C. SETHNA ET AL. 21
may occasionally be negative in children and a positive
result is not required for diagnosis. Therefore, a kidney
biopsy may be required to confirm pauciimmune glome-
rulonephritis with vasculitic or necrotizing lesions [7].
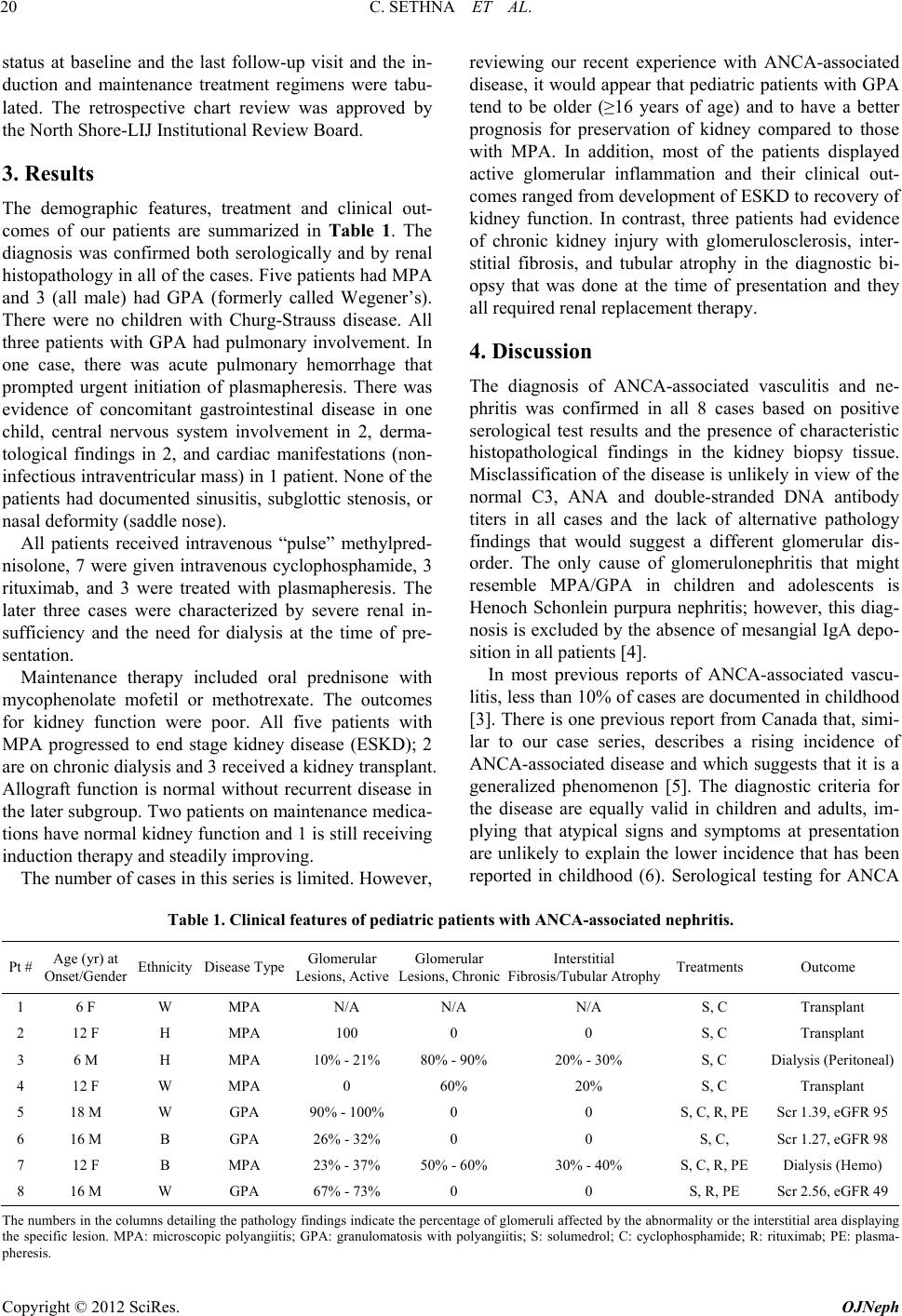
All of our cases had characteristic features of ANCA-as-
sociated disease and positive serology. The trend shows
no evidence of abating and a new case was encountered
during the preparation of this report. The patient was not
included in this series because she was 21 years of age
and would be considered an adult even though she was
cared for by pediatric subspecialists. Thus, we propose
that the increased incidence encountered over the last 2
years reflects a true change in the frequency of this com-
plex illness in pediatric patients. At present, the cause for
the sudden change in the epidemiology of ANCA-asso-
ciated disease remains a mystery.
Recent studies suggest that ANCA may develop due to
molecular mimicry with fimbrial protein antigens in bac-
teria [8]. Although there is a follow-up report that has
shed some doubt on this association [9], it raises the pos-
sibility that altered environmental exposure may account
for the surge in pediatric cases of ANCA-associated dis-
ease over the last few years.
ANCA-associated vasculitis is usually abrupt and se-
vere in onset and requires early identification to achieve
optimal outcomes. The present cases, several of whom had
irreversible kidney damage at the time of diagnosis, may
heighten awareness of ANCA-associated vasculitis in pedi-
atric patients so that serological testing is performed
promptly and aggressive therapy is administered in a
timely manner. It is worth noting that our outcomes for
kidney function were much worse than in a series of 8 chil-
dren with ANCA-associated vasculitis (7 GPA, 1 MPA),
of whom only 1 developed ESKD over a follow-up pe-
riod ranging from 11 - 30 years [10]. This suggests that
both the incidence and severity of ANCA-associated vas-
culitis in childhood may be changing. A younger age, the
diagnosis of MPA, and the presence of chronic glomeru-
lar and interstitial damage appear to be indicators of a
poor prognosis for maintenance of normal kidney func-
tion. However, children who have significant active
glomerular inflammation can respond to therapy with a
return of renal function. The logistical difficulties in im-
plementing effective but costly therapies such as plas-
mapheresis and rituximab that are required to achieve
rapid remission underscore the urgency of establishing
the diagnosis of GPA/MPA in an accurate and timely
manner [11-13].
In conclusion, ANCA-associated vasculitis is not a
new entity, but a change in epidemiology of this severe
illness warrants concern among physicians who care for
individual patients and public health officials. We en-
courage the formation of a registry through established
societies in pediatric nephrology and rheumatology to
monitor the incidence and outcomes of patients with
these rare diseases.
REFERENCES
[1] R. J. Falk and J. C. Charles Jennette, “ANCA Disease:
Where Is This Field Heading?” Journal of the American
Society of Nephrology, Vol. 21, No. 5, 2010, pp. 745-752.
doi:10.1681/ASN.2009121238
[2] A. E. Berden, F. Ferrario, E. Christian Hagen, D. R. Jayne,
J. Charles Jennette, K. Joh, I. Neumann, L. H. Noël, C. D.
Pusey, R. Waldherr, J. A. Bruijn and I. M. Bajema, “His-
topathologic Classification of ANCA-Associated Glome-
rulonephritis,” Journal of the American Society of Ne-
phrology, Vol. 21, No. 10, 2010, pp. 1628-1636.
doi:10.1681/ASN.2010050477
[3] C. E. Rodrigues, M. R. Callado, C. A. Nobre, F. E. Moura,
R. M. Vieira, L. A. de Albuquerque and W. P. Vieira,
“Wegener’s Granulomatosis: Prevalence of the Initial
Clinical Manifestations—Report of Six Cases and Re-
view of the Literature,” Revista Brasileira de Reumato-
logia, Vol. 50, No. 2, 2010, pp. 150-164.
doi:10.1590/S0482-50042010000200005
[4] R. Coppo, P. Cirina, A. Amore, R. A. Sinico, A. Radice
and C. Rollino, “Properties of Circulating IgA Molecules
in Henoch Schonlein Purpura Nephritis with Focus on
Neutrophil Cytoplasmic Antigen IgA Binding (IgA-
ANCA): New Insight into a Debated Issue. Italian Group
of Renal Immunopathology Collaborative Study on He-
noch Schonlein Purpura in Adults and Children,” Ne-
phrology Dialysis Transplantation, Vol. 12, No. 11, 1997,
pp. 2269-2276. doi:10.1093/ndt/12.11.2269
[5] S. Grisaru, G. W. Yuen, P. M. Miettunen and L. A.
Hamiwka, “Incidence of Wegener’s Granulomatosis in
Children,” The Journal of Rheumatology, Vol. 37, No. 2,
2010, pp. 440-442. doi:10.3899/jrheum.090688
[6] D. A. Cabral, A. G. Uribe, S. Benseler, K. M. O’Neil, P. J.
Hashkes, G. Higgins, A. S. Zeft, D. J. Lovell, D. J. Kings-
bury, A. Stevens, et al., “Classification, Presentation, and
Initial Treatment of Wegener’s Granulomatosis in Child-
hood,” Arthritis Rheum, Vol. 60, No. 11, 2009, pp. 3413-
3424. doi:10.1002/art.24876
[7] M. Shimizu, T. Sekiguchi, et al., “A Case of a 6-Year Old
Girl with Anti-Neutrophil Cytoplasmic Antibody- Negative
Pauci-Immune Crescentic Glomerulonephritis,” Clinical
and Experimental Nephrology, Vol. 15, No. 4, 2011, pp.
596-601. doi:10.1007/s10157-011-0423-3
[8] R. Kain, M. Exner, R. Brandes, et al., “Molecular Mim-
icry in Pauci-Immune Focal Necrotizing Glomerulone-
phritis,” Nature Medicine, Vol. 14, No. 10, 2008, pp.
1088-1096. doi:10.1038/nm.1874
[9] A. J. Roth, M. C. Brown, R. N. Smith, A. K. Badwar, et
al., “Anti-LAMP-2 Antibodies Are Not Prevalent in Pa-
tients with Antineutrophil Cytoplasmic Autoantibody Glo-
merulonephritis,” Journal of the American Society of Ne-
phrology, Vol. 23, No. 5, 2012, pp. 545-555.
[10] N. Arulkumaran, S. Jawad, S.W. Smith, L. Harper, P.
Brogan, C. D. Pusey and A. D. Salama, “Long-Term Out-
come of Paediatric Patients with ANA Vasculitis,” Pe-
Copyright © 2012 SciRes. OJNeph