Health
Vol.6 No.5(2014), Article ID:43143,6 pages DOI:10.4236/health.2014.65060
The angiotension converting enzyme (ACE) gene I/D polymorphism in different ethnic groups of geriatric age living in the Far North
![]()
1Yakutsk Science Centre of Complex Medical Problems, Siberian Branch of the Russian Academy of Medical Science, Yakutsk, Russia; nati8692@mail.ru
2Мedical Institute, North-Eastern Federal University Named after M. K. Ammosov, Yakutsk, Russia; ecapopova@yandex.ru
Copyright © 2014 Natalya Arkhipova et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In accordance of the Creative Commons Attribution License all Copyrights © 2014 are reserved for SCIRP and the owner of the intellectual property Natalya Arkhipova et al. All Copyright © 2014 are guarded by law and by SCIRP as a guardian.
Received 19 December 2013; revised 23 January 2014; accepted 31 January 2014
ABSTRACT
The study of ACE gene I/D polymorphism has been carried out in elderly, senile and long-liver patients with coronary heart disease (CHD) taking into account their nationality, age and sex. It has been recorded that with the increase of age there is a decrease in the frequency of the genotype ACE*I/*I and a tendency of increase in the frequency of the genotype ACE*D/*D. A comparative analysis of genotypes АСЕ*D/*D and АСЕ*D/*I has showed sex differences in the frequency of homozygous genotype detection. Left ventricular hypertrophy can be observed significantly more often among carriers of genotype ACE*I/*I established by Sokolow-Lyon ECG signs. Association analysis of ACE gene I/D polymorphism has registered significant differences in BMI and blood lipid parameters.
KEYWORDS
CHD; Geriatric Age; Risk Factors; ACE Gene; Non-Indigenous and Yakut Patients
1. INTRODUCTION
Republic of Sakha (Yakutia) is the biggest region in the Russian Federation with the territory of over 3 million square kilometers, occupying one fifth part of the country. More than one third of the territory of Republic is situated beyond the Arctic Circle. The population of Yakutia is less than one million. The population density is 0.3 people per 1 square kilometers, which is 28.3 times lower compared to the indicator of the Russian Federation in the whole. Yakutia differs from the other regions of Russia not only in the magnitude of its territory, but also in the harsh climatic conditions. The main population of the Republic comprises indigenous and non-indigenous people—Yakut (45.67%) and Russian (41.27%).
The frequency of cardiovascular disease (CVD) occurrence increases with the age worldwide and it is 75% of all the deaths among the people aged 65 and older [1]. The process of aging in Russia as a whole, including the Republic of Sakha (Yakutia), is accompanied by an increase in the proportion of older people in the general population [2,3]. To date, mortality caused by cardiovascular diseases in Russia remains the highest in the world [4,5]. In the structure of mortality in Republic of Sakha (Yakutia) the leading place is also taken by circulatory system diseases—46.9% [6].
More attention is paid to the study of genetic predisposition as a risk factor of CHD and candidates are being searched for the role of death genes and human longevity [7].
In recent years, a lot of money is allocated for fundamental research of aging and age-related diseases study [8]. One of the most investigated candidate genes of CHD is angiotensin converting enzyme (ACE), which is localized on the chromosome 17q23, containing 26 exons and 25 introns [9]. There is a close connection between ACE genotype and activity of an enzyme that controls the content of angiotensin II, which plays a key role in the regulation of human hemodynamics. This polymorphism is associated with multifactorial diseases, such as, myocardial infarction, stroke, asthma, insulin dependent diabetes mellitus, ischemic heart disease and the causes of aging and longevity. Revealing high-risk individuals before signs of the disease is essential for the proper medical genetic counseling. Prevention of diseases, which substantially reduces human life, is one of the approaches to increasing the actual length of the active life [10].
2. AIM
To study features of ACE gene I/D polymorphism in the group of patients with CHD of geriatric age living in the Republic of Sakha (Yakutia), according to their nationality, age and gender.
3. MATERIALS AND METHODS
Study was carried out under the joint research project of YSC ILC SB RAMS and Institute of Internal Medicine SB RAMS in Novosibirsk “Atherosclerosis: epidemiology, etiopathogenesis and development of prevention, diagnosis and treatment of the inhabitants of the Far North on the example of the population of Yakutia”. The present work had been performed from 2004 to 2009 at the Republican Hospital No. 3 of the Ministry of Health of the Republic of Sakha (Yakutia), Geriatric Centre and YSC ILC SB RAMS.
The criteria for inclusion to the study group are people aged 60 years and older with a verified diagnosis of CHD: the Minnesota category code 1.1.1.-1.2.7, 4.1-4.2, 5.1-5.2, 6-1, 7-1, 8-3 (the latter for people over age 40); exertional angina by questionnaire Rose; detection of zone violation of local myocardial contractility by echocardiography, diagnosis of myocardial ischemia during daily ECG monitoring.
Written informed consent for conduction of biomedical research in this paper was obtained from 272 patients —non-indigenous—Russian (n = 111) and Yakut (n = 161), among them 151 were men and 121 women. Average age of patients is 77.2 ± 0.5 years. Experience of living in the North of non-indigenous patients was more than 35 years at the time of the study. According to the classification of age periods (WHO, 1963), the patients were divided into three age groups: 60 - 74 years of (elder, n = 115), 75 - 86 years (senile, n = 113) and 90 years and older (long livers, n = 44). The study was approved by the local Committee on Biomedical Ethics at YSC CMP SB RAMS.
Molecular genetic studies were carried out in the Department of Molecular Genetics SB RAMS YSC ILC. DNA samples were obtained from peripheral blood lymphocytes using the phenol-chloroform extraction. Polymorphism analysis of I/D ACE gene was performed by PCR and RFLP methods. The following Sequence of oligonucleotide primers was used:
ACE F: 5’ ctg-gag-acc-act-ccc-atc-ctt-tct 3’; R: 5 “gatgtg-gcc-atc-aca-ttc-gtc-aga-t 3”.
Statistical processing of the results was performed using methods of parametric and nonparametric statistics. We calculated arithmetical mean (M), the average error of the mean value (m) for signs having a continuous distribution, and also frequency of occurrence signs with discrete values. To estimate intergroup differences in the characteristic values that have continuous distribution, we used the student t-test, and when comparing frequency values—c2-Pearson criterion.
We used Pearson’s r-criterion, Spearman’s rs-criterion and c2 Pearson criterion to make analysis of the dependence between signs. As for statistical processing of material, we used standard package of the program of applied statistical analysis (Statistica for Windows v. 6.0). A critical level of zero statistical hypothesis reliability (no significant differences or factor influences) was taken as 0.05.
4. RESULTS AND DISCUSSIONS
In the analysis of I/D polymorphism of ACE gene in 272 patients of geriatric age with CHD, the genotype frequency of АСЕ*D/*D has been amounted to 18, 8% (n = 51), АСЕ*D/*I—43, 0% (n = 117), АСЕ*I/*I—38, 2% (n = 104). No significant differences have been found in the frequency distribution of genotypes of АСЕ*D/*D, АСЕ*D/*I, АСЕ*I/ *I according to nationality and age (c2 = 4.00; p > 0.10 and c2 = 2.23; p > 0.10 respectively). However, we have noted that the frequency of the genotype АСЕ*I/*I decreases with age: in the elderly— 40, 9% (n = 47), at senile age—38, 1% (n = 43) and 90 years of age and older—31, 8% (n = 14).
As mentioned above, the proportion of genotype ACE*D/*D in our group of patients was only 18.8% (less than 1/5 of patients). After having analyzed the genotype ACE*D/*D and ACE*I/*I frequencies, we found out that with the increase of age there was a corresponding increase in relative number of patients with genotype ACE*D/*D, and the number of patients with genotype ACE*I/*I—slightly reduces (t = 1.74; p = 0.085). According to our data, the reduction in the number of carriers of this genotype occurs in the age of over 75.
Similar results were also obtained by other researchers. For example, when studying I/D polymorphism of ACE gene in different age groups of St. Petersburg residents there was revealed a significant decrease in ACE*I allele and genotype of АСЕ *I/*I among people over 70 years [10,11]. On examination of europeoid male population of Novosibirsk it was pointed out that with age there was traced a decrease of allele АСЕ*I frequency and the relevant genotypes, as well as, an increase of allele АСЕ*D and its homozygous genotype. It was also found out that АСЕ* D/*D had the smallest mortality and was higher for genotype allele АСЕ*I [12]. During a cohort study in Germany it was detected that the prevalence of D allele of ACE gene and homozygotes for this allele was higher among people over 80 years [13]. However, these findings were not confirmed in other large studies of centenarians living in France and Denmark [14]. A frequency increase of the homozygous genotype of the АСЕ*D/*D with the age seems rather contradictory, since, according to the literature, it is characterized by increased cardiovascular risk and mortality in the developed countries [15-18].
In V. N. Anisimov’s opinion [19], the data on the polymorphism of the genes, associated with a range of serious diseases, does not reveal any association with the longevity or lead to paradoxical conclusions, like in the case of a high frequency of genotype ACE*D/*D at centenarian residents of France.
We have identified gender discrepancies, when comparing carriers of homo-and heterozygous genotypes of АСЕ* D/*D, АСЕ*D/*I, АСЕ*I/*I. The frequency of genotype АСЕ*D/*D is observed somewhat higher among men (n = 35, or 23, 2%) than among women (n = 16, or 13, 2%) (χ2 = 5, 23; p = 0.072). If we compare men and women, the patients with genotypes АСЕ*D/*D and АСЕ*D/*I, it can be noted that the carriers of genotype АСЕ*D/*D are significantly more common among men (n = 35, or 68.6%) than among women (n = 16, or 31, 4%) (c2 = 5, 23; p = 0.021). This can probably be explained by the association of the genotype АСЕ*D/*D with the increased risk of CVD, which are more exposed to men than women [20].
Linkage between left ventricular hypertrophy (LVH), and I/D polymorphism of the ACE gene, which is one of the candidate genes contributing to the process of myocardial hypertrophy, is of particular interest. On the basis of series observations, there was formed the view on the role of the genotype АСЕ*D/*D as a risk factor for LVH [21-23]. For the diagnosis of LVH—an independent predictor of coronary heart disease—traditional (most commonly used) ECG-LVH criteria (Sokolow-Lyon index, Cornell voltage and Gubner-Ungerleider signs) were used. A result of research detected a slightly higher connection of Sokolow-Lyon index with genotype АСЕ* I/*I (n = 25, or 24.0%) than with the genotype of АСЕ*D/*D (n = 7, or 13.7%) and АСЕ*D/*I (n = 16, or 13.7%) (c2 = 4, 73; p = 0.092). In this case there was no association of other studied ECG signs of LVH (Cornell voltage and Gubner-Ungerleider) with homo-and heterozygous genotypes of ACE gene (Table 1).
In the group of Yakut, unlike non-indigenous people, there is a trend toward more frequent detection of genotype АСЕ*I/*I, than genotype АСЕ*D/*I (Table 2).
If in the total group of patients with genotype АСЕ* I/*I only a certain predisposition to the development of LVH (judging on the basis of Sokolow-Lyon) has been traced, then in the group of Yakut carriers of genotype АСЕ*I/*I the myocardial remodeling has been observed more frequently. In both groups, LVH is reflected more precisely by the signs of Sokolow-Lyon, than using the other two studied ECG signs of LVH (Table 3).
According to the several authors, who studied I/D polymorphism of ACE gene among patients with acute

Table 1. The frequency of genotypes АСЕ*D/*D, АСЕ*D/*I, АСЕ*I/*I in patients of geriatric age with CHD and their connection with ECG signs of left ventricular hypertrophy (n = 272).

Table 2. The frequency of detection of genotypes АСЕ*D/*I and АСЕ*I/*I in Yakut people of geriatric age with CHD (n = 161).

Table 3. Frequency of genotypes АСЕ*D/*I and АСЕ*I/*I in Yakut patients of geriatric age with CHD and their correlation with ECG-signs of LVH (n = 161).
coronary syndrome, genotypes ACE*D/*I and ACE*I/*I are associated with a favorable prognosis even after an episode of acute myocardial ischemia, but only at the age of less than 75 years. In the senile age the risk of mortality among carriers of genotype *I/*I tends to be doubled compared with carriers of genotype ACE* D/*D [24]. Based on the study made in Denmark, we can notice the relatively high risk of death in carriers of genotype АСЕ*I/*I compared with the carriers of АСЕ *I/*D and ACE *D/*D [25].The decrease in the number of patients with genotype ACE*I/*I with the age, detected by us, indirectly confirms the findings of the above mentioned authors.
Association analysis of I/D polymorphism ACE gene gave significant differences in body mass index (BMI) and blood lipids. We have revealed a BMI that corresponds to excess body weight (p < 0.05) significantly more often among patients with genotype ACE*D/*I than with ACE*D/*D. Separate studies results showed an association of АСЕ*D allele with the presence of abdominal obesity [26] and, conversely, lack of correlation of polymorphism I/D ACE gene with the increased body mass [27]. It has been found that the carriers of genotype ACE*D/*I compared with the carriers of genotype ACE*D/*D have significantly higher levels of total cholesterol (TC), cholesterol with very low density lipoproteins (VLDL), high density lipoprotein cholesterol (HDL), triglycerides (TG) (p < 0.05) (See Table 4).
The results of comparison of groups of patients with genotypes ACE*D/*D and ACE*I/*I indicate that there have been significant differences in the content blood total cholesterol, atherogenic factor (SC) (p < 0.05) and especially HDL cholesterol (p < 0.002) for almost the same values of the patients’ age (0.05 < p < 0.10) in the two groups (See Table 5).
Comparative analysis of lipid composition of the blood in the groups of carriers of genotypes ACE*D/*D, ACE*D/*I, ACE*I/*I have revealed significantly lower levels of HDL-C (H = 13, 99; p < 0.001) in the patients with genotype ACE*D/*D.
The study results are consistent with the data of other authors who have identified the highest level of HDL cholesterol in carriers of genotype ACE*D/*I in comparison with carriers of genotypes ACE*D/*D and ACE*I/*I [28]. Genotype of АСЕ*D/*D is interconnected with adverse changes in blood biochemical parameters, namely, low HDL-C [29]. In the survey of Yakut population the genotype ACE*D/*I of angiotensin-converting enzyme has been associated with increased total cholesterol and LDL cholesterol in myocardial infarction [30]. According to the results of an earlier research among patients of Moscow population with CHD there was found a correlation of D allele of ACE gene converting enzyme with high plasma levels of total cholesterol and LDL-C [31].
No interrelation of homo-and heterozygous genotypes of ACE gene has been identified with systolic and diastolic blood pressure, smoking factor and diabetes mellitus.
The observed tendency to the increase in the frequency of genotype ACE*D/*D with the age leads to the need for more in-depth analysis with the inclusion into the study probably a larger number of long-livers.
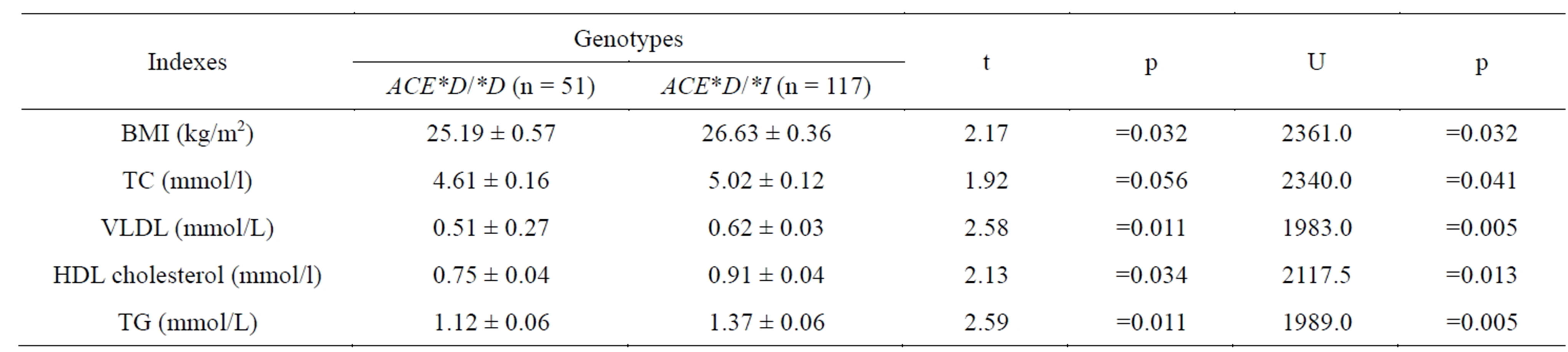
Table 4. The revealed differences when comparing the genotypes of ACE*D/*D, ACE*D/*I in patients of geriatric age with CHD (n = 168).

Table 5. Differences identified when comparing groups of carriers of genotypes ACE*D/*D, ACE*I/*I in patients of geriatric agewith CHD (n = 155).
5. CONCLUSIONS
1) With the increase in age, the number of patients with genotype ACE*I/*I decreases and the tendency to increase proportion of patients with genotype ACE*D/*D can be observed. The link between genotype ACE*I/*I with one of the ECG signs of LVH (Sokolow-Lyon) allows including it to the factors of cardiovascular risk in the group of people older than 75 years.
2) Patients with genotype АСЕ*D/*D are identified significantly more often among men, than among women.
3) There has been established an association of genotype ACE*D/*I with blood lipids and BMI.
REFERENCES
- Bello, N. and Mosca, L. (2004) Epidemiology of coronary heart disease in women. Progress in Cardiovascular Diseases, 4, 287-295. http://dx.doi.org/10.1016/j.pcad.2003.08.001
- Yakovlev, V.M. and Hite, G.Y. (2011) Basics of Geriatric Cardiology. A guide for practicing physicians. Publishing House Vidar-M, 424.
- Timofeev, L.F., Krivoshapkin, V.G. and Lazebnyk, O.A. (2012) Protection of public health in the Sakha Republic (Yakutia). Health Atlas, 212.
- Boqueria, L.A. and Gudkova, R.G. (2012) Cardiovascular Surgery—2011. Diseases and congenital anomalies of the circulatory system. Scientific Center of Cardiovascular Surgery Bakuleva RAMS, 196.
- Boitsov, S.A., Nikulina, N.N., Yakushin, S.S., et al. (2011) Sudden cardiac death in patients with coronary artery disease: Prevalence, detection and statistical accounting problems. Russian Journal of Cardiology, 2, 59-64.
- (2013) State report on condition of sanitary and epidemiological welfare of the population in the Republic of Sakha (Yakutia) in 2012. Offset, Yakutsk 226.
- Tereshchenko, S.N., Zateyschikov, D.A., Zhirkov, I.V., et al. (2009) Gene polymorphism of angiotensin converting enzyme, angiotensin II, No-synthase receptors estrogen and gender differences in their influence on the development of cardiovascular disease. Cardiology, 4, 58-62.
- Оlshansky, S.J. (2006) Future. The Longevity dividend. The scientist, 20, 28-36.
- Mattei, M.G., Hubert, C. and Alhenc-Gelas, F. (1989) Angiotensin converting enzyme gene is on chromosome 17. Cytogenetics and Cell Genetics, 51, 1041.
- Glotov, O.S. and Baranov, V.C. (2007) Genetic polymorphism of aging. Advances in Gerontology, 2, 35-55.
- Havinson, V.H., Solovieva, D.V., Strekalov, D.L., et al. (2002) Analysis of the distribution in the Russian population of some genetic markers associated with multifactorial pathologies of average and old age. Medical Academy Journal, 2, 56-66.
- Voevoda, M.E. (2001) Polymorphism and linkage with risk factors of some susceptibility genes to cardiovascular diseases in ethnic groups of Siberia, molecular epidemiological and evolutionary-genetic aspects. Ph.D. Dissertation, 53.
- Luft, F.C. (1999) Bad genes, good people, association, Linkage, longevity and the prevention of cardiovascular disease. Clinical and Experimental Pharmacology and Physiology, 26, 576-579. http://dx.doi.org/10.1046/j.1440-1681.1999.03080.x
- Blanche, H., Cabanne, L., Sanbatou, M., et al. (2001) A study of French centenarians: Are ACE and APOE associated with Longevity. Comptes Rendus de l’Académie des Sciences—Series III—Sciences de la Vie, 324, 129-135. http://dx.doi.org/10.1016/S0764-4469(00)01274-9
- Malygina, N.A., Kostomarova, I.V., Gankovskaya, O.A., et al. (1999) Angiotensin-converting enzyme gene polymorphism in patients with coronary heart disease of elderly. 4, 31-35.
- Malygina, N.A., Kostomarova, I.V. and Melent’ev, A.S. (2002) Linkage of angiotensin-converting enzyme gene polymorphism with hereditary predisposition to myocardial infarction. Clinical Medicine, 8, 25-29.
- Ruiz, J., Blanché, H., Cohen, N., et al. (1994) Insertion/deletion polymorphism of the angiotensin-converting enzyme gene is strongly associated with coronary heart disease in non-insulin-dependent diabetes mellitus. Proceedings of the National Academy of Sciences, 91, 3662- 3665. http://dx.doi.org/10.1073/pnas.91.9.3662
- O’Donnell, C.J., Lindpaintner, K., Larson, M.G., et al. (1998) Evidence for association and genetic linkage of the angiotensin-converting enzyme locus with hypertension and blood pressure in men but not women in the Framingham Heart Study. Circulation, 97, 1766-1772. http://dx.doi.org/10.1161/01.CIR.97.18.1766
- Anisimov, V.N. (2008) Molecular and physiological mechanisms of aging. 1, 481.
- US Department of Health and Human Services (2000) Healthy people 2010: Understanding and improving health. Government Printing Office, Washington.
- Moiseyev, V.S., Demurov, L.M., Kobalava, J.D., et al. (1997) ACE gene polymorphism in patients with hypertensive disease, left ventricular hypertrophy and myocardial infarction at a young age. Therapeutic Archives, 9, 18-23.
- Kamitani, A., Rakugy, H., Higaki, J., et al. (1995) Enhanced predictability of myocardial infarction in Japanese by combined genotype analysis. Hypertension, 5, 950- 953. http://dx.doi.org/10.1161/01.HYP.25.5.950
- Prasad, N., O’Kane, K.P., Johnstone, H.A., et al. (1994) The relationship between blood pressure and left ventricular mass in essential hypertension is observed only in the presence of the angiotensin-converting enzyme gene deletion allele. Quart Journal of Medicine, 11, 659-662.
- Saygitov, R.T., Glaser, M.G., Sementsov, D.P., et al. (2006) I/D polymorphism of the ACE gene in patients with acute coronary syndrome. Cardiovascular therapy and prevention, 8, 34-41.
- Frederiksen, H. (2003) Angiotensin I—converting enzyme (ACE) gene polymorphism in relation to physical performance, cognition and survival—A follow-up study of elderly Danish twins. Annals of Epidemiology, 13, 57- 65. http://dx.doi.org/10.1016/S1047-2797(02)00254-5
- Kotlovsky, M.Y., Kotlovskaya, O.S., Osedko, O.Y., et al. (2011) The deletion of allele of angiotensin-converting enzyme in people with hypertension and chronic form of CHD. Successes of Modern Science, 10, 40-43.
- Goncharova, L.N., Birlyukova, D.V., Timoshkina, E.I., et al. (2009) The study of the relationship of insertional deletion polymorphism of the angiotensin converting enzyme gene with a high body mass in patients with hypertension in different ethnic groups of the Republic of Mordovia. Cardiovascular Therapy and Prevention, 6, 5-9.
- Stepanov, V.A., Puzyrev, V.P. and Charles, R.S. (1998) Analysis of angiotensin-converting enzyme of polymorphism associations with coronary atherosclerosis, lipid levels and blood pressure. Siberian Medical, 3/4, 20-25.
- Shabalin, A.V., Governor, M.I., Chernykh, N.I., et al. (2004) Longevity—Model for studying the aging process. BULLETIN SB RAMS, 4, 11-21.
- Grigorieva, L.V. (2006) Molecular genetic study of myocardial infarction in Yakut population. Ph.D. Dissertation, 24.
- Shadrina, M.I., Slominsky, P.A., Miloserdova, O.V., et al. (2001) The analysis of ACE gene polymorphism in patients with coronary heart disease in Moscow population. Genetics, 4, 540-544.
§ ABBREVIATIONS
§ ACE—Angiotension Converting Enzyme
§ BMI—Body Mass Index
§ CHD—Coronary Heart Disease
§ CMP—Complex Medical Problems
§ CVD—Cardio Vascular Disease
§ DNA—Deoxyribonucleic Acid
§ ECG—Electrocardiography
§ HDL—High Density Lipoprotein Cholesterol
§ HLV—Hypertrophy of Left Ventricular
§ LDL—Low-Density Lipoprotein
§ PCR—Polymerase Chain Reaction
§ RFLP—Restriction Fragment Length Polymorphism
§ SB RAMS—Siberia Branch of Russian Academy of Medical Science
§ TC—Total Cholesterol
§ TG—Triglyceride
§ VLDL—Very Low-Density Lipoprotein
§ YSC—Yakut Scientific Centre