International Journal of Clinical Medicine
Vol.5 No.1(2014), Article ID:41675,8 pages DOI:10.4236/ijcm.2014.51002
Efficacy of Extracorporeal Shock Wave Lithotripsy (ESWL) versus Pneumatic Ureteroscopic Lithotripsy (URSL) for Lower Ureteral Stones Therapy in Asia: A Meta-Analysis
Tao Li, Shengjun Fu, Xing Ming, Li Yang, Ji Cheng, Zhiping Wang*
Institute of Urology, Department of Urology, Key Laboratory of Urological Diseases in Gansu Province, Gansu Nephro-Urological Clinical Center, Lanzhou University Second Hospital, Lanzhou, China.
Email: *eryzwp@lzu.edu.cn
Copyright © 2014 Tao Li et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In accordance of the Creative Commons Attribution License all Copyrights © 2014 are reserved for SCIRP and the owner of the intellectual property Tao Li et al. All Copyright © 2014 are guarded by law and by SCIRP as a guardian.
Received November 12th, 2013; revised December 10th, 2013; accepted December 31st, 2013
ABSTRACT
Objective: To assess the efficacy and safety of extracorporeal shock wave lithotripsy or pneumatic ureteroscopic lithotripsy for lower ureteral stones therapy, we sought to identify and summarize randomized controlled trials that were used to treat distal ureteral stone. Methods: Eligible studies were identified from electronic databases. Database search, quality assessment, and data extraction were performed by two reviewers independently. Our primary outcome was the stone-free rate. Secondary outcomes were the fragmentation rate, complications and the rate of re-treatment and secondary procedures. The results were assessed by Review Manager 5.0. Publication bias was evaluated by Stata 11.0. Results: 13 trials were included. Meta-analysis of pooled data showed that pneumatic ureteroscopic lithotripsy demonstrated a significant advantage over extracorporeal shock wave lithotripsy (OR = 0.14, 95% CI [0.09, 0.23], P < 0.00001) in the stone-free rate; the extracorporeal shock wave lithotripsy had statistical disadvantages over pneumatic ureteroscopic lithotripsy in the fragmentation rate of ureteral stones (OR = 0.14, 95% CI [0.05, 0.39], P = 0.0002); and the rate of re-treatment and secondary procedure was lower in pneumatic ureteroscopic lithotripsy than in extracorporeal shock wave lithotripsy (OR = 5.37, 95% CI [2.61, 11.07], P < 0.00001). Our pooled results showed that there was no statistical difference between extracorporeal shock wave lithotripsy and pneumatic ureteroscopic lithotripsy in hematuresis, ureteral stricture and urosepsis or fever. Finally extracorporeal shock wave lithotripsy had a higher incidence of colic pain than pneumatic ureteroscopic lithotripsy. Conclusion: The present meta-analysis suggested that pneumatic ureteroscopic lithotripsy had large advantages over extracorporeal shock wave lithotripsy in the treatment of lower ureteral stones.
Keywords: Efficacy of Extracorporeal Shock Wave Lithotripsy; Pneumatic Ureteroscopic Lithotripsy; Distal Ureteral Stones; ESWL; URSL
1. Introduction
Ureteric calculi is the third most common phenomenon of the urinary tract, and 70% ureteric calculi is situated in the lower third part of the ureter, known as distal ureteral stones [1]. Currently, ureterorenoscopy (URS) and extracorporeal shock wave lithotripsy (ESWL) are two treatment methods which were accepted extensively for distal ureteral stones [2]. Meanwhile, ESWL and URS have been regarded as the standard choices for ureteric calculi. Since the first introduction of ESWL in early 1980s [3], ureteral stone managements have been changed from an open approach to a minimally invasive one [4]. Some reports showed that ESWL was a safe, noninvasive and effective method to treat a majority of stones with a minimal number of complications [5,6]. By contrast, a series of limitations were revealed, such as pain and tissue trauma, stone size, location, composition, and shock energy, frequently influenced the success as the factors [7]. During the last two decades, there was a fast development in the endourological devices for manipulation and retrieval of ureteral stones [8]. Advance in intracorporeal lithotripsy has also facilitated fragmentation of these stones with pneumatic lithotripsy (URSL). URSL is a safe and highly effective procedure particularly in the distal ureter even for larger stones [9]. Guang-Qiao ZENG et al. [10] and Muhammad Islam et al. [11] recommended that URSL may be regarded as the optimal choice for the treatment of distal ureteric calculi. However, WANG Guang et al. [12] considered that ESWL was the first line treatment for patients with distal ureteric calculi. Although ESWL and URSL are currently accepted choices for the treatment of distal ureteric calculi [13,14], optimum management remains an ongoing question among urologists. However, to date, no systematic review and meta-analysis has been performed to determine the efficacy and safety between ESWL and URSL for distal ureteric calculi. Therefore, this metaanalysis was performed to evaluate the efficacy and safety between ESWL and URSL to provide more reliable evidence for the choice of stone management.
2. Methods
Relevant publications were identified through a literature search using the key words (“extracorporeal shock-wave lithotripsy” OR “extracorporeal shock wave lithotripsy”) AND (“pneumatic ureteroscopic lithotripsy” OR “ureteroscopic pneumatic lithotripsy”) in the following electronic databases: PubMed, Sciverse, the Cochrane Library, SinoMed and China Knowledge Resource Integrated Database (last search was updated on Aug. 10, 2013). We also evaluated the references of included studies to identify additional potentially associated publications.
Our primary outcome was the stone-free rate (SFR). Secondary outcomes were fragmentation rate (FR), complications and the rate of re-treatment and secondary procedures. The titles and abstracts were screened by 2 reviewers independently, who discarded the studies that were not eligible, and 2 reviewers independently assessed the retrieved titles and abstracts of all identified trials to confirm fulfillment of the inclusion criteria. Data extraction was performed independently by the same investigators using standard data extraction forms. To reduce bias, 1 of the reviewers was unaware of the source of the publication and the authors’names. Disagreements were resolved in consultation with the third reviewer. The quality of the included trials was assessed using the Cochrane Collaboration tool [15], which included random sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting, and other sources of bias. Randomised controlled trials of urolithiasis in any language were eligible. Only those studies were identified in a comparison between ESWL and URSL for distal ureteric calculi. We excluded trials in which the comparison between ESWL and URSL accompany with other management modalities or upper ureter.
3. Statistical Analysis
We analyzed the data using Review Manager Version 5.0, extracted and pooled the data for summary estimates. P< 0.05 was considered statistically significant. For the meta-analysis, we combined the data on dichotomous outcomes using the Mantel-Haenszel relative risk method. We used the chi-square statistic to assess the heterogeneity between the trials and the I2 statistic to assess the extent of inconsistency. We used a fixed-effects model for calculations of summary estimated and their 95% CI, I2 values of 25%, 50%, and 75% correspond to low, medium, and high levels of heterogeneity, unless significant heterogeneity was present, in which case, the results were confirmed using a random effects statistical model. When significant heterogeneity was present, I2 values was over 50% and data were available and sufficient, a subgroup analysis was performed to explore possible heterogeneity. Stata version 11.0 was used to assess the publication bias test.
4. Results
According to the inclusion criteria defined above, we identified 13 independent studies, including 5180 patients receiving ESWL and only 1912 patients receiving URSL (Figure 1). Table 1 showed the studies’ characteristics included in the meta-analysis. All studies [10-12, 16-25] were multicenter, double-blind, randomized and parallel-group. The included studies consisted of 11 China, 1 Turkey, and 1 Peshawar populations. Baseline information was comparable between ESWL and URSL groups. Three studies [22-24] compared upper, middle, and low ureteral stones between two procedures. The duration time of stone free rate was one week reported in one study [21]. Quality assessment of the 13 studies were showed in Table2
4.1. The Rate of Stone Free
13 available studies’ data including 7092 patients reported the rate of stone free for ESWL vs URSL. Heterogeneity was observed in pooled analysis (P < 0.00001,

Figure 1. Flow chart for selecting randomized controlled trials for analysis.
I2 = 74%). Thus, we performed meta-analysis using the random-effects model. At the follow-up end points, URSL had a significant advantage over ESWL (OR = 0.14, 95% CI [0.09, 0.23], P < 0.00001). The results were depicted in Table3 Subsequently, subgroup analysis was performed to explore the possible heterogeneity.
One study [21] reported the duration time of stone free rate was seven days. After deleting the report, the pooled results of the following 12 studies showed there was still statistical significance in the treatment between ESWL and USRL (random-effects model, M-H 0.16, 95% CI 0.10 - 0.25, P < 0.00001). Three studies [22-24] reported whole ureteral stones in these two procedures. The pooled results demonstrated there was also statistical difference between ESWL and USRL treatments after extracting the three studies (random-effects model, M-H 0.14, 95% CI 0.08 - 0.25, P < 0.00001).
4.2. The Fragmentation Rate
There were 6 studies [16-19,21,23] (851 ESWL and 607 URSL) analyzing the FR between ESWL and URSL treatments in distal ureteric calculi. Heterogeneity was assessed in pooled analysis (P = 0.02, I2 = 61%). Therefore, we performed meta-analysis using the random-effects model. The pooled results showed that the ESWL procedure had statistical disadvantages over URSL in FR of ureteral stones (OR = 0.14, 95% CI [0.05, 0.39], P = 0.0002) (Table 3). After deleting the study that the duration time of stone free was seven days [21], the pooled studies showed that there was still statistical difference in FR between ESWL and URSL (random-effects model, M-H 0.08, 95% CI 0.05 - 0.15, P < 0.00001).
4.3. Re-treatment and Secondary Procedure Rate
9 available studies’ data including 6099 patients reported the re-treatment and secondary procedure rate for ESWL vs URSL. Heterogeneity was observed in pooled analysis (P < 0.00001, I2 = 81%). We performed meta-analysis by the random-effect model. The result of meta-analysis showed that there was statistically significant difference between ESWL and URSL procedure (OR = 5.37, 95% CI [2.61, 11.07], P < 0.00001). The URSL had a lower re-treatment and secondary procedure rate than ESWL procedure (Table 3). After deleting the study which reported the duration time of stone free was seven days [21], the result showed that there was still a significant difference between two procedures (random-effects model, M-H 6.02, 95% CI 2.78 - 13.04, P < 0.00001).
4.4. Complications
There was 10 studies [10-11,16-21,24,25] reported various complications caused by ESWL and URSL. The most common adverse events were colic pain, hematuresis, and ureteral stricture. Five studies [17,18,20,24,25] reported the incidence of hematuresis, however, the pooled results showed there was no statistically significant difference in hematuresis between ESWL and URSL (P = 0.39). Six studies [11,16-18,20,24] compared the difference of the adverse events of colic pain, the pooled results showed URSL could effectively reduce the rate of colic pain than ESWL (P = 0.04). The pooled studies of four studies’ data [10,19,21,25] revealed there was no statistically significant difference between ESWL and URSL (P = 0.17) in ureteral stricture. Four studies [16, 17,24,25] reported the complication rate of urosepsis/ fever, and the result showed there was also no statistically significant difference (P = 0.21). Eight studies [10,11, 16,18-20,24,25] reported the URSL modality could cause ureteral perforation, which was no one occurred in ESWL group.
4.5. Publication Bias
We assessed the publication bias of included studies, the
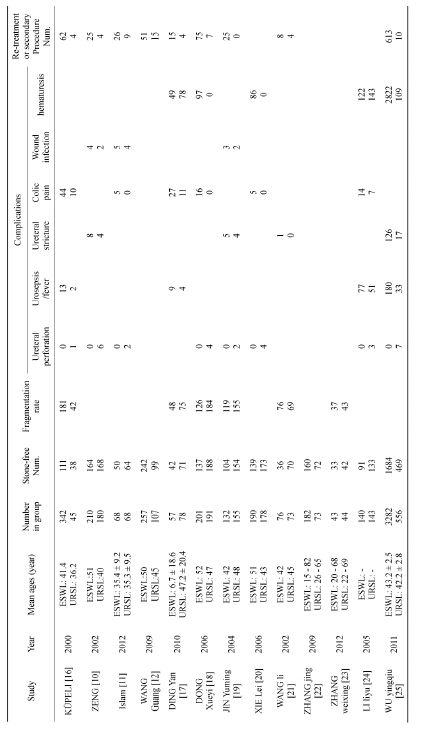
Table 1.Baseline characteristics of included studies.

Table 2. Methodological quality of included studies.
Table 3. Results of meta-analysis for the efficacy and safety for distal urinary stone in ESWL or URSL.
E: ESWL; U: URSL.
result showed that there was no statistically significant difference in these studies (P = 0.525). Therefore, we could conclude there was a small publication bias in this review with meta-analysis.
5. Comment
With various techniques developing, ESWL and URSL have revolutionized the treatment of distal ureteric calculi and afforded obvious advantages over conventional open surgical lithotomy [26]. However, the first optimal strategy was still a controversial issue. A number of studies suggested that ESWL can be regarded as the first treatment option for patients with lower ureteral stones compared with URSL [11,12,16], due to its noninvasive nature, fewer complications, faster convalescence, and shorter operative time. Several reports showed the success rates >90% in those patients performed ESWL [27,28]. By contrast, some papers reported that URSL had an advantage over ESWL in high stone free rate, reliable efficacy for the treatment of distal ureteric calculi [17,20,21]. Some small sample studies are limited by their sample size and have a power too low to detect effects that may exist. Combining data from those studies have an advantage of increasing the statistical power. In order to provide comprehensive and reliable evidence, we performed this review with meta-analysis to evaluate the efficiency and safety in the treatment of distal ureteric calculi compared between ESWL and URSL modalities.
Muhammad Islam [11] and BORA KÜPELI [16] reported the outcome of these two treatment modalities was similar in SFR, and the rates were 74% and 32.4%, respectively. The SFR performed by ESWL seems to be related to stone location. Our pooled meta-analysis results showed that the URSL procedure cause a higher value in SFR than ESWL treatment (OR = 0.14, P < 0.00001). FR is also a crucial factor to evaluate the efficiency of these two treatment modalities. WANG Li [21] reported the overall successful rate of stone fragmentation of URSL was lower than that of ESWL (94.5% vs 100%). The results indicated that URSL had a disadvantage over ESWL in stone FR. However, several studies showed a different conclusion that ESWL could not increase the FR. The pooled results indicated that the treatment of URSL modality had an advantage over ESWL in FR (OR = 0.14, P = 0.0002).
Several factors might impact the efficiency of stone elimination, such as location and stone size, composition, obstruction, as well as proficiency of the operator. Several studies reported [28,29] that ESWL for distal ureteral stones appeared to be an attractive treatment option. Nevertheless, some patients whose stones were not pulverized always need a re-treatment or repetitive ESWL modality. Our study indicated that the incidence of re-treatment or secondary procedure in ESWL was higher than in URSL for patients with lower ureteral stones (OR = 5.37, P < 0.00001).
Demirbas M et al. [28] reported a few patients who performed ESWL encountered self-limiting hematuria, dysuria, and pain in 2004. WU et al. [21] showed that the incidence of fever and hematuria in ESWL group was significantly higher than that in URSL group. BORA KÜPEL et al. [16] reported the main complications involved urosepsis, ureteral perforation, and colic pain. However, their reports showed there was no statistically significant difference in the complication rates between ESWL and URSL (P = 0.32, P = 0.25). Our pooled results showed that there was also no statistically significant difference between ESWL and URSL in hematuresis, ureteral stricture, urosepsis or fever (P = 0.39, P = 0.17, P = 0.21, respectively), but ESWL had a higher incidence of colic pain than URSL (P = 0.04). The reason maybe that the probe of URSL could closely contact with stones, which rarely generates thermal energy resulting in slight and short damage in ureteral mucosa, and the amplitude was less than 2 mm. Several studies [10,11, 18-20,24,25] indicated that the complication of ureteral perforation appeared in URSL group, and actually there was no one patient occurred in ESWL. It is evident that ESWL is the least invasive treatment option. Therefore, we could conclude that URSL was a risk factor for ureteral perforation.
Heterogeneity is a possible problem when accounting the results of the present meta-analysis. In pooled analysis results, significant heterogeneity existed in comparison of stone free rate, fragmentation rate, and re-treatment or secondary procedure. So we performed subgroup analysis by excluding the studies which involved 7 days’ duration time of stone free and whole urethra. The reason may be that different rates were caused by different locations of ureter.
Some limitations of this meta-analysis should be assessed. First, because published articles were only included in the meta-analysis, publication bias might existed, and unpublished reports might show less positive results [30]. Second, approximately all studies came from China. Thus, more studies are needed from other countries to evaluate the efficiency between ESWL and URSL. Third, the sample size of some studies was relatively small, while a more precise analysis should be conducted if more data were available. Fourth, our results could not evaluate the stone size’ diversity between two treatment modalities, and the precise option between ESWL and URSL needed to be performed.
5. Conclusion
The present meta-analysis suggested that URSL had more advantages over ESWL in the treatment of lower ureteral stones disease. There was no statistical difference between ESWL and URSL in adverse events of hematuresis, ureteral stricture and urosepsis or fever. URSL had an advantage of decreasing the incidence of colic pain over ESWL, but it could easily cause ureteral perforation. Due to the limitations of the analysis noted above, more efficient performance of higher quality, large samples, and more rigorous, long-term randomized controlled trials are warranted to verify the efficacy and safety between ESWL and URSL.
Conflict of Interest
None.
[1] REFERENCES
[2] M. Y. Zhang, S. T. Ding, J. J. Lv, et al., “Comparison of Tamsulosin with Extracorporeal Shock Wave Lithotripsy in Treating Distal Ureteral Stones,” Chinese Medical Journal (English), Vol. 122, No. 7, 2009, pp. 798-801.
[3] M. J. Bader, B. Eisner, F. Porpiglia, et al., “Contemporary Management of Ureteral Stones,” European Urology, Vol. 61, No. 4, 2012, pp. 764-772. http://dx.doi.org/10.1016/j.eururo.2012.01.009
[4] C. Chaussy, J. Schuller, E. Schmiedt, H. Brandl, D. Jocham and B. Liedl, “Extracorporeal Shock-Wave Lithotripsy (ESWL) for Treatment of Urolithiasis,” Urology, Vol. 23, No. 5, 1984, pp. 59-66. http://dx.doi.org/10.1016/0090-4295(84)90243-7
[5] M. L. Paik, M. A. Wainstein, J. P. Spirnak, et al., “Current Indications for Open Stone Surgery in the Treatment of Renal and Ureteral Calculi,” The Journal of Urology, Vol. 159, No. 2, 1998, pp. 374-378. http://dx.doi.org/10.1016/S0022-5347(01)63922-3
[6] I. Gecit, S. Kavak, E. K. Oguz, et al., “Lithotripsy Tissue Damage in Kidney, Adrenal Glands and Diaphragm Following Extracorporeal Shock Wave,” Toxicol Ind Health, 2012. http://dx.doi.org/10.1177/0748233712462481
[7] A. Skolarikos, G. Alivizatos and J. de la Rosette, “Extracorporeal Shock Wave Lithotripsy 25 Years Later: Complications and Their Prevention,” European Urology, Vol. 50, No. 5, 2006, pp. 981-990. http://dx.doi.org/10.1016/j.eururo.2006.01.045
[8] P. Larcher, O. De Cobelli, L. Carmignani, et al., “Prognostic Parameters in Extracorporeal Lithotripsy,” Archivio Italiano di Urologia, Nefrologia, Andrologia: Organo Ufficiale dell’Associazione per la Ricerca in Urologia, Vol. 61, No. 4, 1989, pp. 361-364.
[9] R. J. Leveillee and L. Lobik, “Intracorporeal Lithotripsy: Which Modality Is Best?” Current Opinion in Urology, Vol. 13, No. 3, 2003, pp. 249-253. http://dx.doi.org/10.1097/00042307-200305000-00014
[10] L. Tunc, B. Kupeli, C. Senocak, T. Alkibay, S. Sözen, U. Karaoglan, et al., “Pneumatic Lithotripsy for Large Ureteral Stones: Is It the First Line Treatment?” International Urology and Nephrology, Vol. 39, No. 3, 2007, pp. 759- 764. http://dx.doi.org/10.1007/s11255-006-9084-7
[11] G.-Q. Zeng, W.-D. Zhong, Y.-B. Cai, et al., “Extracorporeal Shock-Wave versus Pneumatic Ureteroscopic Lithotripsy in Treatment of Lower Ureteral Calculi,” Asian Journal of Andrology, Vol. 4, No. 4, 2002, pp. 303-305.
[12] M. Islam and A. Malik, “Ureteroscopic Pneumatic versus Extracorporeal Shock Wave Lithotripsy for Lower Ureteral Stones,” J Coll Physicians Surg Pak., Vol. 22, No. 7, 2012, pp. 444-447.
[13] G. Wang, M. F. Chen, L. Wang, et al., “Comparison of the Efficacy and Side Effects of Pland Eswl in Treating Distal Ureteral Calculi,” Modern Hospital, Vol. 9, No. 3, 2009, pp. 34-35.
[14] S. R. El-Faqih, I. Husain, P. E. Ekman, et al., “Primary Choice of Intervention for Distal Ureteric Stone: Ureteroscopy or ESWL?” British Journal of Urology, Vol. 62, No. 1, 1988, pp. 13-18. http://dx.doi.org/10.1111/j.1464-410X.1988.tb04257.x
[15] M. S. Pearle, R. Nadler, E. Bercowsky, et al., “Prospective Randomized Trial Comparing Shock Wave Lithotripsy and Ureteroscopy for Management of Distal Ureteral Calculi,” The Journal of Urology, Vol. 166, No. 4, 2001, pp. 1255-1260. http://dx.doi.org/10.1016/S0022-5347(05)65748-5
[16] J. Higgins and S. Green, “Cochrane Handbook for Systematic Reviews of Interventions, Version 5.0.2,” The Cochrane Collaboration, 2009, pp. 149-190. http://www.cochrane-handbook.org
[17] B. Küpeli, T. Alkibay, Z. Sinik, et al., “What Is the Optimal Treatment for Lower Ureteral Stones Larger than 1 cm?” International Journal of Urology, Vol. 7, No. 5, 2000, pp. 167-171. http://dx.doi.org/10.1046/j.1442-2042.2000.00162.x
[18] Y. Ding, Y. Q. Gu and P. P. Qian, “Comparison of Ureteroscopic Pneumatic Lithotripsy and Extracorporeal Shock-Wave Lithotripsy for Middle and Lower Ureteral Calculi,” China Modern Doctor, Vol. 48, No. 35, 2010, pp. 127-128.
[19] X. Y. Dong, H. T. Zhao, Y. X. Wang, et al., “Comparison of Ureteroscopy Pneumatic Lithotripsy and ESWL in the Treatment of Distal Ureteral Calculi,” Journal of University, Vol. 5, No. 2, 2006, pp. 43-46.
[20] Y. M. Jin, P. Li and Z. Y. Deng, “Comparison between Effectiveness of Lower and Middle Ureteric Calculi Treated by ESWL and That by TUPL,” China Medical Engineering, Vol. 12, No. 6, 2004, pp. 78-82.
[21] L. Xie, X. Y. Yu, W. J. Li, et al., “Comparison of Ureteroscopy Pneumatic Lithotripsy and Extracorporeal Shock Wave Lithotripsy in the Treatment of Distal Ureteral Calculi,” Chinese Journal of Primary Medicine and Pharmacy, Vol. 13, No. 6, 2006, pp. 910-911.
[22] L. Wang, Y. Wang and T. Li, “A Comparative Study on ESWL and Ureteoslopic Pneumatic Lithotripsy for Ureteral Stones,” Hebei Medical Journal, Vol. 24, No. 11, 2002, pp. 886-887.
[23] J. Zhang, G. Z. Wang, N. Jiang, et al., “Comparison of Three Procedures for Treatment of Ureteral Calculus,” Journal of Bengbu Medical College, Vol. 34, No. 2, 2009, pp. 140-142.
[24] W. X. Zhang, S. D. Yang, H. B. Zhang, et al., “Comparison of Emergency Ureteroscopic Lithotripsy and Extracorporeal Shock Wave Lithotripay in the Treatment of Ureteral Stones with Acute Renal Colic,” China Medcine and Pharmacy, Vol. 2, No. 9, 2012, pp. 73-75.
[25] L. Y. Li, Z. X. Tao, L. Luo, et al., “Comparison of Ureteroscopic Pneumatic Lithotripsy and Extracorporeal Shock-Wave Lithotripay for Ureteric Calculi,” Journal of Clinical Urology, Vol. 20, No. 6, 2005, pp. 326-330.
[26] Y. Q. Wu, L. J. Wu and G. Q. Chen, “Comparison the Efficacy of Middle and Lower Ureteric Calculus Treated by URL and ESWL,” China Modern Doctor, Vol. 49, No. 29, 2011, pp. 36-37.
[27] G. M. Preminger, H. G. Tiselius, D. G. Assimos, et al., from American Urological Association Education and Research, Inc.; European Association of Urology, “2007 Guideline for the Management of Ureteral Calculi,” European Urology, Vol. 52, No. 6, 2007, pp. 1610-1631. http://dx.doi.org/10.1016/j.eururo.2007.09.039
[28] A. Kose and M. Demirbas, “The ‘Modified-Prone Position’: A New Approach for Treating Prevesical Stones with Extracorporeal Shock Wave Lithotripsy,” BJU International, Vol. 93, No. 3, 2004, pp. 369-373. http://dx.doi.org/10.1111/j.1464-410X.2003.04619.x
[29] M. Demirbas, A. C. Kose, M. Samli, et al., “Extracorporeal Shockwave Lithotripsy for Solitary Distal Ureteral Stones: Does the Degree of Urinary Obstruction Affect Success?” Journal of Endourology, Vol. 18, No. 3, 2004, pp. 237-240. http://dx.doi.org/10.1089/089277904773582822
[30] F. J. Anglada-Curado, P. Campos-Hernández, J. Carrasco-Valiente, et al., “Extracorporeal Shock Wave Lithotripsy for Distal Ureteral Calculi: Improved Efficacy Using Low Frequency,” International Journal of Urology, Vol. 20, No. 2, 2012, pp. 214-219. http://dx.doi.org/10.1111/j.1442-2042.2012.03133.x
[31] M. Egger, G. D. Smith and M. Schneider, “Systematic Reviews of Observational Studies,” In: M. Egger, G. D. Smith and D. G. Altman, Eds., Systematic Reviews in Healthcare Meta-Analysis in Context, BMJ Publishing, London, 2001, pp. 211-227.
Abbreviations
ESWL: extracorporeal shock wave lithotripsy URSL: pneumatic ureteroscopic lithotripsy URS: Ureterorenoscopy SFR: stone-free rate
NOTES
*Corresponding author.