Open Journal of Rheumatology and Autoimmune Diseases
Vol.07 No.03(2017), Article ID:78176,6 pages
10.4236/ojra.2017.73014
Knee Osteoarthritis and Risk Factors Associated
Lamini N’Soundhat Norbert Edgard*, Mouelé Mboussi Paméla Chardène, Nkouala-Kidédé Chabel Daphtone, Akoli Ekoya Ondzala, Ntsiba Honoré
Rheumatology Department, Brazzaville University Teaching Hospital, Brazzaville, Republic of Congo

Copyright © 2017 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/



Received: June 24, 2017; Accepted: August 1, 2017; Published: August 4, 2017
ABSTRACT
Objective: Report of risk factors associated to knee osteoarthritis to improve management and functional prognosis of patients. Methods and patients: Transversal and analytic survey conducted in Brazzaville University Teaching Hospital (Congo) on 13,041 patients between 2000 and 2012. The diagnosis of knee osteoarthritis was done before a mechanical knee pain and radiological signs according to Kellgren and Lawrence criterias. The functional disability has been appreciated by Lequesne functional pain rate. Results: 200 patients, 42 men (21%), 158 women (79%), sex ratio was 0.26. The average age was 57.4 years old, extremes were 25 - 82 years. The knee osteoarthritis predominated between 60 and 69 years for men (38%) and 50 - 59 years old for women (36%). Body mass index (BMI) average was 29.98 kg/m2. Co morbidities associated were arterial high blood pressure in 106 patients (53%) and diabetes mellitus (28.5%) and alcohol consumption (28%). Tobacco addiction was associated in 12%. 72.15% of women were post-menopausal, with an average length of menopause at 9.6 years. Obesity (45.5%) and overweight (35.5%) were associated with genu varum in 58.7% and genu valgum in 40.1%. Joint fluid was report in 30.5%. The functional disability evaluated by Lequesne functional pain rate was superior to 8 for more of 50% of patients. The knee osteoarthritis was mainly secondary in 81%. Conclusion: Age more than 57 years, female sex and menopause, obesity, genu varum or genu valgum, cardiovascular risk factors, were the main risk factors associated. Diagnosis was done too later and patients had an improvement functional disability.
Keywords:
Knee Osteoarthritis, Genu Valgum, Genu Varum

1. Introduction
Knee osteoarthritis is the most frequent member’s osteoarthritis in sub-Saharan Africa with an evolution to a bad functional prognosis. Knee prothetic surgery is not available in most developing countries. It leads to severe pain and disability development. Knee osteoarthritis is the first improvement after 50 years old in Africa [1] and its level prevalence is related between 33% and 50% after more than 60 years [2] . In Africa, populations socio economics’ privacy associated to the difficulties of access to quality cares, makes that patients consult too late, often at a very evolved and invalidity stages. For that, in Western and developing countries, they act before installation of distortions and invalidity. These actions begin by identification and management of risk factors associated to this invalidating osteoarthritis. So, we intended to study the most risk factors associated to the knee osteoarthritis, in order to improve management and therefore, functional prognosis of our patients.
2. Patients and Method
It was a transversal and analytic study, conducted on medical files of thirteen thousands and forty one (13,041) patients, followed in consultation and in hospitalization in rheumatology and traumatology―orthopedics’ departments of the university teaching hospital of Brazzaville in Congo, from July 2000 to July, 2012, during 12 years. Diagnosis of knee osteoarthritis has been done on clinical arguments and x-ray, when a mechanical painful of knee were notified, with or without trouble of the statics of legs and on x-ray of the knees, narrowed of cartilage, condensation of the joint surfaces and marginal osteophytis, according to Kellgren and Lawrence criterias [1] . Functional disability has been appreciated by Lequesne pain functional rate: for a score between 0 and 7, handicap was considered as means, between 8 and 10 as important, between 11 and 13 as very important and finally beyond 14 as extreme, intolerable. Surgical indication as being carried for a Lequesne score superior to 10. Two hundred patients (200) have been kept, with hospitable frequency of 8%. The software ear data version 16 permitted collections of data and software SPSS 11.5, statistical analysis. Quantitative variables have been expressed on average ± gap-type. Qualitative variables have been expressed in strength and percentage. Ethic consent was obtained by patients and the study was approved by the National Ethics Committee.
3. Results
It was about 200 patients, 42 men (21%) and 158 women (79%) with a sex ratio was 0.26. Average age was 57.4 years old, extremes of 25 and 82 years. The knee osteoarthritis predominated on men (38%) between 60 and 69 years and between 50 and 59 years old on women (36%). Forty four (44) patients (22%) were less than 50 years old at the delay of diagnosis. The average delay of consultation was 4 years and 7 months. The Body mass index (BMI) was evaluated in 191 patients. The mean BMI was 29.98 kg/m2. 68.4% of men and 81.7% of women had a BMI superior or equal to 30 kg/m2 (Table 1). The mechanical stress and traumatisms of knee were the main previous antecedents before apparition of knee osteoarthritis with respectively 73.5% and 13.5% of cases. Antecedents of inflammatory joint diseases of the knee and surgical acts represented only re-

Table 1. Breakdown of patients according to sex and body mass index.
spectively 6% and 5% of cases. About co morbidities, arterial high blood pressure was the main cardiovascular factor associated to knee osteoarthritis, found among 106 patients (53%), followed respectively by diabetes mellitus and consumption of alcohol in 28.5% and 28% of cases. The tobacco addiction was associated in 12% of cases. 114/158 women in our series (72.15%), were post menopausal at the time of knee osteoarthritis diagnosis, with an average length of menopause at 9.6 years. Pain was the main call sign. It came with a lameness in 90.5% of cases (n = 181), crunch in 87.5% (n = 175) and avoidance in 27.5% of cases (n = 55). Clinical pain location was more frequently bilateral (54%). We found a genu varum deformity in 58.7% of cases (n = 108), genu valgum in 40.1% (n = 65) and synovial fluid in 30.5% of cases (n = 61). On x-ray, lesions were bilateral in 66.5% of cases and one-sided in 33.5% of cases. According to the Kellgren and Lawrence criteria, lesions were at stage 2 in 41.5% of cases, stage 3 in 21.7% and stage 4 in 2.8% of cases. One compartment was involved in 53.7% of cases, two compartments in 38.3% and three compartments only in 6.9% of cases. The functional evaluation by Lequesne pain functional rate was more than 8 on 50% of patients. It was considered as important in 43% of cases, very important in 27% and extreme in 8% of cases. Obesity was the most factors often associated. Indeed 54.7% of obese patients had a Lequesne pain functional rate superior to 11. The knee osteoarthritis was mainly secondary. The secondary shapes represented 81% of cases against 19% of primitive knee osteoarthritis. The main etiologic factor of secondary knee osteoarthritis was axial deviations, presented on all of our patients. The other etiologic factors are represented in Figure 1.
4. Discussion
To approach the question of risk factors is a matter for process in health both preventive and curative management. Our study appears in secondary and tertiary objectives, since the patients who come in consultation already endure a knee symptomatic osteoarthritis disease, for which we must endeavor to limit progress, reduce or to warn functional handicap. Because of prothetic surgery is not available in our professional environment, reinforce more again us to need focus on the determining of risk factors and disease’s evolution. As in Togo [3] , Burkina Faso [4] and Ivory Coast [5] , the knee osteoarthritis in Congo-Brazzaville occupies a major place in rheumatology department with a hospitable frequency
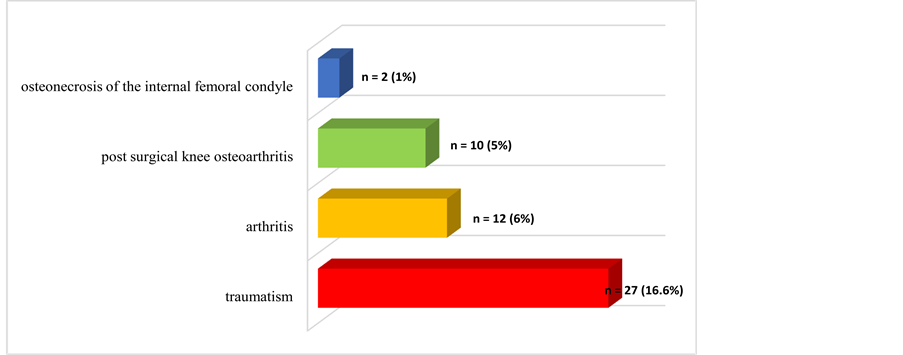
Figure 1. Breakdown of etiologic factors of secondary knee arthritis other than axial deviations.
of 8% in our series. Oniankitan et al. in Togo [3] , reported the same and testified also a lot of problem of health in our countries. It mainly interests adult old more than 50 years, regardless of sex, as well as in Africa than in Europe [4] [6] [7] . Age is an important risk factor of knee osteoarthritis [8] . The frequency of this one increases with age as been shown by Felson et al. [9] . Women are more frequently attack than men, with a statistically meaningful difference. Menopause appears to be the main factor as suggested by Ouedraogo et al. [4] and Zhang and et al. [10] . Professional activity is another risk factor of knee osteoarthritis in our study. The domestic activities and farmers are the main incriminated in sub-Saharan Africa, contributing to explain the female predominance of knee osteoarthritis in our countries, where those activities are rather devolved to the women. Cardiovascular risk factors are frequently associated to knee osteoarthritis in African reports [4] . They essentially concern arterial high blood pressure, diabetes mellitus, overweight/obesity and alcohol consumption and tobacco addiction. Relation between frequency of cardiovascular risk factors and risk to develop knee osteoarthritis has been little studied. However, if we refer to Singh and al study [11] , it seems that the populations affected by knee osteoarthritis have more cardiovascular risk factors. Indeed, they report a frequency of 40% for arterial high blood pressure, 32% for hypercholesterolemia, 20% for tobacco addiction and 11% for diabetes mellitus, compare with patients without osteoarthritis respectively in 25%, 24%, 26% and 6% of cases. Sedentary lifestyle, hyper caloric corollary diet of the obesity, itself a risk to develop diabetes mellitus and arterial high blood pressure can explain frequency of these cardiovascular risk factors in our set. Improvement of the knee osteoarthritis in our report is very important. In 72.8% of patients, it is more than to 8 according to Lequesne functional pain rate that indicates account of joint deterioration. Obesity is the most frequently factor associated. The role of obesity in the knee osteoarthritis has been established in West by many studies [12] [13] . This tie between obesity and knee osteoarthritis even persists after correction of metabolic troubles associated to the obesity [3] . If in our study, obesity appears associated with a severe handicap, like related by Ouedraogo et al. [4] , axial deviations seem to be the main factor. Their high frequency in the study, 87.4%, grants them a high level, in the evolution of the knee osteoarthritis, although it is difficult to say if they are cause or complication of it. The place of legs static troubles is very important in our series. Although we didn’t study relation between obesity, legs static deformities and functional disability, it’s likely that static disorders and obesity participate to explain the importance of joint narrowing. Although there is no clinical and radiological correlation, the low frequency of severe radiographic damage (Kellgren and Lawrence stage 4) is surprising to the view of frequency of legs axial deviations and obesity, as well as predominance in one compartmental shape, contrary to other African series [4] [6] .
5. Conclusion
Knee osteoarthritis is frequent in our practice. Patients are most often seen too late, with important joint damages associated with genu varum or genu valgum. The Lequesne functional pain rate has a high level. Age, female sex, obesity, axial legs deformities and cardiovascular risk factors were the main risk factors of knee osteoarthritis. Joint prothetic replacement is not available in our countries.
Cite this paper
Edgard, L.N.N., Chardène, M.M.P., Daphtone, N.-K.C., Ondzala, A.E. and Honoré, N. (2017) Knee Osteoarthritis and Risk Factors Associated. Open Journal of Rheumatology and Autoimmune Diseases, 7, 147-152. https://doi.org/10.4236/ojra.2017.73014
References
- 1. Richette P. (2005) Arthrosis. Revue du Praticien, 55, 1933-1942.
- 2. Bagge, E., Bjelle, A., Valkenburg, H.A. and Svanbord, A. (1992) Prevalence of Radiographic Osteoarthritis in Tow Elderly European Populations. Rheumatology Internal, 12, 33-38.
- 3. Oniankitan, O., Fianyo, E. and Mijiyawa, M. (2009) Osteoarthritis of the Knee in Hospital Outpatients in Lomé (Togo). Mali Médical, 24, 4-6.
- 4. Ouédraogo, D.D., Séogo, H., Cissé, R., Tiéno, H., Ouédraogo, T., Nacoulma, I.S. and Drabo, Y.J. (2008) Risk Factors Associated with Osteoarthritis of the Knee in a Rheumatology Outpatient Clinic in Ouagadougou, Burkina Faso. Médecine Tropicale, 68, 597-599.
- 5. Eti, E., Kouakou, H.B., Daboiko, J.C., Ouali, B., Ouattara, B., Gabla, K.A., et al. (1998) Aspects Epidemiology and Features of Knee Osteoarthritis in the Ivory Coast. Revue du Rhumatisme (English Edition), 65, 766-770.
- 6. Singwe, N.M., Emche, M.C.B., Ntsiba, H., Ongolo, Z.P., Biwole, S.M., Ndobo, P., et al. (2007) Clinical and Radiological Aspects of Knee Osteoarthritis in Yaoundé. African Journal of Medicine, 5, 317-323.
- 7. Iqbal, M.N., Haidri, F.R., Motiani, B. and Mannan, A. (2011) Frequency of Factors Associated with Knee Osteoarthritis. Pakistan Journal of Medicine Association, 61, 786-789.
- 8. Andrianakos, A.A., Kontelis, L.K., Karamitsos, D.G., Aslanidis, S.I., Georgountzos, A.I., Kaziolas, G.O., et al. (2006) Prevalence of Symptomatic Knee, Hand, and Hip Osteoarthritis in Greece. The ESORDIG study. Journal of Rheumatology, 33, 2507-2513.
- 9. Felson, D.T., Naimark, A., Anderson, J., Kazis, L., Catelli, W. and Meenan, R.F. (1987) The Prevalence of Knee Osteoarthritis in Elderly. The Framingham Osteoarthritis Study. Arthritis Rheumatism, 30, 914-918.
https://doi.org/10.1002/art.1780300811 - 10. Zhang, Y. and Jordan, J. (2010) Epidemiology of Osteoarthritis. Clinical Geriatric Medicine, 26, 355-369.
https://doi.org/10.1016/j.cger.2010.03.001 - 11. Singh, G., Miller, J.D., Lee, F.H., Pettitt, D. and Russell, M.W. (2002) Prevalence of Cardiovascular Disease Risk Factors among US Adults with Self-Reported Osteoarthritis: Data from the Third National Health and Nutrition Examination Survey. American Journal of Management Care, 8, 383-391.
- 12. Wills, A., Black, S., Cooper, R., et al. (2012) Life Course Body Mass Index and Risk of Knee Osteoarthritis at the Age of 53 Years: Evidence from the 1946 British Birth Cohort Study. Annals of Rheumatism Diseases, 71, 655-660.
https://doi.org/10.1136/ard.2011.154021 - 13. Michael, J.W.P. and Shlüter-Brust, K.U. (2010) The Epidemiology, Etiology, Diagnostic and Treatment of Osteoarthritis of the Knee. Deutsches Arzteblatt International, 107, 156-162.