Open Journal of Stomatology
Vol. 2 No. 3 (2012) , Article ID: 22658 , 3 pages DOI:10.4236/ojst.2012.23031
Modified Widman flap procedure: With or without periodontal dressing?
![]()
Department of Periodontics, School of Dentistry, Mashad University of Medical Sciences, Mashad, Iran
Email: *Mokhtarimr@mums.ac.ir
Received 18 June 2012; revised 20 July 2012; accepted 10 August 2012
Keywords: Periodontal Dressing; Periodontal Surgery; Pain
ABSTRACT
Aim: The purpose of this study was to evaluate the postoperative pain experience and gingival indexes with and without the use of periodontal dressing after Modified Widman flap procedure. Materials and Methods: Twenty patients requiring comparable bilateral flap procedures were selected. One quadrant of each jaw randomly received periodontal dressing after the surgery while the other one didn’t. Plaque Index (PI), Sulcus Bleeding Index (SBI) and Probing Depth (PD) were measured prior to the surgery, one week and 2 weeks after the surgery. Postoperative pain experience also was assessed at the conclusion of study. Results: Results showed no significant differences between dressed and undressed segments regarding changes in probing depth, plaque index or sulcus bleeding index. However patients reported significantly less pain postoperatively when the dressing was used Conclusion: Pain is reduced by periodontal dressing but No significant differences between dressed and undressed segments regarding changes in probing depth, plaque index or sulcus bleeding index.
1. INTRODUCTION
Periodontal diseases are chronic, progressive bacterial infections resulting in inflammation and destruction of tooth supporting tissues [1]. Surgical and nonsurgical procedures are used to arrest the disease process, prevent disease recurrence and regenerate lost periodontium. Nonsurgical therapy including curettage, scaling and root planing is the most common treatment for periodontitis [2-5].
Surgical therapies for treatment of sever cases of periodontal and gum diseases is used to increase access to the root surface, making it possible to remove all irritants [3,4]. Various surgical therapy techniques have been used, Modified Widman flap is one of them [5] which by a reverse bevel incision into alveolar crest makes a full access to root surface of pocket while the bone exposure is minimal.
The periodontal treatment results are influenced by several factors like prescription of antibiotics, surgical techniques and root planing frequency, among other things like application of periodontal dressing [6].
Periodontal dressings which first had been described by Ward (1923, 1929) are applied as a post-therapeutic care to cover and protect the surgical sites after some procedures such as apically repositioned flap, free gingival grafts, and non-surgical procedures [7]. Periodontal dressings can comfort patients and accelerate healing period by preventing persistent bleeding and keeping away mechanical influences during the healing phase [6]. It also prevents its detachment from the root surface by protecting the coagulum during talking and chewing [6]. However several studies reported that periodontal dressing can induce more pain and discomfort. Since there is a lack of information about periodontal dressing application after modified Widman flap procedure, our hypothesis was that the periodontal dressing reduced postoperative pain experience and enhanced gingival indexes after the mentioned procedure.
2. METHODS AND MATERIALS
In this clinical trial study 20 patients (11 females, 9 males) with the former diagnosis of generalized chronic periodontitis were selected from patients referred to Periodontology Department of MUMS dental clinic. To be included in this study, patients had to be in surgical phase and requiring comparable bilateral flap procedures. Patients with history of periodontal surgery in the 60 days previous to the experiment and those who had any systematic condition which could negatively influence oral health have been excluded from the study. Informed consent was obtained from all participants. Clinical indices such as, Silness & Löe Plaque Index, (PI), Sulcus Bleeding Index (SBI), and Probing Depth (PD) were recorded prior to the surgery. Following measurement recording and administration of local anesthesia, all sites were treated via Modified Widaman flap attempting to debrid the exposed roots and osseous defects with hand and ultrasonic instruments, the flaps repositioned and sutured using 4-0 silk sutures. After the surgery one quadrant of each jaw randomly received periodontal dressing (Coe pack, USA). One week after treatment PI and SBI and 2weeks later PD were assessed. Patients also were interviewed to rate their postoperative pain experience (on a scale that ran from 0 = no pain to 3 = sever pain). Collected data were entered into a computer and analyzed by the Statistical Package for Social Science (SPSS 15.5) software.
3. RESULTS
The average age of the subjects was 41.77 for the men and 47.54 for the women. Results showed no differences in clinical parameters between study groups (tests and controls) prior to the treatment. (P = 0.846, P = 0.756, P = 0.617 for initial probing depth, plaque index and sulculs bleeding index respectively).
No significant differences were found between dressed and undressed segments regarding changes in probing depth, plaque index or sulculs bleeding index. However patients reported significantly less pain postoperatively when the dressing was used (Table 1).
Results indicated that probing depth remarkably decreased 2 weeks after treatment (P = 0.00) in both test and control groups. There also was a significant increase in plaque index 1week after treatment with use of dressings (P = 0.042) while control group showed no significant change in terms of this parameter (P = 0.999). Significant decrease in sulcus bleeding index was found 1week after experiment in both study groups (P = 0.004 and P = 0.00 for test and control groups respectively). But No significant differences were found between dressed and undressed segments regarding changes in probing depth, plaque index or sulculs bleeding index. However patients reported significantly less pain postoperatively when the dressing was used.
4. DISCUSSION
In this study, postoperative pain was reported to be less in segments with periodontal dressing. Other clinical indices like SBI and PI after treatment were also less in test group than the control group but it was not statistically significant.
Several authors demand wound protection by a dressing after primary periodontal surgery [7-9].
Sachs and Pritchard observed advantages of periodon-
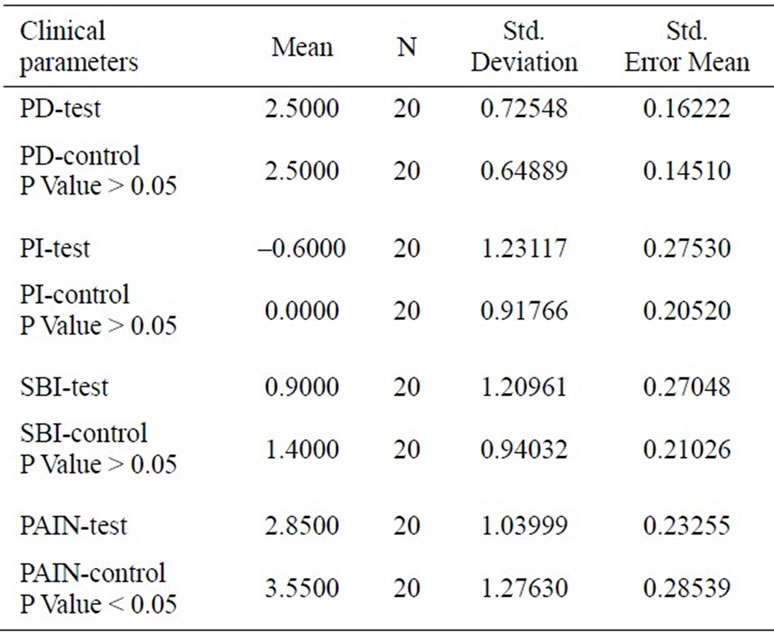
Table 1. Comparison of mean clinical parameters of study groups after treatment using Paired T Test.
tal dressing in terms of preventing persistent bleeding at healing phase following the flap surgery.
Addy et al. (1976) in a study on 21 patients requiring gingivectomies compared the effect of chlorhexidine mouthwash and periodontal dressing as post-operative treatments. They showed that the mean post-operative pocket depth for the dressing-treated segments was slightly greater than that for the mouthwash treated segments, though the difference was not clinically important [10].
Wikesjo et al. found out that periodontal dressing had effective role in pasting fibrin to root surface and inhibited penetration of epithelium to periodontal ligament space [11]. Ramfjord, Eaglstein and Plagmann mentioned that following closed curettage using periodontal dressing could yield better adaptation of buccal and lingual papilla [9,12,13] Checchi et al. stated that patients had some difficulty in eating when periodontal dressing was in their mouths. They also added that periodontal dressing provided safeguard and good psychological effect for patients [14].
The results obtained clearly demonstrate the potential importance of the application of a dressing for a stable long-term success after periodontitis surgery. However, further randomized, double-blinded, full-mouth clinical studies are necessary to confirm our results.
REFERENCES
- Pucher, J. and Stewart, J. (2004) Periodontal disease and diabetes mellitus. Current Diabetes Reports, 4, 46-50. doi:10.1007/s11892-004-0011-y
- Schluger, S., Youdelis, R., Page, R.C. and Johnson, R.H. (1990) Diseases of the periodontium. In: Periodontal Disease, Lea & Febiger, Philadelphia, 53-71.
- Newman, M.G., Takei, H., Klokkevold, P.R. and Carranza, F.A. Jr. (2002) Carranza’s clinical periodontology. 9th Edition, Saunders, Philadelphia.
- Canakçi, V., Orbak, R., Tezel, A. and Canakçi, C.F. (2003) Influence of different periodontal curette grips on the outcome of mechanical non-surgical therapy. International Dental Journal, 53, 153-158. doi:10.1111/j.1875-595X.2003.tb00740.x
- Ramfjord, S.P. and Nissle, R.R. (1974) The modified Widman flap. Journal of Periodontology, 45, 601-607. doi:10.1902/jop.1974.45.8.601
- Sigusch, B.W., Pfitzner, A., Nietzsch, T. and Glockmann, E. (2005) Periodontal dressing (Vocopac®) influences outcomes in a two-step treatment procedure. Journal of Clinical Periodontology, 32, 401-405. doi:10.1111/j.1600-051X.2005.00686.x
- Pritchard, J.F. (1972) Advanced periodontal disease. 2nd Edition, W.B. Saunders Co., Philadelphia.
- Sachs, H.A., Farnoush, A., Checchi, L. and Joseph, C.E. (1984) Current status of periodontal dressings. The Journal of Periodontology, 55, 689-696. doi:10.1902/jop.1984.55.12.689
- Plagmann, H.C. (1998) Lehrbuch der parodontologie. Hanser, München.
- Addy, M. and Dolby, A.E. (1976) The use of chlorhexidine mouthwash compared with a periodontal dressing following the gingivectomy procedure. Journal of Clinical Periodontology, 3, 59-65. doi:10.1111/j.1600-051X.1976.tb01851.x
- Wikesjö UMNu, R. (1990) Periodontal repair in dogs: Effect of wound stabilization on healing. The Journal of Periodontology, 61, 719-724. doi:10.1902/jop.1990.61.12.719
- Eaglstein, M.D. (1991) Wound dressings: Current and future. In: Barbul, A., Ed., Clinical and Experimental Approaches to Dermal and Epidermal Repair—Normal and Chronic Wounds, Wiley-Liss, New York.
- Ramfjord, S.P. (1980) Root planing and curettage. International Dental Journal, 30, 93-100.
- Checchi, L. and Trombelli, L. (1993) Postoperative pain and discomfort with and without periodontal dressing in conjunction with 0.2% chlorhexidine mouthwash after apically positioned flap procedure. Journal of Periodontology, 64, 1238-1242. doi:10.1902/jop.1993.64.12.1238
NOTES
*Corresponding author.