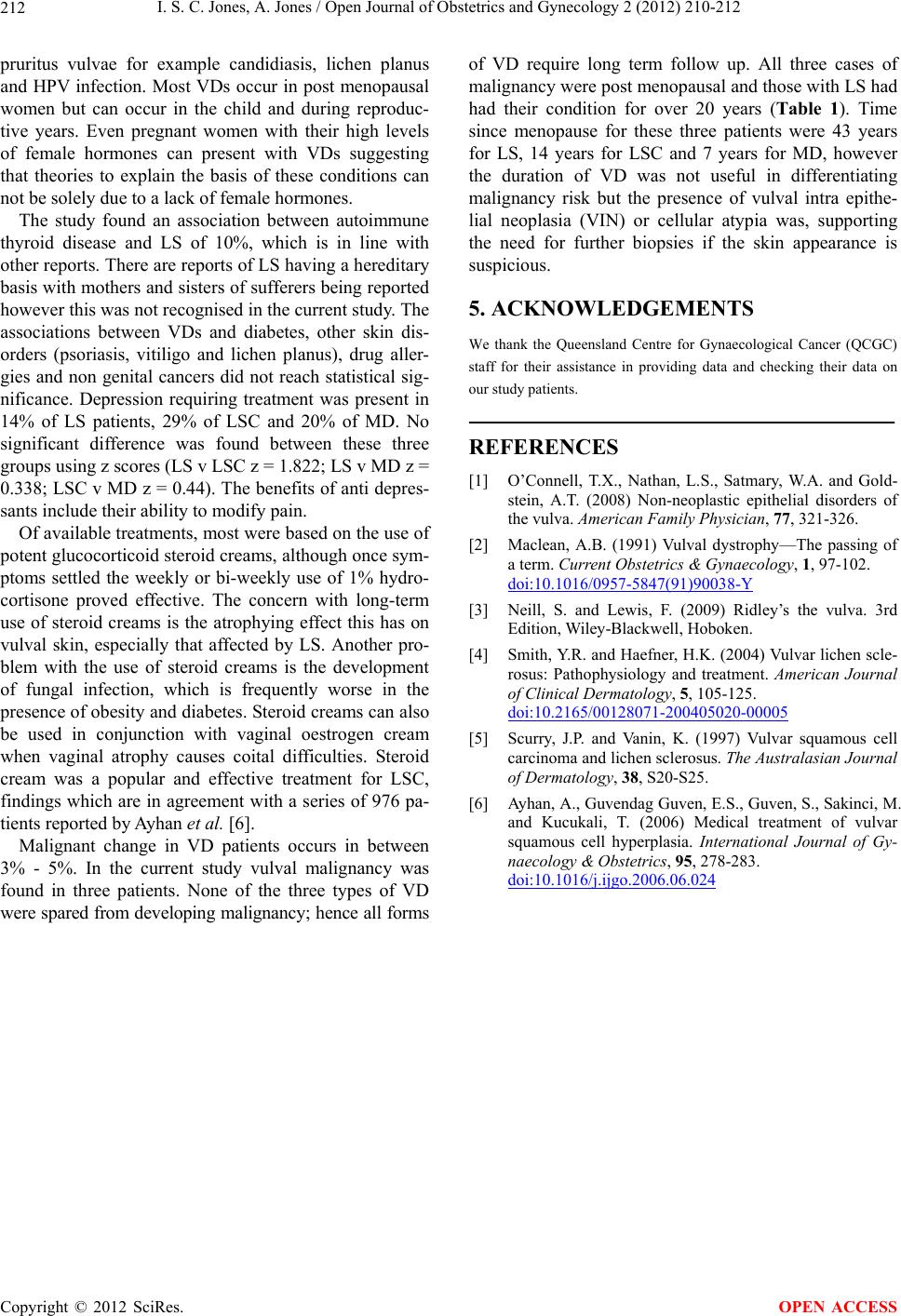
Malignant change in VD patients occurs in between
3% - 5%. In the current study vulval malignancy was
found in three patients. None of the three types of VD
were spared from developing malignancy; hence all forms
of VD require long term follow up. All three cases of
malignancy were post menopausal and those with LS had
had their condition for over 20 years (Table 1). Time
since menopause for these three patients were 43 years
for LS, 14 years for LSC and 7 years for MD, however
the duration of VD was not useful in differentiating
malignancy risk but the presence of vulval intra epithe-
lial neoplasia (VIN) or cellular atypia was, supporting
the need for further biopsies if the skin appearance is
suspicious.
5. ACKNOWLEDGEMENTS
We thank the Queensland Centre for Gynaecological Cancer (QCGC)
staff for their assistance in providing data and checking their data on
our study patients.
REFERENCES
[1] O’Connell, T.X., Nathan, L.S., Satmary, W.A. and Gold-
stein, A.T. (2008) Non-neoplastic epithelial disorders of
the vulva. American Family Physician, 77, 321-326.
[2] Maclean, A.B. (1991) Vulval dystrophy—The passing of
a term. Current Obstetrics & Gynaecology, 1, 97-102.
doi:10.1016/0957-5847(91)90038-Y
[3] Neill, S. and Lewis, F. (2009) Ridley’s the vulva. 3rd
Edition, Wi ley- Blackwe ll, Hoboken.
[4] Smith, Y.R. and Haefner, H.K. (2004) Vulvar lichen scle-
rosus: Pathophysiology and treatment. American Journal
of Clinical Dermatology, 5, 105-125.
doi:10.2165/00128071-200405020-00005
[5] Scurry, J.P. and Vanin, K. (1997) Vulvar squamous cell
carcinoma and lichen sclerosus. The Australasian Journal
of Dermatology, 38, S20-S25.
[6] Ayhan, A., Guvendag Guven, E.S., Guven, S. , Sakinci, M.
and Kucukali, T. (2006) Medical treatment of vulvar
squamous cell hyperplasia. International Journal of Gy-
naecology & Obstetrics, 95, 278-283.
doi:10.1016/j.ijgo.2006.06.024
Copyright © 2012 SciRes. OPEN ACCESS