International Journal of Clinical Medicine
Vol.1 No.1(2010), Article ID:2529,4 pages DOI:10.4236/ijcm.2010.11002
Aerobic Threshold for Exercise Prescription
![]()
Center of Sports Medicine –University of Florence, Florence, Italy.
Email: laura.stefani@unifi.it
Received July 10th, 2010; revised August 10th, 2010; accepted August 11th, 2010.
Keywords: sedentary, exercise as prescription, intensity of exercise, Cardio pulmonary test
ABSTRACT
The Aerobic Threshold (AerT), is an aged cardiovascular parameter not commonly used to evaluate the heart’s performance in athletes. It indirectly evaluated by ventilator parameters during Cardio Pulmonary Test (CPT). Considering that” exercise as prescription therapy “for the diseases, includes training normally established around at the 40% of the peak VO2, this parameter could be taken in care as initial level for the effort prescribed. The aim of the study was to estimate the behavior of the AerT and also Anaerobic Threshold (AT), VO2max in sedentary people. A group of athletes coming from different sports at the same and highest dynamic component were enrolled as control. A group of 41 athletes (16 soccer, 10 basket and 15 cyclists) and 9 healthy subjects were submitted to a CPT. The AerT, AT (assessed by V-slope method) and VO2max were evaluated. The statistical analysis was performed with T student test (P < 0.05 significant). As expected in sedentary all the values were lower than athletes, however for Aer T value appears to be not significantly inferior respect of this one, with the exclusion of the comparison with the cyclists. In sedentary the AerT measure seems to give additional information in evaluating the cardiovascular performance. The VO2max and AT remain the main parameters in defining the athletes performance. Therefore we cannot exclude any further utility of the AerT in normal subject but regularly trained.
1. Introduction
The Cardio Pulmonary Test (CPT) is currently considered the best tool to determine the production of physical energy by the measurement of the aerobic metabolism.
Several variables are usually considered in the CPT, however among them the main parameter for the assessment of the heart performance, is the maximum oxygen uptake (VO2max) expressed in ml/kg/min [1].
Particularly in athletes this parameter is used to estimate the physical performance and different values of this one normally typify diverse kinds of sports [2].
The degree of the VO2max depends in fact on the cardiovascular workload that is strictly related to a specific sport discipline. The regular training determines a progressive enhancement of the parameters directly associated with the athletes performance and therefore the sports are consequently classified in a major” static or dynamic“component [3].
Literature reports however some other parameters derived from CPT, like the anaerobic threshold (AT) [4] and the aerobic threshold (AerT) [5] expressed as a percentage of VO2max.
While the AT determination is employed particularly in athletes to classify the fitness level and to follow the effects of physical training [6], on the contrary the AerT is not currently used in athletes population for the poor relationship with an high performance level, but it is use among the deconditioned patients where the 20% to 40% of their VO2max should be the initial intensity of exercise [7].
The last one has been recently considered in evaluating non-athletes subjects, even if regularly trained, where the physical exercise is prescribed as therapy to contrast the risks factors derived from an improper life style.
2. Aim
The main aim of this study it is to compare VO2max, AT and AerT values of the three different kinds sports, included into the same class, in order to better discover any possible difference among them.
3. Materials and Method
Sample: The study was conducted on a sample of 9 healthy non-athletes subjects (6 male, 3 female) similar for the general characteristics (Table 1) matched with a control group of 41 subjects athletes from three different kinds of sport (16 soccer players, 15 cyclists and 10 basketball players).
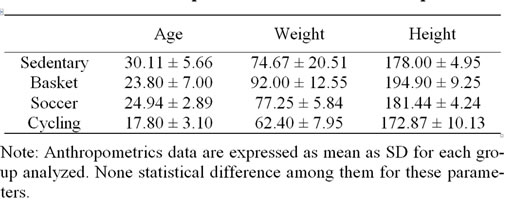
Table 1. Anthropometrics measures of sample
Following the Sport Classification [3], cycling, basketball and soccer are all included in the group with high dynamic component, with static component at high level for the first, moderate level for the second and low level for the third. Therefore global cardiovascular load shows some slight differences for each sport [3].
Experimental design: All the examinations were performed at the Sports Medicine Centre, of the University of Florence - Italy. All the subjects enrolled, following our ethical internal committee, gave their oral consent to participate to the study; the research protocol was approved by the Ethics Committee of the Faculty of Medicine and Surgery of Florence. Every subject enrolled has undergone to a incremental and maximal cardiopulmonary test (CPT).
For the football players, basketball players and the healthy subjects the treadmill test was used, while for cycling the cycle ergometer was preferred considering the specificity of athletic movements [8]..
Before to start, all the subjects were examined by a physician using a dynamic spirometry test and electrocardiogram (ECG) performing to confirm normal lung and heart function.
The respiratory gas measurements were obtained using a Schiller Cardiovit Ergo-Spiro CS 200 (Schiller AG, Baar, Switzerland). Calibrations of flow transducer and gas analysers were performed daily. The transducer with mouthpiece detecting breath by breath registrations of oxygen uptake (VO2), expired CO2 (VCO2), minute ventilation (VE).
The treadmill test: The CPT was performed by he Schiller Cardiovit Ergo-Spiro CS 200 treadmill (Schiller AG, Baar, Switzerland). The exercise test was performed following the modified Bruce protocol (Table 2). In this context the slope and the velocity of the ramp increase at a lower workload than the standard test. The protocol is a protocol appositely modified to guarantee a progressive enhancement of the effort.
The first two stages of the Modified Bruce Test are performed at a 2.7 km/h and 0% grade and 2.7 km/h and 5% grade, and the third stage corresponds to the first stage of the Standard Bruce Test protocol.
The ramp treadmill protocols offers also the advantage of steady gradual increases in work rate for a better estimation of the functional capacity [9].
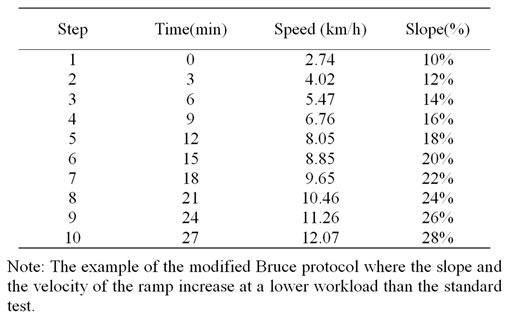
Table 2. Modified Bruce test protocol
The cycle ergometer test: The cycling exercised on a Schiller Cardiovit Ergo-Spiro CS 200 cycle ergometer (Schiller AG, Baar, Switzerland). During exercise the cadence should be held at a constant 70 rep/min, the first workload was 25 W and increasing 25 W every 2 minutes to subjective exhaustion.
AerT measurement: As literature reports the presence of two points of discontinuities during an incremental effort correspond to the AerT and AT. These discontinuities are observed in ventilator curve response or in the lactate plasma level curve response (correspond 2 mmol and 4 mmol respectively).
They substantially are the transition from aerobic to anaerobic metabolism [5,10].
The first of these points of the curve discontinuities is coincident with AerT. It is associated with the correspondent workload value and it is coincident with the first sustained increase in VE (expressed L/min) as a response of increasing of exercise intensity [11]. AerT were also evaluated that 2 mmol of blood lactate [12]. However few data are now available in literature about the current employment of the AerT, and few results are present about the comparison of this one with the other parameters obtained during CPT, mainly if it is measured in normal subjects but regularly trained [13].
The second discontinuities corresponds to the AT. It is an equilibrium period between the lactate production and the lactate elimination (maximal lactate steady state, MLSS) [14], and it is generally associated with the blood lactate concentration of 4 mmol [12].
Measure of Aerobic Threshold: Following the literature, the AT values were obtained during the CPT by V-Slope method: this method identify AT as the VO2 at which the change in slope of the relationship of VCO2 to VO2 occurs [15]. VO2max measurement: Achieving a clear plateau in VO2 has traditionally been used as the best evidence of VO2max. VO2max is the best index of aerobic capacity and the gold standard for cardio respiratory fitness. It represents the maximal reachable level of oxidative metabolism involving a large group of muscles. However, mainly in some clinical testing situations, a clear plateau may not be achieved before symptom limitation of exercise [16,17].
The value of maximum oxygen uptake (VO2max), anaerobic threshold (AT), aerobic threshold (AerT) are expressed in ml/kg/min.
Statistical analysis was performed using the SPSS 13.0 package for Windows XP. All data are expressed as mean ± Standard Deviation (SD). The groups were compared using ANOVA test. A probability value (p) of < 0.05 was considered statistically significant.
Confidence intervals of 95% percent for difference between methods were calculated.
4. Results
All the values of the AT and Aer T are expressed in mlO2 /kg/min and in percent of VO2max (Table 3).
The results show an increase of the parameters calculated either in sedentary or in control subjects.
Particularly for the AerT, the averaged value is 18.36 ± 3.35 mlO2/min/kg in sedentary, 22.76 ± 5.34 mlO2/ min/kg in basket, 24.00 ± 4.72 mlO2/min/kg for soccer and 28.47 ± 7.52 mlO2/min/kg for cycling. These values correspond around to a 40% of VO2max in all sample and they are significantly higher in the cyclist group compared to the healthy one (p < 0.05).
On the other hand the AT value is a percent of VO2 max estimated around the 70% of VO2max for basket and soccer, around 76% VO2max for cycling while it is around 65% for sedentary subjects. It demonstrates the same trend of AerT parameter, with a lower value in healthy subjects, highest in cycling and approximately in the middle for basket and soccer.
The AT values are statistically higher in athletes vs. sedentary (p < 0.01), however no difference is evident between soccer and basketball group (p = 0.25).

Table 3. Data of AerT, Aerobic Threshold; AT, Anaerobic Threshold by V-slope method; VO2max, maximum oxygen uptake of samples
Note: data of the AT and AerT are expressed in mlO2/kg/min and in percent of VO2max; all the values increase during the effort either in sedentary or in control group (athletes). The behaviour of the AerT showed in the former a particular trend to enhance respect of the other parameters that remedains significantly lower than in athletes.
As expected the VO2max parameter reports a progressive and significant increase (p < 0.01) of the values in athletes globally considered (64.20 ± 6.95 mlO2/min/kg) respect of the healthy group (43.25 ± 9.30 mlO2/min/kg).
However, in addition to this feature, the selected analysis of the behaviour of VO2max for each sport considered in the study, demonstrates a statistical difference among them (VO2max in basket is 58.23 ± 5.25 mlO2/min/kg, in soccer 61.96 ± 5.94 mlO2/min/kg, in cycling 72.40 ± 9.65 mlO2/min/kg with p = < 0.05) with the exclusion of the comparison between soccer and basketball (p = 0.12).
5. Discussion
There are practical reasons for assessing a subject by CPT. AerT, AT and VO2max are the main indexes of exercise intensity to provide guidelines for exercise training. The intensity of training resulting from these parameters may optimize the intensity-duration relationship. AT is highly related to the performance in a various endurance activities, in many cases the relationship is stronger than those between VO2max and performance [18].
AerT actually is less frequently considered during an incremental effort because CPT is mainly used in evaluating patient with heart disease where a decrease of VO2max is considered as a universal marker of reduced exercise capacity and therefore it represents the onset in assessing the reduction of the exercise tolerance [19]. It is note that athletes may attain values of VO2max over 20 times their resting values [20].
On the contrary the AerT, enclosing a restricted application in athletes, it has been more commonly linked to a people with a low intensity of physical activity, in fact the intensity of effort required for treatment is generally between 60% and 80% of the maximum heart rate. The results of this study show the AerT has a peculiar trend in healthy subject’s respect of athletes, supporting the hypothesis to play an important role to set protocols training for people where the physical activity can be used as a therapy. We cannot therefore exclude any further importance of the AerT in normal subject regularly trained where this parameter could be appreciated as the minimum intensity of the effort executed. This could be crucial point to decide the term of the “exercise as prescription”.
The VO2max and AT remain however the main parameters in defining the athletes performance. Cyclist have the highest value for every CPT parameters, the static component of the effort may have an additional role in the chronic cardio – pulmonary sport adaptation.
Moreover particularly for the general population where the exercise can be prescribed with therapeutical impact the AT could represent the upper limit of the working range.
6. Limits of the Study
The study involves a quite small cohort of subjects and therefore the results obtained cannot be considered definitive. The correct use of the AerT instead of AT in non-athletes subjects to establish the degree of physical exercise, will need further assessment of a possible relationship of this parameter with other factors characterizing the body composition. Moreover to verify the effective clinical utilization of these parameters on the general population in terms of exercise as prescription, it will need more investigations in future.
7. Acknowledgments
None founding sources were used to obtain the results of the present study and the data do not constitute endorsement.
REFERENCES
- I. M. Weisman and R. J. Zeballos, “Clinical Exercise Testing,” Clinics in Chest Medicine, Vol. 22, No. 4, December 2001, pp. 679-701.
- J. H. Wilmore and D. L. Costill, “Physiology of Sports and Exercise,” Human Kinetics, Champaign, Churchill Livingstone, New York, 2004.
- J. H. Mitchell, W. Haskell, P. Snell and S. P. van Camp “Task Force 8: Classification of Sports 10,” Journal of American College of Cardiology, Vol. 45, No. 8, April 2005, pp. 1364-1367.
- K. Wasserman, B. J. Whipp, S. N. Koyal and W. Beaver “Anaerobic Threshold and Respiratory Gas Exchange during Exercise,” Journal of Applied Physiology, Vol. 35, No. 2, August 1973, pp. 236-243.
- J. S. Skinner and T. H. McLellan, “The Transition from Aerobic to Anaerobic Metabolism,” Research Quarterly Exercise and Sport, Vol. 51, No. 1, March 1980, pp. 234- 248.
- R. Casaburi, “Physiologic Responses to Training,” Clinics in Chest Medicine, Vol. 15, No. 2, June 1994, pp. 215-227.
- J. N. Cohn, “Quantitative Exercise Testing for the Cardiac Patient: The Value of Monitoring Gas Exchange: Introduction,” Circulation, Vol. 76, No. (Suppl. 6) 1987, pp. S6-1- S6-2.
- R. T. Withers, W. M. Sherman, J. M. Miller and D. L. Costill, “Specificity of the Anaerobic Threshold in Endurance Trained Cyclists and Runners,” European Journal of Applied Physiology, Vol. 47, No. 1, August 1981, pp. 93-104.
- J. Myers, N. Buchanan and D. Walsh, “Comparison of the Ramp Versus Standard Exercise Protocols,” Journal of American College of Cardiology, May 1991, Vol. 17, No. 6, pp. 1334-1342.
- W. Kindermann, G. Simon, J. Keul, “The Significance of the Aerobic-Anaerobic Transition for Determination of Work Load Intensities during Endurance Training,” European Journal of Applied Physiology, Vol. 42, No. 1, September 1979, pp. 25-34.
- P. Palange and F. Schena, “Cardiopulmonary Exercise Testing – Theory and Applications,” COSMED, 2001, pp. 230-231.
- A. Mader, H. Heck and W. Hollmann, “Evaluation of Lactic Acid Anaerobic Energy Contribution by Determination of Post Lactic Acid Concentration of Ear Capillary Blood in Middle Distance Runners and Swimmers,” In: F. Landry and W. Orban, Eds., Exercise Physiology, Symposia Specialists Incorporated, Florida, 1976, pp. 187-199.
- W. L. Beaver, N. Lamarra and K. Wassermann, “Breath-by Breath Measurement of True Alveolar Gas Exchange,” Journal of Applied Physiology, Vol. 51, No. 6, December 1981, pp. 1662-1675.
- R. Beneke and S. P. von Duvillard, “Determination of Maximal Lactate Steady State Response in Selected Sports Events,” Medicine & Science in Sports & Exercise, Vol. 28, No. 2, February 1996, pp. 241-246.
- W. L. Beaver, K. Wasserman, B. J. Whipp, “A New Method for Detecting Anaerobic Threshold by Gas Exchange,” Journal of Applied Physiology, Vol. 60, No. 6, June 1986, pp. 2020-2027.
- J. Myers, D. Walsh, N. Buchanan and V. F. Froelicher, “Can Maximal Cardiopulmonary Capacity be Recognized by a Plateau in Oxygen Uptake?” Chest, Vol. 96, No. 6, December 1989, pp. 1312-1316.
- T. D. Noakes, “Maximal Oxygen Uptake: ‘Classical’ Versus ‘Contemporary’ Viewpoints: A Rebuttal,” Medicine and Science in Sports and Exercise, September 1998, Vol. 30, No. 9, pp. 1381-1398.
- P. J. Maud and C. Foster, “Physiology Assessment of Human Fitness,” 2nd Edition, Human Kinetics Publishers, Champaign, 2006, pp. 66-67.
- N. L. Jones and K. J. Killian, “Exercise Limitation in Health and Disease,” New England Journal of Medicine, Vol. 343, No. 9, August 2000, pp. 632-641.
- B. D. Johnson, K. W. Saupe and J. A. Dempsey, “Mechanical Constraints on Exercise Hyperpnoea in Endurance Athletes,” Journal of Applied Physiology, September 1992, Vol. 73, No. 3, pp. 874-886.