M. R. Andersen et al. / Open Journal of Obstetrics and Gynecology 2 (2012) 183-191
Copyright © 2012 SciRes.
188
OPEN ACCESS
women with Acid reflux disease were index positive, in a
larger population these differences might have achieved
statistical significance.
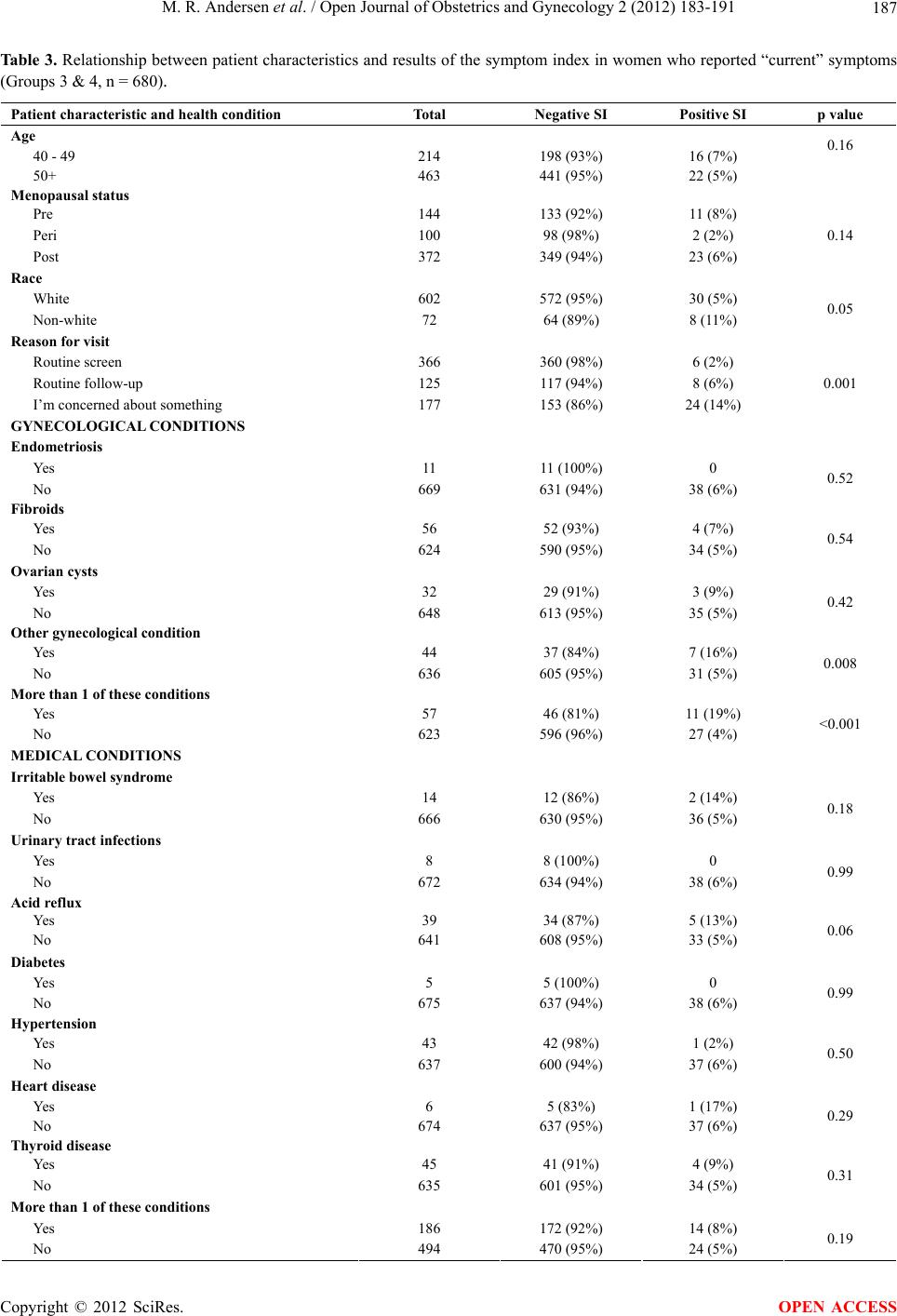
None of the individual gynecological conditions named
on our survey were associated with an elevated fre-
quency positive SI results. However, women reporting
any of a variety of “other” gynecological conditions (16%
versus 5%; p < 0.01) and those with more than one gy-
necologic condition were more likely to have a positive
results (19% versus 4%; p < 0.01).
3.5. Multivariate Analyses
Multivariate analyses were then conducted on an ad-hoc
basis in order to explore whether the statistically signifi-
cant bivariate association of race and symptoms might be
related to differences in personal characteristics or health
status. When a multivariate logistic regression model of
SI positivity that included race, age, more than one gy-
necological condition, fibroids, and IBS was tested, the
association of race with positive results for symptoms
was reduced in size and was not statistically significant.
Differences in the rate of SI positivity associated with
race may be due to other characteristics of our sample.
3.6. Acceptability to Providers
A survey of the physicians, physician assistants (PAs),
and nurses working in the clinic (n = 10) revealed that
they felt the SI was “very acceptable” (5.0, sd = 0 among
physicians and PAs, and 4.5, sd = 0.58 among nurses).
This represented the answers on a Likert scale running
from 1 to 5, where 1 was “not at all acceptable” and 5 =
“very acceptable”. These clinic staff also felt the SI
added 1 - 2 minutes to the patient visit, in the 10% to
20% of patients for whom they judged it added any time
at all. They also indicated that the symptom information
provided was useful to them in their practice (4.3, sd =
0.82 for physicians and PAs and 4.3, sd = 0.58 among
nurses). This on a Likert scale running from 1 to 5 where
1 was “not at all useful” and 5 = “very useful”.
Participating patients were also linked to the Western
Washington SEER registry to determine if they had de-
veloped any cancer in the 12 months following study
participation. One new case of ovarian cancer was iden-
tified. The participant had a positive SI and was diag-
nosed with ovarian cancer shortly after participating. In
this sample no other participants with a positive SI de-
veloped ovarian cancer and no patients with a negative
SI developed ovarian cancer in this sample.
4. CONCLUSIONS
Recently, many lay media outlets have encouraged
women to keep diaries of symptoms as a possible method
of early detection for ovarian cancer. In the Diagnosing
Ovarian Cancer Early (DOvE) study conducted in Can-
ada, women were recruited though a public media cam-
paign utilizing newspaper, radio, television, and fliers to
attract symptomatic women to participate. Remarkably,
through this approach, investigators diagnosed ovarian
cancer in one per 132 women, which is ten times higher
than reported in other studies. Comparison of DOvE pa-
tients to those in the general population found a complete
resection rate of cancer to be 73% compared to 44%, p =
0.075. While this was not statistically significant in this
pilot study, the trend was encouraging and suggests that a
valid tool to assess symptoms associated with ovarian
cancer could be important.
When symptoms are collected prospectively in a clinic
setting using the SI, it appears that 5.5% of women re-
port current symptoms associated with a positive result,
although as many as 9.7% of women may report having
had these symptoms frequently in the past. Thus, it is
important to direct women to report only symptoms they
are currently experiencing frequently. Predictors of
symptoms appear to include the nature of the clinic visit
with women reporting current concerns more likely than
those visiting for a routine screening appointment to re-
port symptoms. Women with a personal history of gyne-
cological conditions, particularly those with more than
one gynecological condition, are also more likely to re-
port currently experiencing symptoms. Those with a di-
agnosis of acid reflux disease or IBS may also be more
likely to report symptoms, although this study did not
have power to fully assess this. Further studies are
needed to better understand racial or ethnic differences in
the reporting of symptoms associated with ovarian can-
cer.
Study Limitations and Considerations
As expected the low incidence of ovarian cancer led to
only one patient in the population developing ovarian
cancer. Although this patient was symptom positive, the
sensitivity and specificity of the SI tool cannot be as-
sessed in the current study.
The value of this report needs to be understood in
context. There have been several efforts to develop algo-
rithms for assessing ovarian cancer symptoms [11-13,17,
18], but few have reported results from use of their index
in a study group other than the one in which it was
developed , and differences associated with methods of
administration of self-report questionnaires have not
been previously examined. The symptom index [13] pro-
vides a considerably more specific result than other
indexes with similar sensitivity and is the first to report
results from prospective use in a clinic population. If
ovarian cancer screening using symptoms is widely